Fever and it's types with examples
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-sourced answer. Here is the full response:
Fever and Its Types
Definition
Fever (pyrexia) is an abnormal elevation of body temperature above the normal range (36.1-37.2°C / 97-99°F), caused by a resetting of the hypothalamic thermostat to a higher set point. It is not a disease itself but a physiological response to a perturbation of normal host physiology.
- Guyton and Hall Textbook of Medical Physiology, p. 900
- Costanzo Physiology 7th Edition, p. 184
Body Temperature Reference Ranges
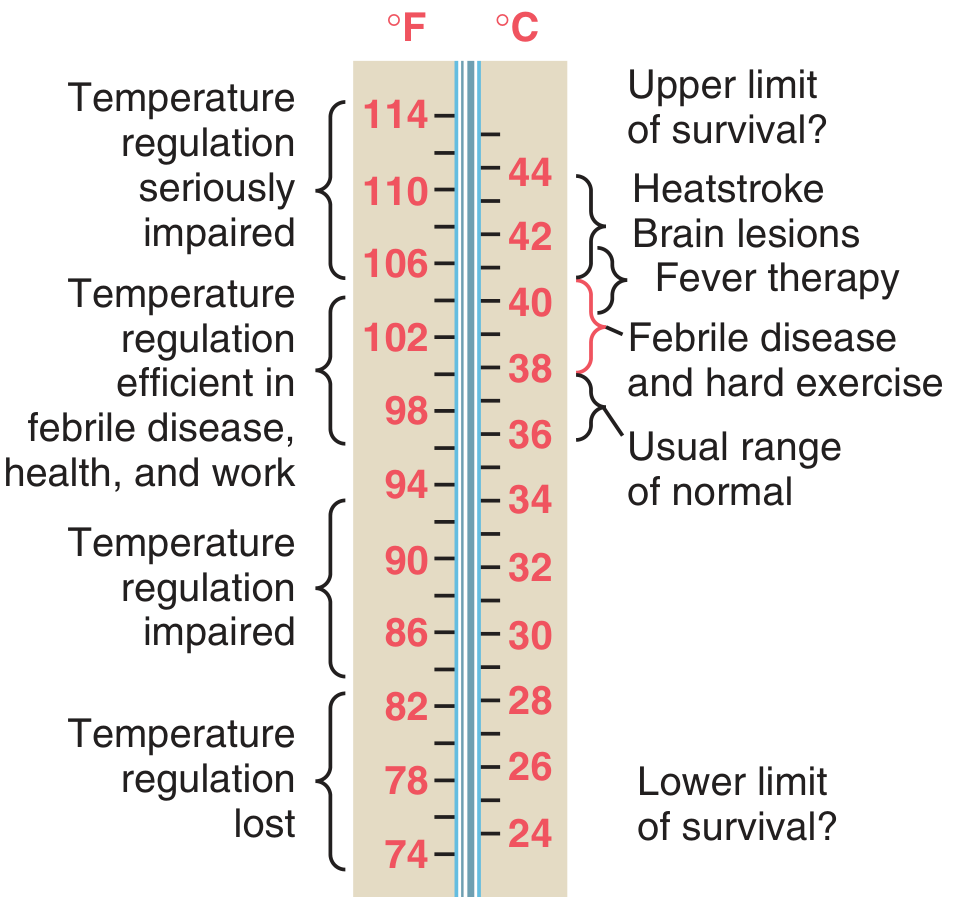
Figure: Body temperatures under different conditions (Guyton & Hall, after DuBois, 1948)
| Range | Temperature |
|---|---|
| Normal | 36.1 - 37.2°C (97 - 99°F) |
| Low-grade fever | 37.3 - 38°C |
| Fever (pyrexia) | 38 - 40°C |
| Hyperpyrexia | > 41.5°C |
Pathophysiology (How Fever Develops)
- Trigger: Bacteria, viruses, tissue breakdown products, or other stimuli activate immune cells (macrophages, leukocytes).
- Pyrogen release: These cells release cytokines, especially Interleukin-1 (IL-1) (also called endogenous pyrogen / leukocyte pyrogen), as well as TNF and IL-6.
- Hypothalamic reset: IL-1 reaches the anterior hypothalamus and stimulates local synthesis of prostaglandin E2 (PGE2), which raises the hypothalamic set-point temperature.
- Heat generation: The body activates heat-conserving and heat-generating mechanisms (vasoconstriction, shivering, piloerection = "chills") until body temperature reaches the new set point.
- Defervescence: When the cause is removed or antipyretics (e.g., aspirin, NSAIDs - which inhibit cyclooxygenase and block PGE2 synthesis) are given, the set point falls - vasodilation and sweating occur to dissipate excess heat.
- Guyton and Hall Textbook of Medical Physiology, p. 900-901
- Harrison's Principles of Internal Medicine 22E, p. 179
Classification by Temperature Degree
| Grade | Temperature (°C) | Example |
|---|---|---|
| Low-grade fever | 37.3 - 38°C | Tuberculosis (early), viral URTI |
| Moderate fever | 38 - 39°C | Influenza, pneumonia |
| High fever | 39 - 41°C | Typhoid, malaria, meningitis |
| Hyperpyrexia | > 41.5°C | Bacterial meningitis, CNS hemorrhage, heat stroke, malignant hyperthermia |
Classification by Pattern (Most Clinically Important)
Fever patterns are best understood on a temperature chart plotted over days. Each pattern has classic diagnostic associations.
1. Continuous (Sustained) Fever
- Temperature remains persistently elevated above normal throughout the day.
- Daily variation is < 1°C and the temperature does not touch normal.
- Examples: Lobar pneumonia (classical - "crisis" on day 7-10), typhoid fever (step-ladder rise then sustained), urinary tract infection, infective endocarditis.
2. Remittent Fever
- Temperature remains above normal throughout the day but fluctuates with a daily variation > 1°C.
- Temperature does not return to normal (unlike intermittent fever).
- Most common fever pattern.
- Examples: Typhoid (during active illness), bacterial pneumonia, infective endocarditis, most bacterial infections, brucellosis.
3. Intermittent Fever
- Temperature is elevated for some hours and then returns to normal (touch normal or subnormal) every day or on alternate days.
- The periodic pattern is highly diagnostically important.
Sub-types:
| Sub-type | Periodicity | Cause |
|---|---|---|
| Quotidian | Fever every day | Plasmodium falciparum malaria, double quartan malaria |
| Tertian | Fever every 3rd day (48h cycle) | Plasmodium vivax, P. ovale malaria |
| Quartan | Fever every 4th day (72h cycle) | Plasmodium malariae |
- Harrison's Principles of Internal Medicine 22E, p. 181 (Chap. 14)
"Plasmodium vivax causes fever every third day, whereas fever occurs every fourth day with Plasmodium malariae."
4. Hectic (Septic) Fever
- An exaggerated form of intermittent fever with a very wide swing (> 2-3°C between peak and trough).
- Associated with drenching sweats when the temperature drops.
- Implies bacteremia or septicemia.
- Examples: Pyemia, septicemia, liver abscess, deep-seated abscesses, infective endocarditis.
5. Relapsing Fever
- Febrile episodes lasting days to weeks, separated by afebrile periods of days to weeks, then relapsing.
Key examples:
| Pattern | Cause |
|---|---|
| Borrelia relapsing fever | Days of fever → afebrile period → relapse (Borrelia spp.) |
| Pel-Ebstein fever | Fever 3-10 days → afebrile 3-10 days → repeat cycle |
| Cyclic neutropenia | Fever every 21 days with neutropenic nadir |
"In the Pel-Ebstein pattern, fever lasting 3-10 days is followed by afebrile periods of 3-10 days; this pattern can be classic for Hodgkin disease and other lymphomas."
- Harrison's Principles of Internal Medicine 22E, p. 181
6. Periodic (Recurrent) Fever Syndromes
- Febrile episodes at predictable intervals caused by autoinflammatory diseases (not infection).
- Examples:
- Familial Mediterranean Fever (FMF): Recurrent fever + serositis (peritonitis, pleuritis)
- TRAPS (TNF receptor-associated periodic syndrome): Prolonged fever episodes
- Hyper-IgD syndrome: Periodic fever + lymphadenopathy
- PFAPA (Periodic Fever, Aphthous stomatitis, Pharyngitis, Adenitis): Seen in children
7. Biphasic (Saddle-back) Fever
- Two separate waves of fever with an afebrile gap of 1-2 days in between.
- Examples: Dengue fever (classic), poliomyelitis, yellow fever, leptospirosis, Colorado tick fever.
8. Inverse Fever (Reversed Diurnal Pattern)
- Normal physiological fever is higher in the evenings. Inverse fever is higher in the mornings (reversed pattern).
- Example: Disseminated tuberculosis (miliary TB), typhoid in some stages.
Summary Table
| Fever Type | Pattern | Classic Example |
|---|---|---|
| Continuous | Always elevated, < 1°C variation | Lobar pneumonia, typhoid |
| Remittent | Always elevated, > 1°C variation, never normal | Most bacterial infections |
| Intermittent - Tertian | Spikes every 48h, returns to normal | P. vivax malaria |
| Intermittent - Quartan | Spikes every 72h, returns to normal | P. malariae malaria |
| Hectic/Septic | Huge swings, drenching sweats | Septicemia, liver abscess |
| Relapsing (Pel-Ebstein) | Febrile 3-10 days, afebrile 3-10 days | Hodgkin's lymphoma |
| Relapsing (Borrelia) | Days fever, days afebrile, relapse | Borrelia infection |
| Saddle-back/Biphasic | 2 fever peaks with afebrile gap | Dengue fever |
| Periodic syndromes | Predictable cyclic fevers | FMF, TRAPS, PFAPA |
| Hyperpyrexia | > 41.5°C | Meningitis, CNS hemorrhage |
Important Special Categories
Fever of Unknown Origin (FUO)
Defined as fever > 38.3°C on multiple occasions, lasting > 3 weeks, with no diagnosis after 1 week of in-hospital investigation. The three major disease categories causing FUO are:
- Infectious diseases
- Autoimmune / non-infectious inflammatory disorders
- Cancer (especially lymphomas, leukemia, renal cell carcinoma)
- Harrison's Principles of Internal Medicine 22E (Disease categories presenting with fever, p. 179)
Temperature-Pulse Dissociation (Relative Bradycardia)
Normally, pulse rises ~10 bpm per 1°C rise in temperature. When pulse is inappropriately slow for the degree of fever, think of:
- Typhoid fever, brucellosis, leptospirosis, drug-induced fever, factitious fever
- Harrison's Principles of Internal Medicine 22E, p. 181
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapters 14 & 208
- Guyton and Hall Textbook of Medical Physiology, Chapter 74
- Costanzo Physiology 7th Edition, Chapter on Temperature Regulation
Pain
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-sourced answer on pain. Here it is:
Pain - Definition, Pathophysiology, and Types
Definition
The International Association for the Study of Pain (IASP) defines pain as:
"An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage."
This definition highlights two key dimensions: the sensory (physical/discriminative) component AND the affective-motivational (emotional/suffering) component. Pain is always subjective.
- Sabiston Textbook of Surgery, p. 352
Pathophysiology - The Nociceptive Process (4 Steps)
Pain begins with nociception - the neural process of encoding noxious stimuli. It has four sequential steps:
1. Transduction
- A noxious stimulus (thermal, mechanical, or chemical) is converted into an electrical signal at free nerve endings called nociceptors.
- Nociceptors are distributed in skin, muscle, fascia, joints, blood vessel walls, dura, and viscera.
- Tissue injury releases sensitizing chemicals: histamine, serotonin, bradykinin, substance P, prostaglandins, cytokines, and glutamate.
2. Transmission
- The electrical signal travels via primary afferent nerve fibers toward the CNS:
| Fiber Type | Myelination | Speed | Pain Sensation |
|---|---|---|---|
| Aβ fibers | Heavily myelinated | Fast | Innocuous touch (not primarily pain) |
| Aδ fibers | Lightly myelinated | Medium | "First pain" - sharp, well-localized, epicritic |
| C fibers | Unmyelinated | Slow | "Second pain" - burning, dull, poorly localized, protopathic |
- Aδ and C fibers are the nociceptors - they respond to high-threshold noxious stimuli.
- Signal travels to the dorsal horn of the spinal cord, then via the spinothalamic tract (anterolateral) to the thalamus and cortex.
3. Modulation
- Occurs primarily in the dorsal horn of the spinal cord (substantia gelatinosa).
- Ascending modulation: Wide dynamic range neurons (WDRNs) in the dorsal horn receive and integrate pain signals.
- Descending inhibition: From the periaqueductal gray (PAG), locus ceruleus, nucleus raphe magnus via the dorsolateral funiculus - using serotonin and norepinephrine.
- This system is activated by opioids, stress, placebo, acupuncture, and TENS.
4. Perception
- The final step - occurs when the signal reaches the cerebral cortex.
- This is where the subjective, emotional, and cognitive experience of pain is formed.
- Highly variable between individuals - influenced by psychology, past experience, context, and culture.
- Sabiston Textbook of Surgery, p. 352-353; ROSEN's Emergency Medicine, p. 92-93
Spinal Cord Pain Tracts
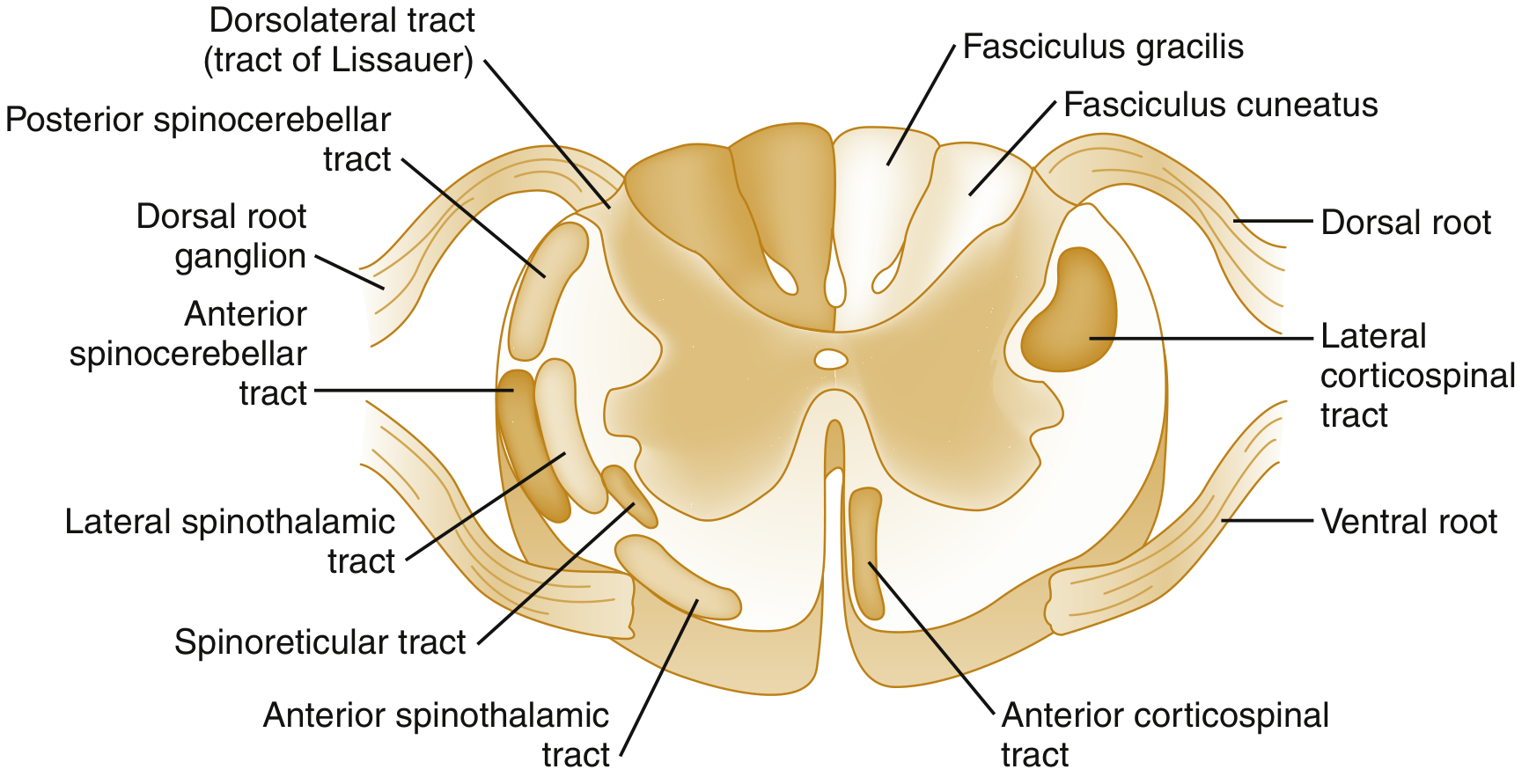
Spinal cord cross-section showing the lateral spinothalamic tract (pain and temperature) running in the anterolateral white matter - Rosen's Emergency Medicine
Classification of Pain
A. By Duration
| Type | Definition | Character |
|---|---|---|
| Acute pain | Short-duration; resolves with tissue healing | Serves a protective/survival function; associated with autonomic activation (tachycardia, hypertension, diaphoresis) |
| Chronic pain | Persists > 3 months beyond expected healing | Serves no useful function; considered a disease in itself; often not associated with autonomic signs |
- Goldman-Cecil Medicine, p. 270; Sabiston Textbook of Surgery, p. 353
B. By Mechanism (IASP Classification - Most Clinically Important)
1. Nociceptive Pain
- The most common type.
- Results from injury or disease affecting somatic structures - activation of normal nociceptors by a genuine stimulus.
- Subdivided into:
a) Somatic Pain
- Injury to skin, muscles, bones, joints.
- Well-localized, sharp initially then throbbing/aching.
- Worsened by movements that stress the injured structure (e.g., walking worsens arthritic knee pain).
- Examples: Arthritis, fracture, myofascial pain, postoperative wound pain, connective tissue disorders.
b) Visceral Pain
- Originates from internal organs (hollow viscera, capsules, mesentery).
- Characteristics differ from somatic pain:
- Poorly localized (fewer nociceptors, wide spinal cord convergence)
- Starts as burning/throbbing, associated with autonomic activation (nausea, vomiting, sweating)
- Often accompanied by referred pain to somatic areas
- Notable: viscera can be cut or burned without pain - but distension or traction causes severe pain
- Examples: Angina pectoris (ischemia → left arm/jaw pain), renal colic, appendicitis (periumbilical → RLQ), pancreatitis (epigastric → back), endometriosis.
"Periumbilical pain is often associated with appendicitis - visceral afferents travel through the celiac ganglia entering at T10, sensitizing dorsal horn at T10 → pain perceived in T10 dermatome (periumbilical)." - ROSEN's Emergency Medicine, p. 93
2. Neuropathic Pain
- Caused by a lesion or disease affecting the somatosensory system (peripheral or central nervous system).
- Accounts for 15-25% of chronic pain.
- Characterized by:
- Positive symptoms (abnormal nervous system excitability): allodynia, hyperalgesia, hyperpathia, paresthesias
- Negative symptoms (loss of neurons): sensory loss, numbness
- Descriptors: "shooting," "electrical," "burning," "stabbing" in a dermatomal or nerve distribution
Sub-types:
| Sub-type | Description | Examples |
|---|---|---|
| Peripheral neuropathic | Lesion in peripheral nerve | Diabetic peripheral neuropathy, postherpetic neuralgia (PHN), chronic post-surgical pain, phantom limb pain |
| Central neuropathic | Lesion in CNS | Central post-stroke pain, spinal cord injury pain, multiple sclerosis pain |
Key terms:
- Allodynia: Pain from a normally non-painful stimulus (e.g., light touch)
- Hyperalgesia: Exaggerated pain response to a noxious stimulus
- Hyperpathia: Abnormally painful reaction, especially to repeated stimuli
- Goldman-Cecil Medicine, p. 269-270
3. Nociplastic Pain (formerly "Central Sensitization Pain")
- Arises from altered nociception without clear tissue damage, and without somatosensory system lesion.
- No biomarkers; no demonstrable structural cause.
- Typically diffuse, widespread symptoms.
- Often coexists with: fatigue, insomnia, cognitive difficulties ("brain fog"), sensitivity to light/sound, multiple chemical sensitivities.
- Examples: Fibromyalgia, irritable bowel syndrome (IBS), tension-type headache, complex regional pain syndrome type I (CRPS-I), chronic widespread pain.
- Goldman-Cecil Medicine, p. 269
4. Mixed Pain
- More than one pain mechanism operating simultaneously.
- Examples: Cancer pain (nociceptive + neuropathic), IBS (nociplastic + visceral nociceptive), headache (tension + migraine components).
C. By Anatomic Region (Selected Examples)
| Region | Condition |
|---|---|
| Head | Migraine, tension headache, cluster headache |
| Chest | Angina, pleuritis, aortic dissection |
| Abdomen | Appendicitis, cholecystitis, pancreatitis, renal colic |
| Back | Mechanical back pain, disc herniation, spinal stenosis |
| Musculoskeletal | Arthritis, fibromyalgia, myofascial pain |
| Neuropathic | Diabetic neuropathy, PHN, trigeminal neuralgia |
Referred Pain (Special Concept)
- Viscerosomatic convergence: Spinal cord neurons receive input from both visceral AND somatic sources simultaneously, so the brain misinterprets the origin of the pain.
- Visceral pain is perceived as coming from a somatic (body surface) area.
| Organ | Where Pain is Referred |
|---|---|
| Heart (ischemia) | Left arm, jaw, neck, epigastrium |
| Diaphragm | Shoulder tip (C3-C5) |
| Appendix (early) | Periumbilical (T10) |
| Gallbladder | Right shoulder, right subscapular |
| Kidney/ureter | Groin, inner thigh |
| Aortic aneurysm | Back, flank |
- Murray & Nadel's Textbook of Respiratory Medicine, p. 886; ROSEN's Emergency Medicine, p. 93
Central Sensitization
After prolonged pain input, the CNS itself becomes hypersensitized:
- Dorsal horn neurons show wind-up (progressive amplification with repeated stimuli)
- The NMDA receptor plays a key role
- Results in allodynia and hyperalgesia extending beyond the original injury site
- Underlies the transition from acute to chronic pain and is central to nociplastic conditions
- ROSEN's Emergency Medicine, p. 93
Pain Assessment
- Visual Analogue Scale (VAS) / Numeric Rating Scale (NRS): 0-10
- Mild: 1-3, Moderate: 4-7, Severe: > 7
- A 30% or greater reduction in pain score = clinically meaningful improvement
- For non-communicating patients: facial expression scales, behavioral scales
- Always assess: location, quality, timing, aggravating/relieving factors, associated symptoms, functional impact, psychological status
- Goldman-Cecil Medicine, p. 270
Quick Reference Summary
| Feature | Somatic Pain | Visceral Pain | Neuropathic Pain | Nociplastic Pain |
|---|---|---|---|---|
| Localization | Well-localized | Poorly localized | Dermatomal/nerve distribution | Diffuse, widespread |
| Quality | Sharp → aching | Cramping/dull/burning | Shooting, electric, burning | Variable |
| Referred pain | Uncommon | Common | No | No |
| Autonomic features | Mild | Pronounced (nausea, sweating) | Absent | Absent |
| Classic example | Fracture, arthritis | Renal colic, angina | PHN, diabetic neuropathy | Fibromyalgia |
Sources:
- Goldman-Cecil Medicine International Edition, Chapter 26 (Pain: Neuropathic, Nociceptive, Nociplastic and Mixed), p. 269-270
- Sabiston Textbook of Surgery, Chapter 20 (Mechanisms of Acute Pain), p. 352-353
- Barash Clinical Anesthesia 9e, Chapter 56 (Primary Afferents), p. 4736
- ROSEN's Emergency Medicine, Chapter 6 (Pain Transmission and Modulation), p. 92-93
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 38 (Neurobiology of Pain), p. 886
Pain
I just covered Pain in detail in my previous response. Here's a quick recap of everything that was covered, and let me know if you'd like me to go deeper on any specific area:
What Was Covered
Definition
Pain = "An unpleasant sensory AND emotional experience associated with actual or potential tissue damage" (IASP)
Pathophysiology - 4 Steps of Nociception
- Transduction - Noxious stimulus → electrical signal at nociceptors
- Transmission - Via Aδ fibers (sharp/fast "first pain") and C fibers (burning/slow "second pain") → spinal cord → thalamus → cortex
- Modulation - In the dorsal horn; descending inhibition from PAG, locus ceruleus
- Perception - Subjective conscious experience in the cortex
Types by Duration
- Acute - Protective, resolves with healing
- Chronic - > 3 months, considered a disease itself
Types by Mechanism (IASP)
| Type | Cause | Examples |
|---|---|---|
| Nociceptive - Somatic | Tissue/musculoskeletal injury | Fracture, arthritis |
| Nociceptive - Visceral | Internal organ pathology | Renal colic, angina, appendicitis |
| Neuropathic | Somatosensory system lesion | Diabetic neuropathy, PHN, post-stroke pain |
| Nociplastic | Altered nociception, no tissue damage | Fibromyalgia, IBS, CRPS-I |
| Mixed | Multiple mechanisms | Cancer pain, headache |
Special Concepts
- Referred pain - Visceral pain perceived at somatic surface (e.g., heart → left arm)
- Allodynia - Pain from normally non-painful stimulus
- Hyperalgesia - Exaggerated pain to a noxious stimulus
- Central sensitization - CNS hypersensitivity; drives transition to chronic pain
Would you like me to expand on any of these topics? For example:
- Pain management / analgesic ladder
- Specific pain syndromes (migraine, neuropathic, cancer pain)
- Gate control theory
- Pain assessment tools
- Pharmacology of analgesics
Types of pain in surgery
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive surgical textbook content. Here is the full, organized answer:
Types of Pain in Surgery
Pain in surgery is encountered in two broad contexts: (1) pain as a presenting symptom that brings the patient to the surgeon, and (2) pain as a consequence of surgery (peri/postoperative pain). Both must be understood for surgical management.
I. Classification by Duration (Fundamental Surgical Distinction)
1. Acute Pain
- Pain expected to be of relatively short duration, resolving with tissue healing or withdrawal of the noxious stimulus.
- Resolves within minutes, hours, or days.
- Associated with autonomic activation: tachycardia, hypertension, tachypnea, diaphoresis.
- Has a protective/survival function - alerts to tissue injury.
- Undertreated acute pain leads to harmful pathophysiologic consequences (splinting, atelectasis, immobility, DVT, delayed recovery).
- Examples: Appendicitis pain, fracture pain, acute postoperative wound pain.
2. Chronic Pain (Persistent Surgical Pain)
- Pain persisting > 3 months beyond the expected healing period.
- Serves no useful biological function - recognized as a disease in itself.
- NOT associated with autonomic signs at rest.
- Results from peripheral sensitization, central sensitization, or nerve injury.
- Examples: Post-herniorrhaphy inguinodynia, post-mastectomy pain syndrome, phantom limb pain, failed back syndrome, chronic post-surgical pain (CPSP).
"Chronic pain serves no useful function and is now recognized as a disease itself." - Sabiston Textbook of Surgery, p. 353
II. Classification by Mechanism (Core Surgical Types)
1. Nociceptive (Somatic) Pain
- Most common type in surgery.
- Results from direct tissue injury activating nociceptors in skin, muscle, bone, fascia, and connective tissue.
- The surgical incision, dissection, and repair all cause this type.
- Quality: Initially sharp, well-localized; becomes aching/throbbing.
- Worsened by movement or stress on the anatomical structure (e.g., coughing after laparotomy, walking after hernia repair).
- Treatment: NSAIDs, paracetamol, opioids (responds well to standard analgesia).
- Examples:
- Postoperative wound pain
- Fracture pain
- Musculoskeletal trauma
- Bone metastases
- Ligamentous/muscular injury after hernia repair
"Acute postoperative pain is generally somatic, rather than visceral or neuropathic. Tissue injury leading to somatic pain activates nociceptors activated in response to physical, chemical, or heat damage." - Fischer's Mastery of Surgery 8e, p. 481
2. Visceral Pain
- Originates from internal organs (hollow viscera, solid organ capsules, mesentery, peritoneum).
- Transmitted via autonomic (sympathetic) afferents.
- Characteristics:
- Poorly localized, diffuse, cramping/colicky or dull/burning
- Associated with significant autonomic features: nausea, vomiting, sweating, pallor
- Commonly referred to somatic surface areas
- Viscera are insensitive to cutting/burning - pain is caused by distension, traction, ischemia, or chemical irritation
- Examples:
- Intestinal obstruction (colicky, periumbilical)
- Biliary colic (RUQ → right shoulder)
- Ureteric colic (loin → groin)
- Acute appendicitis - initial periumbilical visceral pain
- Mesenteric ischemia
- Post-laparoscopic shoulder-tip pain (diaphragmatic irritation from CO₂)
"Visceral pain refers to pain conveyed through afferent autonomic pain fibers. It is usually poorly localized." - Schwartz's Principles of Surgery 11e, p. 1647
3. Neuropathic Pain
- Caused by direct nerve injury, entrapment, or damage during surgery or disease.
- May appear early (immediately) or late (weeks to months post-op).
- Quality: Shooting, electrical, burning, stabbing - in a nerve or dermatomal distribution.
- Features: Allodynia (pain from light touch), hyperalgesia, paresthesias, numbness.
- Treatment: Gabapentinoids (pregabalin, gabapentin), tricyclic antidepressants, SNRIs, local nerve blocks, neurectomy for refractory cases. Responds poorly to simple NSAIDs/opioids.
- Surgical examples:
- Ilioinguinal/iliohypogastric nerve injury after inguinal hernia repair → inguinodynia
- Intercostal nerve injury after thoracotomy → post-thoracotomy pain syndrome
- Nerve injury after mastectomy → post-mastectomy pain syndrome
- Phantom limb pain (after amputation)
- Meralgia paresthetica (lateral femoral cutaneous nerve injury)
- Post-amputation stump neuroma pain
4. Mixed Pain
- Two or more mechanisms operating simultaneously - very common in surgical oncology.
- Example: Cancer pain = nociceptive (bone/soft tissue invasion) + neuropathic (nerve compression/infiltration) + visceral (organ involvement).
- Breakthrough pain: Acute, excruciating pain superimposed on stable background cancer pain - spontaneous or triggered.
III. Specific Surgical Pain Syndromes
A. Inflammatory Pain
- Caused by tissue trauma and the release of inflammatory mediators (prostaglandins, bradykinin, histamine, substance P).
- Primary hyperalgesia: Increased sensitivity at the injury site.
- Secondary hyperalgesia: Sensitization of surrounding uninjured tissue (via central sensitization).
- Underpins the rationale for pre-emptive analgesia and multimodal analgesia.
B. Ischemic Pain / Rest Pain
- Due to tissue ischemia in peripheral vascular disease.
- Claudication: Cramping pain in muscles during walking that is relieved by rest - reproducible at a similar effort level.
- Rest pain: Constant severe pain at rest (usually in foot/toes), worsened by leg elevation, relieved by dependency - indicates critical limb ischemia (Fontaine stage III).
C. Phantom Limb Pain
- Pain perceived in a limb that has been amputated.
- Caused by neuromas (disorganized axon masses at the stump) disrupting the neural efferent-afferent loop.
- Up to 85% of amputees experience phantom pain.
- Modern treatment: Targeted Muscle Reinnervation (TMR) and Regenerative Peripheral Nerve Interface (RPNI) - surgical techniques that provide trophic targets for amputated nerves, reducing neuroma formation.
D. Cancer Pain in Surgery (WHO Analgesic Ladder)
The WHO 3-step analgesic ladder guides escalation:
| Step | Pain Level | Drugs |
|---|---|---|
| Step 1 | Mild | Paracetamol, NSAIDs, tricyclics, anticonvulsants |
| Step 2 | Moderate | Weak opioids - codeine, tramadol |
| Step 3 | Severe | Strong opioids - morphine, fentanyl |
- Oral morphine: given 4-hourly, then converted to slow-release MST every 12 hours once dose is titrated.
- Breakthrough pain: Covered with short-acting opioids (morphine/fentanyl).
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 4944
IV. Chronic Post-Surgical Pain (CPSP) - Major Surgical Concern
CPSP = pain persisting > 3 months after surgery with no other explanation.
| Operation | Incidence of CPSP |
|---|---|
| Inguinal hernia repair | Up to 63% (moderate-severe in 6-8%) |
| Thoracotomy | 30-50% |
| Mastectomy | 20-30% |
| Limb amputation | 30-85% |
| General surgery | 2-10% |
Risk factors: Pre-existing pain, nerve injury, young age, female sex, psychosocial factors, poor acute pain control.
V. Summary Table
| Type | Mechanism | Quality | Localization | Example |
|---|---|---|---|---|
| Somatic (Nociceptive) | Tissue/nociceptor injury | Sharp → aching | Well-localized | Wound pain, fracture |
| Visceral | Organ distension/ischemia | Cramping/dull | Poorly localized, referred | Bowel obstruction, biliary colic |
| Neuropathic | Nerve injury/entrapment | Burning, shooting, electric | Dermatomal | Phantom limb, inguinodynia |
| Mixed | Multiple mechanisms | Variable | Variable | Cancer pain |
| Ischemic/Rest | Tissue ischemia | Cramping (claudication), severe (rest) | Muscle/foot | PAD, critical limb ischemia |
| Phantom | Neuroma + CNS | Burning, shooting | Amputated region | Post-amputation |
Sources:
- Sabiston Textbook of Surgery, Chapter 20 (Acute Pain Management), p. 352-353
- Fischer's Mastery of Surgery 8e, Postoperative Pain Management, p. 481
- Schwartz's Principles of Surgery 11e, Chapter on Hernia, p. 1647
- Bailey and Love's Short Practice of Surgery 28e, Cancer Pain, p. 4944
- Goldman-Cecil Medicine, Chapter 26 (Pain Classification), p. 269-270
This is a shared conversation. Sign in to Orris to start your own chat.