bExplain the mechanishof action, uses & side-effects of Chloroquin
Reading File
Finding Sources
Searching PubMed
chloroquine mechanism action pharmacology
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from two authoritative pharmacology textbooks. Here is the full answer:
Chloroquine - Mechanism of Action, Uses & Side Effects
Overview
Chloroquine is a synthetic 4-aminoquinoline drug developed during World War II. It was the mainstay of antimalarial therapy for decades, though its utility has declined sharply due to widespread P. falciparum resistance. It acts on erythrocytic (blood) stages of the parasite and has no activity on liver hypnozoites.
Mechanism of Action
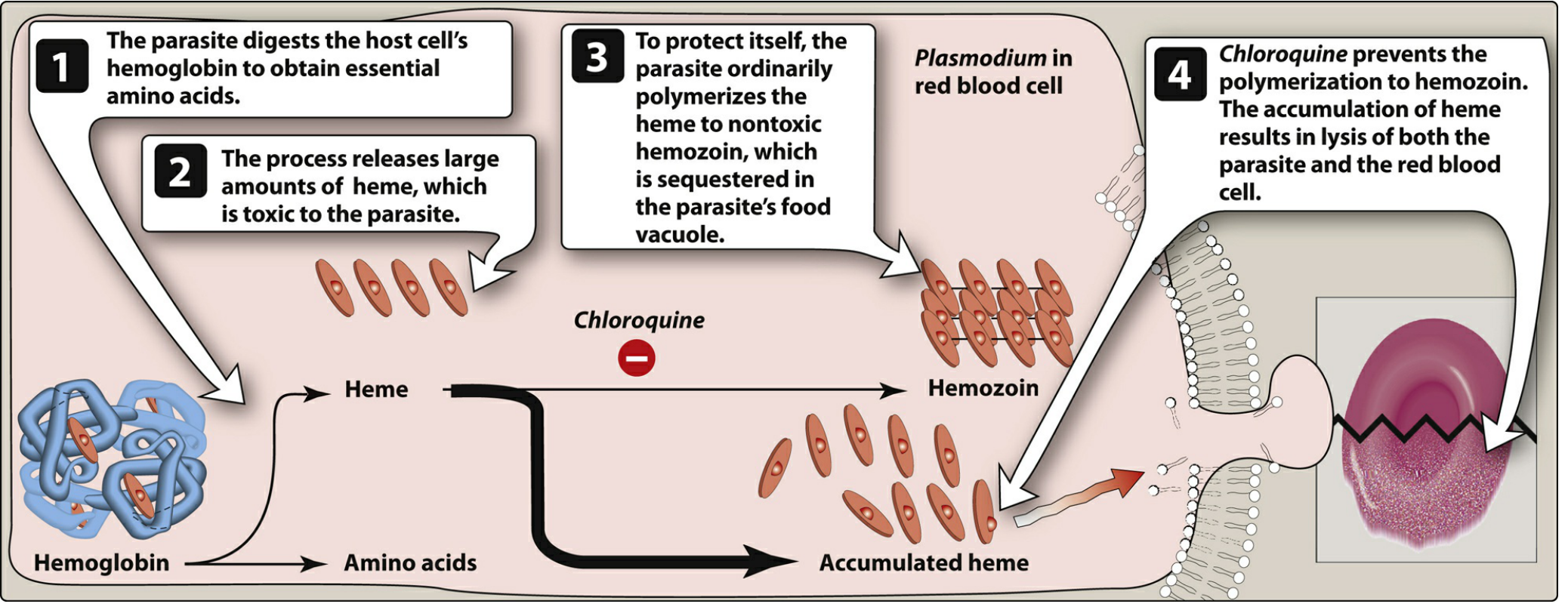
The process occurs in four steps (as shown above):
- Hemoglobin digestion - The Plasmodium parasite digests the host red blood cell's hemoglobin inside its acidic food vacuole to obtain essential amino acids.
- Toxic heme release - This digestion releases large amounts of free heme (ferriprotoporphyrin IX), which is toxic to the parasite itself.
- Normal detoxification - To protect itself, the parasite normally polymerizes free heme into an insoluble, chemically inert pigment called hemozoin, which is safely sequestered in the food vacuole.
- Chloroquine blocks this - Chloroquine, being a diprotic weak base, is concentrated in the acidic food vacuole by ion trapping. There, it specifically binds to free heme and prevents its polymerization into hemozoin. The resulting accumulation of toxic heme causes oxidative damage to parasite membranes, leading to lysis of both the parasite and the red blood cell.
The exact molecular details are not fully elucidated, but the heme-polymerization blockade is the primary accepted mechanism.
- Lippincott Illustrated Reviews: Pharmacology, p. 1171-1172
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. (block 18)
Immunomodulatory Mechanism (for non-malarial uses)
Chloroquine and its analogue hydroxychloroquine also raise the intracellular lysosomal pH, which inhibits:
- Toll-like receptor (TLR) signaling
- Antigen processing and presentation
- Pro-inflammatory cytokine production (TNF-α, IL-1, IL-6)
This accounts for its use in autoimmune diseases.
Resistance Mechanism
Resistance of P. falciparum results from mutations in the pfcrt gene (P. falciparum chloroquine resistance transporter), encoding a transporter in the food vacuole membrane that pumps chloroquine out of the vacuole. Additional modulatory transporters include PfMDR1 and PfMRP. P. vivax resistance is linked to overexpression of the pvcrt transporter.
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Rapid and complete after oral dosing; also absorbed rapidly from IM/SC sites |
| Distribution | Very large volume of distribution; concentrates in liver, spleen, kidney, lung, melanin-containing tissues, leukocytes, and erythrocytes |
| Protein binding | ~60% bound to plasma proteins |
| Metabolism | Hepatic CYP enzymes produce active metabolites: desethylchloroquine and bisdesethylchloroquine |
| Elimination | ~50% renal clearance of unchanged drug; long half-life (weeks) due to tissue sequestration |
| CNS penetration | Yes; also crosses the placenta |
Clinical Uses
1. Malaria
- Treatment of uncomplicated malaria caused by P. vivax, P. ovale, P. malariae, P. knowlesi, and chloroquine-sensitive strains of P. falciparum
- Drug of choice for P. ovale and P. malariae infections
- Prophylaxis for travelers to areas where chloroquine-sensitive malaria is still prevalent (some parts of Central America, Haiti, the Middle East)
- Standard prophylactic dose: 300 mg base (500 mg salt) orally, once weekly, beginning 1-2 weeks before travel and continued for 4 weeks after leaving the endemic area
- Note: For P. falciparum, artemisinin-based combination therapies (ACTs) have largely replaced chloroquine due to widespread resistance
2. Extraintestinal (Hepatic) Amebiasis
- Used as an adjunct for amoebic liver abscess when metronidazole is insufficient or not tolerated
3. Autoimmune / Rheumatic Diseases (mainly hydroxychloroquine)
- Rheumatoid arthritis
- Systemic Lupus Erythematosus (SLE)
- Discoid lupus
- Sjogren's syndrome (Hydroxychloroquine is generally preferred due to a safer side-effect profile)
Side Effects
At Prophylactic / Low Doses (generally well tolerated)
- GI upset: nausea, vomiting, abdominal discomfort
- Pruritus - common, especially in dark-skinned individuals
- Headache
- Blurred vision / visual disturbances
- Skin rash / urticaria
With Prolonged / High-Dose Use
| System | Side Effects |
|---|---|
| Ocular | Retinopathy (irreversible retinal damage with long-term use) - routine ophthalmologic examination required. Also: corneal deposits, blurred vision |
| Cardiac | QT interval prolongation - risk of arrhythmias; avoid co-administration with other QT-prolonging drugs. Hypotension, myocardial suppression |
| Skin | Nail bed and mucous membrane discoloration (bluish-gray) |
| Neurological | Headache; with overdose: confusion, convulsions, coma |
| GI | Nausea, vomiting, diarrhea |
Acute Overdose / Toxicity
Chloroquine has a narrow margin of safety - a single dose of ~30 mg/kg may be fatal.
- Rapid parenteral administration is especially dangerous
- Features: hypotension, vasodilation, cardiac arrhythmias, cardiac arrest
- Neurological: confusion, convulsions, coma
- Parenteral doses >5 g are usually fatal
- Management: mechanical ventilation + epinephrine + diazepam
Contraindications / Cautions
- Psoriasis - may provoke an acute attack
- Porphyria - may trigger an acute attack
- Hepatic dysfunction
- Severe GI disease
- Neurological disorders
- Pregnancy: crosses placenta (use with caution; still used when benefits outweigh risks for malaria)
Summary Table
| Aspect | Key Points |
|---|---|
| Drug class | 4-aminoquinoline |
| Main target | Erythrocytic stage of Plasmodium |
| Mechanism | Inhibits heme polymerization to hemozoin → toxic heme accumulation → parasite lysis |
| Primary uses | Malaria (sensitive strains), hepatic amebiasis |
| Serious ADRs | Retinopathy, QT prolongation, cardiotoxicity in overdose |
| Resistance | pfcrt mutations in P. falciparum |
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 1171-1174 | Goodman & Gilman's Pharmacological Basis of Therapeutics | Goldman-Cecil Medicine
bExplain the mechanishof action, uses & side-effects of Chloroquin
Reading File
Finding Sources
Searching PubMed
chloroquine pharmacology mechanism uses
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed from three authoritative textbooks. Here is a complete, well-structured answer:
Chloroquine - Mechanism of Action, Uses & Side Effects
Drug class: Synthetic 4-aminoquinoline | Prototype of: Antimalarial quinolines
1. Mechanism of Action
A. Antimalarial Mechanism (Primary)
Figure: Action of chloroquine on hemozoin formation by Plasmodium species (Lippincott Illustrated Reviews: Pharmacology, Fig. 35.7)
The mechanism proceeds in four steps within the parasite's acidic food vacuole:
| Step | What Happens |
|---|---|
| 1 | The Plasmodium parasite digests host red blood cell hemoglobin to obtain essential amino acids |
| 2 | This digestion releases large amounts of free heme (ferriprotoporphyrin IX), which is highly toxic to the parasite |
| 3 | Normally, the parasite protects itself by polymerizing free heme into insoluble, non-toxic hemozoin (malarial pigment), safely sequestered in the vacuole |
| 4 | Chloroquine - a diprotic weak base - concentrates inside the acidic food vacuole by ion trapping. It binds specifically to free heme and blocks its polymerization to hemozoin. The resulting accumulation of toxic heme causes oxidative damage to phospholipid membranes, leading to lysis of both the parasite and the RBC |
Chloroquine also raises the vacuolar pH, amplifying heme toxicity and disrupting parasite metabolism.
B. Immunomodulatory Mechanism (for autoimmune uses)
Because chloroquine is a weak base, it also accumulates in lysosomes and cytoplasmic vesicles of immune cells, raising their pH from ~4.0 to ~6.0. This lysosomotropic activity produces several anti-inflammatory effects:
- Inhibits antigen processing and presentation - macrophages and monocytes require an acidic pH for protein digestion and antigen processing; raising the pH disrupts this
- Disrupts MHC class II receptor assembly - stabilizes MHC molecules with invariant chains at higher pH, preventing displacement by autoantigens and downregulating antigen presentation
- Blocks endosomal Toll-like receptors (TLR3, 7, 8, 9) - preventing recognition of self-nucleic acids and suppressing type-I interferon production (particularly relevant in SLE)
- Reduces pro-inflammatory cytokines (TNF-α, IL-1, IL-6) from macrophages
- Stabilizes lysosomal membranes and decreases circulating immune complexes
C. Resistance Mechanism
Resistance in P. falciparum results from mutations in the pfcrt gene (P. falciparum chloroquine resistance transporter) - a transporter in the food vacuole membrane that pumps chloroquine out of the vacuole before it can act. Additional modulators include PfMDR1 (P-glycoprotein) and PfMRP. In P. vivax, resistance is linked to overexpression of the pvcrt transporter.
2. Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Rapid and complete orally; also well absorbed IM/SC |
| Distribution | Very large volume of distribution; concentrates in liver, spleen, kidney, lung, melanin-containing tissues, leukocytes, erythrocytes |
| Protein binding | ~60% |
| Metabolism | Hepatic CYPs produce active metabolites: desethylchloroquine and bisdesethylchloroquine |
| Elimination | ~50% renal; long half-life (weeks) due to deep tissue sequestration |
| Special | Penetrates the CNS; crosses the placenta |
3. Clinical Uses
Malaria
- Treatment of uncomplicated malaria due to P. vivax, P. ovale, P. malariae, P. knowlesi, and chloroquine-sensitive P. falciparum
- Drug of choice for P. ovale and P. malariae
- Chemoprophylaxis for travelers to areas with proven chloroquine-sensitive malaria (parts of Central America, Haiti, the Middle East)
- Dose: 300 mg base (500 mg salt) orally once weekly, starting 1-2 weeks before travel, continuing 4 weeks after return
- Note: For P. falciparum, artemisinin-based combination therapies (ACTs) have largely replaced chloroquine due to near-universal resistance
Non-malarial Uses
- Hepatic (extraintestinal) amebiasis - used as adjunct or when metronidazole is insufficient
- Rheumatoid arthritis - disease-modifying (DMARD) via immunomodulatory mechanism (hydroxychloroquine preferred)
- Systemic Lupus Erythematosus (SLE) - reduces flares, protects against organ damage
- Discoid lupus erythematosus
- Sjogren's syndrome
4. Adverse Effects
At Low / Prophylactic Doses (generally mild)
- GI upset: nausea, vomiting, abdominal pain, diarrhea
- Pruritus - common, especially in dark-skinned individuals
- Headache
- Blurred vision / visual disturbances
- Urticaria / skin rash
With Prolonged or High-Dose Use
| System | Adverse Effect |
|---|---|
| Ocular | Retinopathy (irreversible, dose-cumulative) - routine ophthalmologic monitoring required; corneal deposits |
| Cardiac | QT interval prolongation - risk of arrhythmias; avoid combination with other QT-prolonging drugs |
| Skin/Mucosa | Bluish-gray discoloration of nail beds and mucous membranes on chronic use |
| Neurological | Headache, dizziness; psychosis with prolonged use |
| Blood | Hemolysis in G6PD-deficient patients |
Acute Overdose / Toxicity
Chloroquine has a narrow margin of safety - a dose of ~30 mg/kg can be fatal; parenteral doses >5 g are usually fatal.
- Cardiovascular: Hypotension, vasodilation, suppressed myocardial function, arrhythmias, cardiac arrest
- CNS: Confusion, convulsions, coma
- Management: Mechanical ventilation + epinephrine + diazepam
Contraindications / Cautions
- Psoriasis - may provoke acute exacerbation
- Porphyria - may trigger acute attack
- Hepatic dysfunction (use with caution)
- Severe GI or neurological disorders
- G6PD deficiency (risk of hemolysis)
- Avoid concurrent QT-prolonging drugs
Quick Reference Summary
| Aspect | Key Point |
|---|---|
| Class | 4-aminoquinoline |
| Target stage | Erythrocytic (blood) stages of Plasmodium |
| Core mechanism | Blocks heme polymerization to hemozoin → toxic heme accumulates → parasite lysis |
| Immune mechanism | Raises lysosomal pH → inhibits TLR signaling, antigen presentation, cytokine release |
| Primary indication | Chloroquine-sensitive malaria; SLE/RA (HCQ preferred) |
| Most serious ADRs | Retinopathy (chronic), QT prolongation, fatal cardiotoxicity (overdose) |
| Key resistance gene | pfcrt mutations in P. falciparum |
Sources: Lippincott Illustrated Reviews: Pharmacology, pp. 1171-1174 | Goodman & Gilman's Pharmacological Basis of Therapeutics | Firestein & Kelley's Textbook of Rheumatology
Write the treatment of severe and complicated falciparum malaria.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"severe malaria" treatment guidelines artesunate
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from Harrison's (2025), Goldman-Cecil, Tintinalli's Emergency Medicine, and Park's Textbook. Here is the complete answer:
Treatment of Severe and Complicated Falciparum Malaria
Severe malaria is a medical emergency with mortality ranging from 15-20% even with optimal treatment, and up to 20-50% in cerebral malaria. Immediate, aggressive treatment is life-saving.
Criteria for Severe/Complicated Falciparum Malaria
A patient qualifies as having severe malaria if one or more of the following are present:
| Feature | Threshold |
|---|---|
| Impaired consciousness / coma (cerebral malaria) | GCS impaired |
| Repeated generalized convulsions | ≥2 seizures in 24 h |
| Renal failure | Serum creatinine >3 mg/dL |
| Jaundice | Serum bilirubin >3 mg/dL |
| Severe anaemia | Hb <5 g/dL |
| Pulmonary oedema / ARDS | Radiological or clinical |
| Hypoglycaemia | Plasma glucose <40 mg/dL |
| Metabolic acidosis | Bicarbonate <15 mmol/L |
| Circulatory collapse / shock | Systolic BP <80 mmHg (adults); <50 mmHg (children) |
| Abnormal bleeding / DIC | Spontaneous bleeding |
| Haemoglobinuria (blackwater fever) | Dark urine |
| Hyperthermia | Temperature >42°C (106°F) |
| Hyperparasitaemia | >5% parasitized RBCs in low-endemic; >10% in hyperendemic areas |
Note: Microscopy may be negative in severe infection due to sequestration. A strongly suspected case should be treated immediately without waiting for confirmation.
General Principles
- Admit to ICU - severe malaria requires intensive nursing care and close monitoring
- Start parenteral antimalarial therapy immediately - do not delay for lab confirmation
- Identify and treat all complications simultaneously
- Switch to oral therapy as soon as the patient can tolerate it (after minimum 24 h parenteral treatment)
- In endemic areas, also start broad-spectrum antibiotics empirically because bacterial co-infection/sepsis cannot be excluded clinically
Specific Antimalarial Treatment
First-Line: IV Artesunate (Drug of Choice)
IV artesunate has replaced quinine as the global standard of care for severe falciparum malaria based on landmark trials showing:
- 35% lower mortality than quinine in Southeast Asian adults (SEAQUAMAT trial)
- 22.5% reduction in mortality vs. quinine in African children (AQUAMAT trial)
Dosing:
- 2.4 mg/kg IV (or IM) on admission (time = 0)
- Then at 12 h and 24 h
- Then once daily until patient can take oral medication
Advantages over quinine:
- No cardiac toxicity (does not cause QT prolongation)
- No hypoglycemia
- Kills all erythrocytic stages (early ring forms to late trophozoites)
- Much faster parasite clearance (significant reduction within 12 h vs. 24-48 h with quinine)
Special notes:
- In children weighing <20 kg: dose is 3 mg/kg (higher weight-adjusted dose)
- In artemisinin-resistant areas (parts of Southeast Asia, East Africa): give artesunate plus quinine together at full doses
- Pre-referral rectal artesunate (10 mg/kg) can be given as a bridging measure in rural areas before IV access is available - shown to reduce mortality in children
Second-Line: Parenteral Quinine (if artesunate unavailable)
Dosing:
- Loading dose: 20 mg of quinine salt/kg by slow IV infusion over 4 hours (or divided IM injection)
- Maintenance dose: 10 mg/kg 8-hourly (infused over 2-8 h); infusion rate must not exceed 5 mg/kg/hour
- Do NOT give the loading dose if the patient has already received quinine or mefloquine in the previous 24 hours
Toxicities to monitor:
- Hypoglycemia (stimulates insulin secretion) - check blood glucose frequently
- QT prolongation / cardiac arrhythmias
- Cinchonism: tinnitus, high-tone hearing loss, nausea, headache
Third Option: Artemether (IM)
- 3.2 mg/kg IM stat on admission, then 1.6 mg/kg/day IM
- Oil-based formulation; absorption is more erratic than artesunate
- Does not confer the same survival benefit as IV artesunate
- Used when IV access is unavailable and artesunate is not on hand
Step-Down to Oral Therapy
Once the patient can tolerate oral medication (after minimum 24 hours of parenteral treatment), complete treatment with:
After IV Artesunate:
- Full 3-day course of oral ACT (artemisinin-based combination therapy)
- Artemether-lumefantrine (AL) - preferred in first trimester pregnancy
- Artesunate-amodiaquine
- Dihydroartemisinin-piperaquine (DHA-PPQ)
- Artesunate-mefloquine (in Southeast Asia)
- Add single-dose primaquine 0.25 mg/kg as gametocytocide (to block transmission) - safe even in G6PD deficiency at this low dose; contraindicated in pregnancy
After IV Quinine:
- Quinine 10 mg/kg TDS + Doxycycline 100 mg OD (or 3 mg/kg in children) for 7 days total (including parenteral days)
- In pregnant women and children <8 years: replace doxycycline with Clindamycin 10 mg/kg 12-hourly
- Alternatively, complete with area-specific ACT
Summary Treatment Algorithm
SEVERE FALCIPARUM MALARIA SUSPECTED
↓
Confirm with RDT / thick blood smear (do NOT delay treatment)
↓
IV ARTESUNATE 2.4 mg/kg at 0h, 12h, 24h → then OD
[If unavailable: IV Quinine 20 mg/kg loading → 10 mg/kg 8-hrly]
↓
Minimum 24 h parenteral treatment
↓
Patient tolerating oral medications?
YES → Full 3-day oral ACT course + single-dose primaquine
NO → Continue parenteral up to maximum 7 days
Supportive Management of Complications
| Complication | Management |
|---|---|
| Cerebral malaria (coma) | Nurse in lateral position; maintain airway; no high-dose steroids, mannitol, or dextran (proven harmful); anticonvulsants for seizures (benzodiazepines) |
| Hypoglycaemia | IV 50% dextrose bolus → 10% dextrose infusion; monitor glucose 4-hourly (especially with quinine); extra vigilance in pregnancy |
| Severe anaemia (Hb <5 g/dL) | Blood transfusion; target Hb >8 g/dL |
| Acute renal failure | Early haemofiltration or haemodialysis; avoid nephrotoxic drugs; correct fluid balance carefully |
| Pulmonary oedema / ARDS | Nurse at 45°; restrict fluids; mechanical ventilation if needed; high PEEP |
| Seizures | IV benzodiazepines (diazepam, lorazepam); avoid high-dose phenobarbital (shown harmful in trials) |
| Shock / circulatory collapse | Cautious fluid resuscitation (beware pulmonary oedema); vasopressors if needed; treat co-existing bacterial sepsis with IV antibiotics |
| DIC / Coagulopathy | Fresh frozen plasma (FFP), platelets; treat underlying infection |
| Hyperpyrexia >39°C | Paracetamol (do not use aspirin); tepid sponging; fans |
| Haemoglobinuria | Maintain adequate urine output; watch for renal failure |
Treatments Proven Ineffective or Harmful (DO NOT USE):
- High-dose glucocorticoids (steroids)
- Urea
- Heparin
- Dextran
- Desferrioxamine
- Anti-TNF-α antibodies
- High-dose phenobarbital (20 mg/kg)
- Large-volume albumin boluses
- Routine exchange transfusion
Special Populations
Pregnancy
- Artemisinin derivatives are safe in all trimesters and preferred over quinine
- Quinine increases the risk of hypoglycaemia in pregnancy and should be avoided if possible
- Do NOT give primaquine in pregnancy
- Artemether-lumefantrine is the preferred ACT in first trimester
Children
- Artesunate dose: 3 mg/kg for children <20 kg
- Clindamycin replaces doxycycline (doxycycline contraindicated <8 years)
- Pre-referral rectal artesunate is particularly valuable
Artemisinin Resistance (Southeast Asia / East Africa)
- Parasites show slow clearance (half-life >5 h; clearance >3 days)
- Give artesunate + quinine together at full doses
- Triple ACT combinations (e.g., artesunate + mefloquine + piperaquine) under evaluation
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025) | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine | Park's Textbook of Preventive and Social Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics
Jmmunosuppression in organ transplantation
Reading File
Finding Sources
Finding Sources
Searching PubMed
immunosuppression organ transplantation
Pharmacotherapy of Jmmunosuppression in organ transplantation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the complete answer:
Pharmacotherapy of Immunosuppression in Organ Transplantation
General Principles of Transplant Immunosuppression
Organ transplantation immunosuppression is organized around five core principles:
- HLA matching - Select the best ABO blood type-compatible, HLA-matched donor
- Multitier therapy - Use several agents simultaneously, each at a different molecular target. Synergistic effects allow lower doses of each drug, limiting toxicity while maximizing efficacy
- Induction + Maintenance - Greater immunosuppression is needed early (induction) to prevent acute rejection; maintenance doses are then reduced over time as the risk of rejection falls and drug toxicity risks rise
- Investigate graft dysfunction - Every episode must be evaluated for rejection, drug toxicity, recurrence of original disease, or infection (these can coexist)
- Dose reduction - Reduce or withdraw a drug when its toxicity exceeds its benefit
Sites of Action (Overview)
| Drug | Site/Mechanism of Action |
|---|---|
| Glucocorticoids | Glucocorticoid response elements in DNA (gene transcription) |
| Cyclosporine | Calcineurin - inhibits phosphatase activity |
| Tacrolimus | Calcineurin - inhibits phosphatase activity |
| Azathioprine | DNA - false nucleotide incorporation |
| Mycophenolate mofetil | Inosine monophosphate dehydrogenase (IMPDH) |
| Sirolimus / Everolimus | mTOR - blocks cell cycle G1→S progression |
| Belatacept | CD80/CD86 costimulatory ligands on APCs |
| Alemtuzumab | CD52 on B cells, T cells, macrophages, NK cells |
| Basiliximab / Daclizumab | IL-2 receptor (CD25) α chain |
| Muromonab-CD3 | T-cell receptor complex |
Phase 1: Induction Therapy
Used at the time of transplantation to prevent early acute rejection. About 70% of de novo transplant patients receive biological induction agents. Induction allows delay of nephrotoxic calcineurin inhibitors (CNIs) and intensifies early protection in high-risk patients (repeat transplants, presensitized patients, African Americans, pediatric patients).
A. Depleting Agents
These agents remove (deplete) recipient T lymphocytes at the time of antigen presentation.
1. Antithymocyte Globulin (ATG / Thymoglobulin) - Most Widely Used
- Polyclonal antibody (rabbit or equine) against human thymocytes
- Depletes CD3+ T cells from circulation
- Two FDA-approved preparations:
- Lymphocyte Immune Globulin (Atgam) - equine derived
- Antithymocyte Globulin (Thymoglobulin) - rabbit derived (more commonly used)
- Side effects: fever, chills, cytokine release syndrome; give glucocorticoids to blunt first-dose reactions; increased risk of infection and post-transplant lymphoproliferative disorder (PTLD)
2. Alemtuzumab (Campath-1H) - off-label in transplantation
- Humanized anti-CD52 monoclonal antibody
- CD52 is expressed widely on B cells, T cells, macrophages, and NK cells
- Produces prolonged lymphocyte depletion
- FDA-approved for CLL and MS; increasingly used off-label as induction in kidney, pancreas, and other organ transplants
3. Muromonab-CD3 (OKT3) - largely historical
- Murine anti-CD3 monoclonal antibody that blocks the T-cell receptor complex
- First-dose cytokine release syndrome is a major adverse effect
- Discontinued in the US; replaced by better-tolerated agents
B. Immune Modulators (Non-depleting)
Anti-IL-2 Receptor Monoclonal Antibodies
Do not deplete T cells; instead block IL-2-mediated T-cell activation by binding to the α chain (CD25) of IL-2R:
- Basiliximab (chimeric - 33% mouse/67% human)
- Daclizumab (humanized - withdrawn from market in some regions)
- Well tolerated; no cytokine storm; used in low-to-moderate immunological risk
C. For Antibody-Mediated (Humoral) Rejection
- Plasmapheresis - removes circulating anti-HLA antibodies
- Intravenous Immunoglobulin (IVIG) - immunomodulatory
- Rituximab - chimeric anti-CD20 mAb; depletes B lymphocytes
Phase 2: Maintenance Therapy
Standard triple therapy: Calcineurin inhibitor + Antiproliferative agent + Glucocorticoid
I. Calcineurin Inhibitors (CNIs) - BACKBONE of Maintenance
Mechanism (both drugs share the same final pathway):
The Plasmodium → T-cell activation pathway:
- TCR activation → rise in intracellular Ca²⁺
- Ca²⁺ activates calcineurin (a phosphatase)
- Calcineurin dephosphorylates NFAT (Nuclear Factor of Activated T-cells)
- Dephosphorylated NFAT translocates to nucleus → activates transcription of IL-2, IL-4, and other lymphokines
- IL-2 drives T-cell proliferation and activation of cytotoxic T lymphocytes
CNIs block step 3 by binding to immunophilins and forming drug-immunophilin-calcineurin complexes.
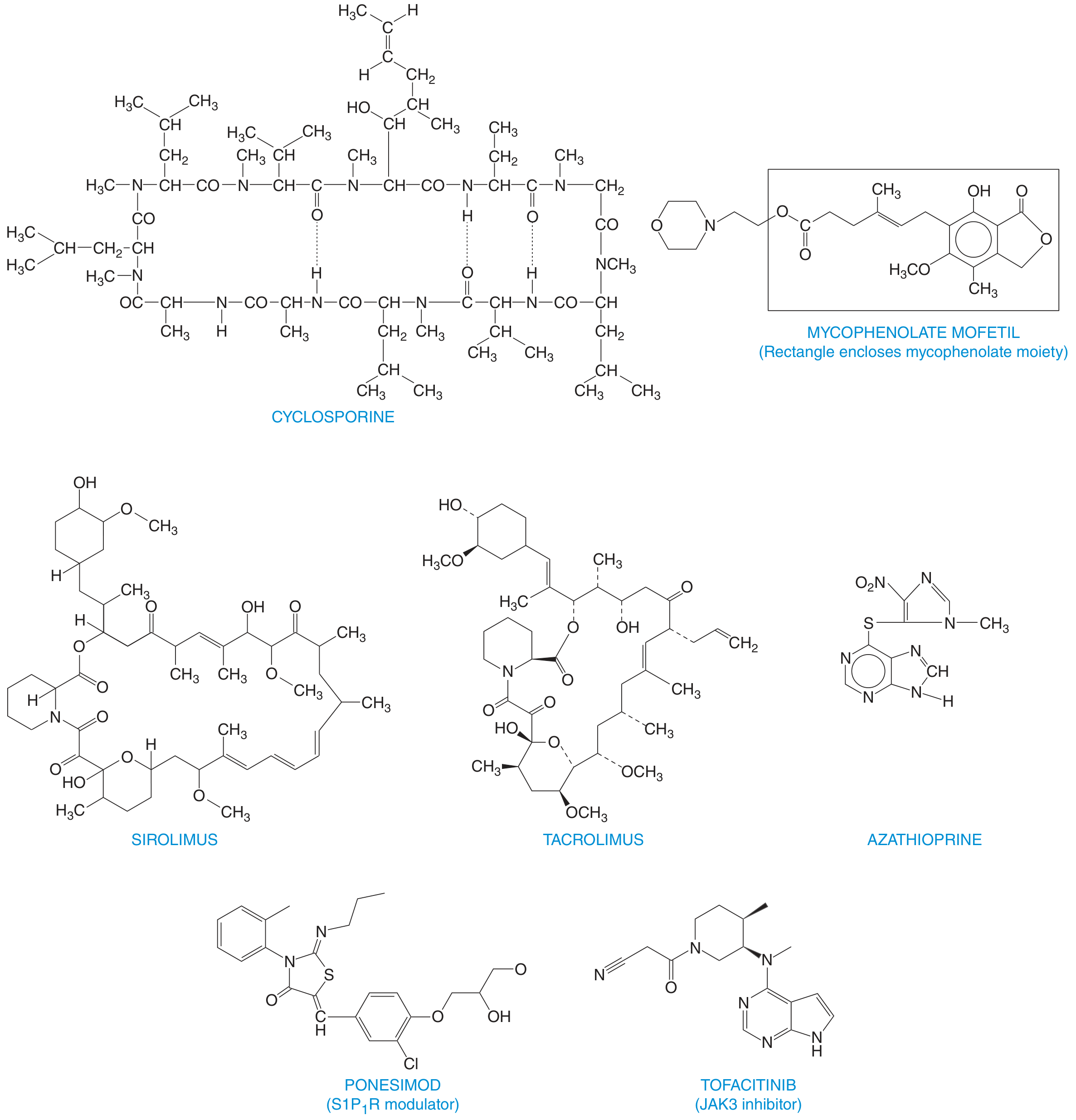
A. Tacrolimus (FK506) - PREFERRED CNI in most centers
| Feature | Detail |
|---|---|
| Source | Macrolide produced by Streptomyces tsukubaensis |
| Binds to | FKBP-12 (immunophilin) |
| Complex formed | Tacrolimus-FKBP-12-Ca²⁺-calmodulin-calcineurin → inhibits calcineurin phosphatase → prevents NFAT dephosphorylation → blocks IL-2 transcription |
| Formulations | Oral capsules (IR and ER), IV solution (5 mg/mL) |
| Monitoring | Whole blood trough levels: 10-15 ng/mL (early); 6-8 ng/mL at 3 months |
| Metabolism | Hepatic CYP3A4/3A5; excreted in feces |
| t½ | ~12 h |
| Initial dose | Kidney: 0.2 mg/kg/day; Liver: 0.1-0.15 mg/kg/day; Heart: 0.075 mg/kg/day (in two divided doses) |
Adverse effects:
- Nephrotoxicity (acute and chronic interstitial fibrosis)
- Neurotoxicity: tremor, headache, insomnia, seizures
- Diabetogenicity - new-onset diabetes after transplant (NODAT)
- Hypertension, hyperkalemia
- Does NOT cause gingival hyperplasia or hirsutism (unlike cyclosporine)
- Alopecia and diarrhea (especially with MMF)
Drug interactions: Metabolized by CYP3A4 - major interactions with azole antifungals, macrolides, rifampin, diltiazem. Do NOT combine with cyclosporine or sirolimus (additive nephrotoxicity).
B. Cyclosporine (Cyclosporin A) - older CNI, still used
| Feature | Detail |
|---|---|
| Source | Cyclic polypeptide of 11 amino acids from fungus Beauveria nivea |
| Binds to | Cyclophilin (immunophilin) |
| Complex formed | Cyclosporine-cyclophilin → binds calcineurin → inhibits NFAT dephosphorylation → blocks IL-2 and other lymphokine gene transcription |
| Formulations | Original: Sandimmune (20-50% bioavailability); Microemulsion: Neoral/Gengraf (better bioavailability). NOT interchangeable without monitoring |
| Protein binding | ~90% |
| Metabolism | Hepatic CYP3A4 |
Adverse effects (more than tacrolimus):
- Nephrotoxicity - dose-limiting; acute (reversible vasoconstriction) and chronic (irreversible striped interstitial fibrosis)
- Hirsutism (hypertrichosis)
- Gingival hyperplasia
- Hypertension
- Hyperlipidemia (raises LDL and cholesterol)
- Hyperuricemia / gout
- Hepatotoxicity
- Neurotoxicity
Drug interactions: CYP3A4 substrate - same interactions as tacrolimus. Also inhibited by grapefruit juice.
II. Antiproliferative / Antimetabolic Agents
A. Mycophenolate Mofetil (MMF) - PREFERRED antiproliferative
| Feature | Detail |
|---|---|
| Class | Prodrug → hydrolyzed to Mycophenolic Acid (MPA) |
| Mechanism | MPA is a selective, noncompetitive, reversible inhibitor of IMPDH (inosine monophosphate dehydrogenase), a key enzyme in the de novo pathway of guanine nucleotide synthesis. B and T lymphocytes rely almost exclusively on this pathway (lacking the salvage pathway that other cells use). Result: selective inhibition of lymphocyte proliferation, antibody formation, cell adhesion, and migration |
| Dose | 1-3 g/day orally in two divided doses |
| Metabolism | MMF → MPA (active) → MPAG (inactive glucuronide, enterohepatic recycled) |
Adverse effects:
- GI toxicity: nausea, vomiting, diarrhea, abdominal pain (dose-limiting)
- Bone marrow suppression: leukopenia, anemia, thrombocytopenia
- Increased susceptibility to infections (especially CMV)
- Increased risk of malignancy (especially skin cancer)
- Teratogenic - strict contraception required
B. Azathioprine - older alternative to MMF
| Feature | Detail |
|---|---|
| Class | Purine antimetabolite; imidazolyl derivative of 6-mercaptopurine |
| Mechanism | Converted to 6-mercaptopurine → further to 6-thio-GTP, which is incorporated into DNA as a fraudulent nucleotide → inhibits de novo purine synthesis → inhibits lymphocyte proliferation |
| Dose | 1-5 mg/kg/day |
| Peak levels | Within 1-2 h of oral dose |
Adverse effects:
- Bone marrow suppression - leukopenia (most common), thrombocytopenia, anemia
- Increased infection risk (especially VZV, HSV)
- Hepatotoxicity
- Alopecia, GI toxicity, pancreatitis
- Increased risk of malignancy
Key drug interaction: Allopurinol blocks xanthine oxidase (the enzyme that catabolizes azathioprine metabolites) → toxic accumulation → reduce azathioprine dose by 75% or avoid combination.
III. mTOR Inhibitors (Proliferation Signal Inhibitors)
A. Sirolimus (Rapamycin)
| Feature | Detail |
|---|---|
| Source | Macrocyclic lactone from Streptomyces hygroscopicus (Easter Island) |
| Mechanism | Binds FKBP-12 (same as tacrolimus) → but the complex does NOT inhibit calcineurin. Instead it binds and inhibits mTOR (mechanistic target of rapamycin), a key protein kinase in cell cycle progression → blocks G1 → S phase transition in T-cell proliferation (downstream of IL-2 receptor signaling) |
| Monitoring | Whole blood levels: 5-15 ng/mL |
| Metabolism | CYP3A4 and P-glycoprotein; t½ ~62 h (long!) |
| Bioavailability | ~15%; take consistently with or without food |
Therapeutic uses:
- Prophylaxis of organ rejection (usually combined with reduced-dose CNI + glucocorticoids)
- CNI-sparing regimens to preserve renal function in patients with CNI nephrotoxicity
- Drug-eluting stents (inhibits local intimal proliferation)
- LT (liver transplant) patients with HCC to reduce tumor recurrence
Adverse effects:
- Hyperlipidemia (dose-dependent - cholesterol + triglycerides) - requires treatment
- NOT directly nephrotoxic - but worsens renal function when combined with cyclosporine
- Impaired wound healing (avoid in early post-op period)
- Lymphocele (increased in renal transplant)
- Oral ulcers / stomatitis, mucositis
- Pneumonitis (interstitial lung disease)
- Anemia, leukopenia, thrombocytopenia
- Proteinuria (avoid if GFR <30% or existing proteinuria)
B. Everolimus
- Hydroxylated derivative of sirolimus; same mechanism via FKBP-12 → mTOR inhibition
- Better oral bioavailability than sirolimus
- Approved for kidney and liver transplantation
- Similar adverse effect profile to sirolimus
IV. Glucocorticoids
Used in all phases (induction, maintenance, and treatment of established rejection).
Mechanism:
- Bind intracellular glucocorticoid receptors → regulate gene transcription
- Curtail NF-κB activation
- Suppress pro-inflammatory cytokines: IL-1, IL-6
- Inhibit T cells from producing IL-2 and proliferating
- Inhibit cytotoxic T lymphocyte activation
- Reduce chemotaxis and lysosomal enzyme release from neutrophils/monocytes
- Broad anti-inflammatory effects - relatively little effect on humoral immunity
Clinical use in transplantation:
- Part of maintenance triple therapy (at low dose)
- High-dose "pulse" steroids (methylprednisolone IV) to treat established acute rejection
- Pretreat before ATG infusion to blunt cytokine release syndrome
- Early steroid withdrawal protocols are increasingly used (especially in pediatric patients) to reduce long-term morbidity
Adverse effects (long-term):
- Growth retardation in children
- Avascular necrosis of bone
- Osteoporosis / osteopenia
- Hyperglycemia / diabetes
- Hypertension
- Cataracts
- Poor wound healing, increased infection risk
- Cushingoid features
V. Belatacept - Costimulation Blockade
| Feature | Detail |
|---|---|
| Class | Selective T-cell costimulation blocker |
| Mechanism | Fusion protein (CTLA-4 + IgG) that binds CD80 and CD86 on antigen-presenting cells (APCs), blocking the CD28 costimulatory signal required for full T-cell activation. Without this "second signal," T cells become anergic |
| Route | IV infusion |
| Use | Prophylaxis of rejection in kidney transplant recipients (especially in CNI-intolerant patients) |
| Advantage | Avoids CNI nephrotoxicity; better renal function preservation long-term |
| Disadvantage | Increased risk of PTLD (post-transplant lymphoproliferative disorder), especially in EBV-seronegative recipients |
Phase 3: Treatment of Established Rejection
| Type | Treatment |
|---|---|
| Acute cellular rejection | High-dose pulse steroids (IV methylprednisolone 500-1000 mg/day × 3 days) |
| Steroid-refractory acute rejection | Polyclonal ATG / antilymphocyte globulin |
| Antibody-mediated (humoral) rejection | Plasmapheresis + IVIG ± rituximab (anti-CD20) ± bortezomib |
| Chronic rejection | Optimization of maintenance immunosuppression; mTOR inhibitors |
Standard Triple Maintenance Regimen
Tacrolimus (CNI)
+
Mycophenolate Mofetil (antiproliferative)
+
Prednisolone (glucocorticoid)
Each drug targets a different step in T-cell activation, allowing synergistic immunosuppression at lower individual doses.
Complications of Long-term Immunosuppression
| Category | Specific Complication |
|---|---|
| Infections | Bacterial (early), CMV/EBV/VZV/fungal (intermediate), opportunistic including PCP (long-term) |
| Malignancy | Skin cancers (squamous >> basal cell); PTLD (EBV-associated lymphoma); Kaposi's sarcoma |
| Metabolic | NODAT (new-onset diabetes), dyslipidemia, hypertension, obesity (metabolic syndrome) |
| Renal | CNI nephrotoxicity; chronic allograft nephropathy |
| Cardiovascular | Leading cause of late death in transplant recipients |
| Bone | Osteoporosis, avascular necrosis |
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics | Bailey and Love's Short Practice of Surgery, 28th Ed. | Roitt's Essential Immunology | Katzung's Basic and Clinical Pharmacology | Sabiston Textbook of Surgery | Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.