Expanded new ballard score
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete overview of the Expanded New Ballard Score (ENBS), sourced from the Textbook of Family Medicine 9e and The Harriet Lane Handbook 23e.
Expanded New Ballard Score (ENBS)
Reference: Ballard JL, Khoury JC, Wedig K, et al. New Ballard Score, expanded to include extremely premature infants. J Pediatr. 1991;119:417-423.
Overview
The ENBS is a standardized tool for estimating gestational age (GA) in newborns based on two domains: neuromuscular maturity and physical maturity. It was expanded from the original Ballard score to include extremely premature infants (as early as 20 weeks). It is most accurate when performed at approximately 24 hours of life. If the GA by exam differs from GA by dates/ultrasound by more than 1 week, the earlier GA should be used.
Scores range from -10 to +50, corresponding to 20-44 weeks of gestation.
Part 1: Neuromuscular Maturity
Each criterion is scored from -1 to 5. With increasing maturity, muscle tone and flexion increase.
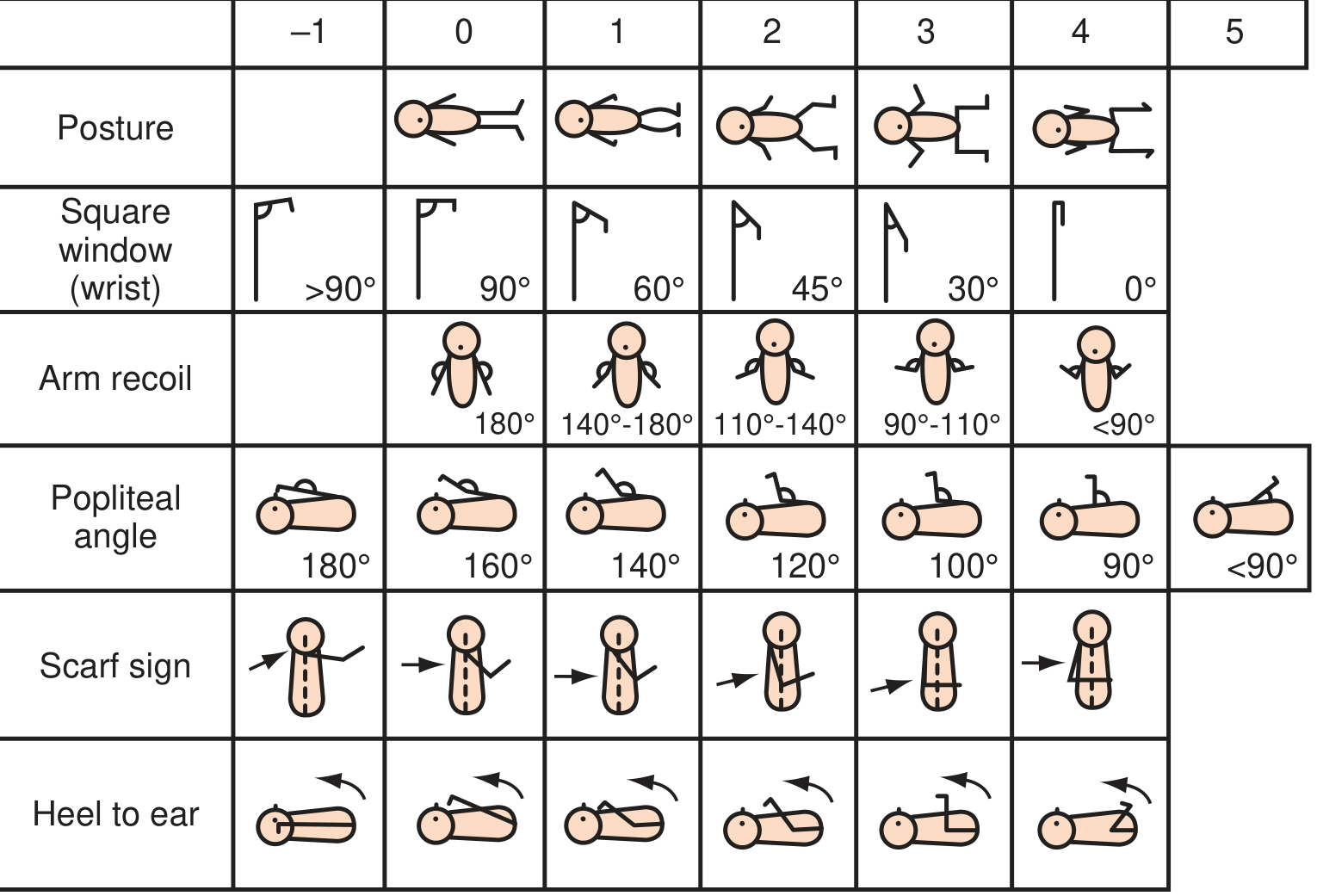
| Criterion | How to Assess | Score increases with... |
|---|---|---|
| Posture | Observe infant quiet and supine | 0 = arms/legs extended; 4 = full flexion of all limbs |
| Square Window (wrist) | Flex hand on forearm; measure wrist angle | >90° (score 0) → 0° (score 5) |
| Arm Recoil | Flex forearms 5 sec, extend fully, release | 180° (score 0) → <90° (score 4) |
| Popliteal Angle | Hip fully flexed, extend knee gently; measure angle | 180° (score -1) → <90° (score 5) |
| Scarf Sign | Pull arm across neck toward opposite shoulder | Past opposite axillary line (score 0) → cannot reach midline (score 3) |
| Heel to Ear | Draw foot toward head without forcing; observe distance | Maximum distance (premature) → foot touches ear/head (term+) |
Part 2: Physical Maturity
Each criterion scored from -1 (most premature) to 4-5 (post-term).
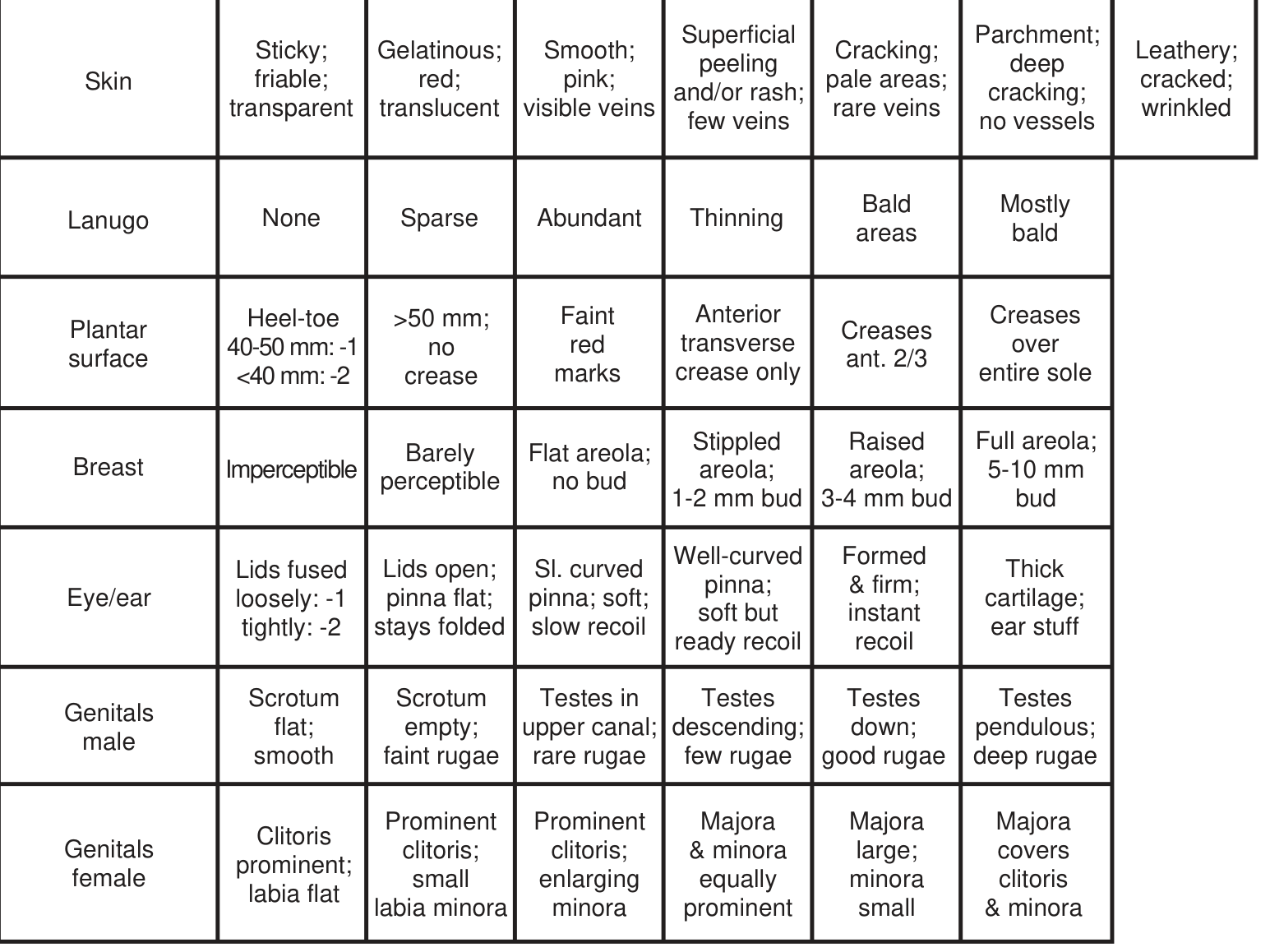
| Criterion | Premature (-1 to 0) | Term (3-4) | Post-term (5) |
|---|---|---|---|
| Skin | Sticky, friable, transparent | Cracking, pale areas, rare veins | Leathery, cracked, wrinkled |
| Lanugo | None (very preterm) → sparse | Bald areas | Mostly bald |
| Plantar Surface | Heel-toe <40 mm; no crease | Creases over anterior 2/3 | Creases over entire sole |
| Breast | Imperceptible | Raised areola, 3-4 mm bud | Full areola, 5-10 mm bud |
| Eye/Ear | Lids fused tightly (-2) | Formed & firm pinna, instant recoil | Thick cartilage, ear stiff |
| Genitalia (Male) | Scrotum flat, smooth | Testes down, good rugae | Testes pendulous, deep rugae |
| Genitalia (Female) | Clitoris prominent, labia flat | Majora large, minora small | Majora covers clitoris & minora |
Part 3: Maturity Rating (Score to Gestational Age)
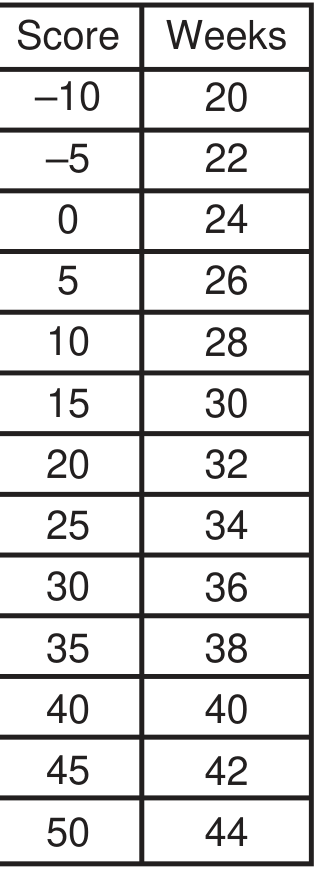
| Total Score | Gestational Age (weeks) |
|---|---|
| -10 | 20 |
| -5 | 22 |
| 0 | 24 |
| 5 | 26 |
| 10 | 28 |
| 15 | 30 |
| 20 | 32 |
| 25 | 34 |
| 30 | 36 |
| 35 | 38 |
| 40 | 40 |
| 45 | 42 |
| 50 | 44 |
Each 5-point increment in score = 2 weeks of gestational age.
Key Clinical Points
- Best timing: ~24 hours after birth (neuromuscular tone stabilizes, but before edema distorts physical signs).
- Accuracy: ±2 weeks; more reliable earlier in gestation when combined with obstetric history.
- Expanded range: The "expanded" part refers to inclusion of scores as low as -10 (for 20-week micropreemies), which the original 1979 Ballard score did not cover.
- Limitations: Sedated, paralyzed, or critically ill neonates may have artificially low neuromuscular scores. Obstetric dating (LMP/ultrasound) remains the gold standard when available.
- SGA/LGA context: After GA is estimated, plot weight, length, and head circumference on growth charts to classify the infant as SGA (<10th percentile), AGA (10th-90th), or LGA (>90th percentile).
Sources: Textbook of Family Medicine 9e, p. 527-528; The Harriet Lane Handbook 23e, p. 645
This is a shared conversation. Sign in to Orris to start your own chat.