Mi
It looks like your message got cut off! Could you finish your thought? I'm here to help.
MI
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete, textbook-sourced breakdown of the types of Myocardial Infarction.
Types of Myocardial Infarction (MI)
MI is classified in two complementary ways: (1) the ECG-based clinical classification used at the bedside to guide immediate treatment, and (2) the Universal Definition etiological classification (Types 1-5) based on the underlying mechanism.
Part 1 - ECG-Based Clinical Classification (ACS Subtypes)
This is how MIs are differentiated in the emergency setting. The broader term Acute Coronary Syndrome (ACS) encompasses three entities:
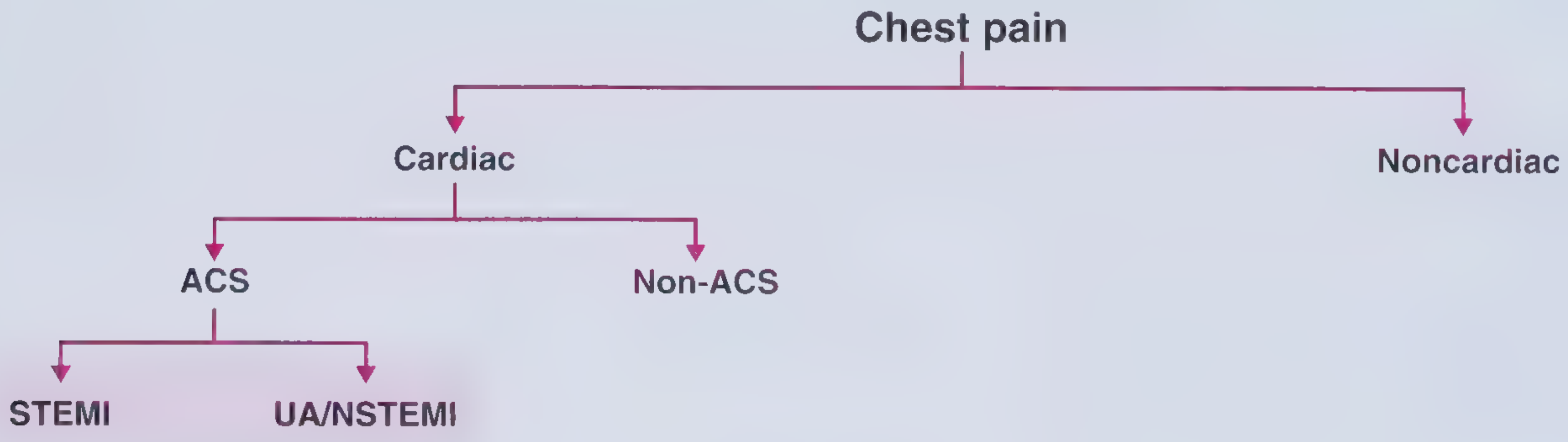
| Subtype | ECG | Biomarkers | Key Point |
|---|---|---|---|
| STEMI | ST-segment elevation in ≥2 contiguous leads | Elevated troponin | Full-thickness (transmural) occlusion; needs immediate reperfusion |
| NSTEMI | ST depression, T-wave changes, or no ECG changes | Elevated troponin | Partial occlusion or supply-demand mismatch |
| Unstable Angina (UA) | ST depression or T-wave changes | Normal (no necrosis) | Ischemia without infarction |
STEMI Diagnostic Criteria (ECG)
New ST-segment elevation at the J point in ≥2 contiguous leads:
- ≥0.2 mV in men ≥40 years in leads V2-V3
- ≥0.25 mV in men <40 years in leads V2-V3
- ≥0.15 mV in women in leads V2-V3
- ≥0.1 mV in all other leads
Why distinguish STEMI from UA/NSTEMI? Because immediate reperfusion therapy (primary PCI or fibrinolytics) is specifically beneficial in STEMI. Treatment strategies differ fundamentally. - Frameworks for Internal Medicine, p. 33
Part 2 - Universal Definition: Types 1-5 (Etiological Classification)
This classification, from the 4th Universal Definition of MI (Thygesen et al., 2018, JACC), identifies the underlying cause of the infarction.
Type 1 - Spontaneous MI
- Mechanism: Atherosclerotic plaque rupture, ulceration, fissuring, erosion, or dissection → intraluminal thrombus → reduced coronary blood flow or distal platelet emboli → myocyte necrosis.
- The patient usually has underlying CAD, but occasionally no obstructive CAD is found.
- This is the "classic" heart attack.
Type 2 - MI Secondary to Ischemia Imbalance
- Mechanism: A condition other than CAD causes an imbalance between myocardial oxygen supply and demand. There is no acute atherothrombosis.
- Causes include: coronary artery spasm, coronary embolism, coronary endothelial dysfunction, tachyarrhythmia, bradyarrhythmia, anemia, respiratory failure, hypotension, hypertension with LVH.
- Example: a patient with severe anemia or sepsis-induced tachycardia developing troponin elevation.
Type 3 - MI Resulting in Death Before Biomarkers Are Available
- Cardiac death with symptoms of myocardial ischemia and presumed new ischemic ECG changes (or new LBBB), but death occurs before blood samples could be obtained or before troponin could rise.
- Biomarkers were either unavailable or not collected.
Type 4a - MI Related to PCI
- Defined by cTn elevation >5× the 99th percentile URL (in patients with normal baseline) occurring within 48 hours of PCI.
- Must also have at least one of: symptoms, new ischemic ECG changes/LBBB, angiographic loss of patency, or new wall motion abnormality on imaging.
Type 4b - MI Related to Stent Thrombosis
- Detected by coronary angiography or autopsy in the setting of ischemia + rise/fall of cardiac biomarkers, with at least one value above the 99th percentile URL.
- Occurs in the context of a previously placed coronary stent.
Type 5 - MI Related to CABG
- Defined by cTn elevation >10× the 99th percentile URL (in patients with normal baseline) within 48 hours of surgery.
- Must also have: new pathologic Q waves or new LBBB, or angiographically documented new graft/native artery occlusion, or imaging evidence of new myocardial loss.
Summary Table
| Type | Mechanism | Setting |
|---|---|---|
| 1 | Plaque rupture/erosion → thrombus | Spontaneous (classic MI) |
| 2 | Supply-demand mismatch, no thrombosis | Secondary to another illness |
| 3 | Presumed ischemia; death before biomarkers | Out-of-hospital cardiac death |
| 4a | PCI-related injury | Post-procedure (cTn >5× URL) |
| 4b | Stent thrombosis | In-stent occlusion |
| 5 | CABG-related injury | Post-surgery (cTn >10× URL) |
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Box 48.3, p. 1778 (4th Universal Definition of MI)
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - p. 2161
- Frameworks for Internal Medicine - p. 33 (ACS subtypes and ECG criteria)
Trauma assesment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer.
Trauma Assessment
Trauma assessment follows three guiding principles (ATLS):
- Treat the greatest threat to life first
- The lack of a definitive diagnosis must never delay indicated treatment
- A detailed history is not essential to begin evaluation
Phase 1: Pre-Arrival Preparation
Before the patient arrives, the ED team should:
- Receive EMS handover: mechanism of injury, suspected injuries, vital signs, treatments given
- Assign roles to team members
- Prepare resuscitation and procedural equipment
- Ensure surgical consultants are available
- Consider whether immediate transfer to a trauma center is needed
Phase 2: Primary Survey (ABCDE)
The goal is to rapidly identify and manage immediately life-threatening injuries, treating each problem as it is found before moving to the next step.
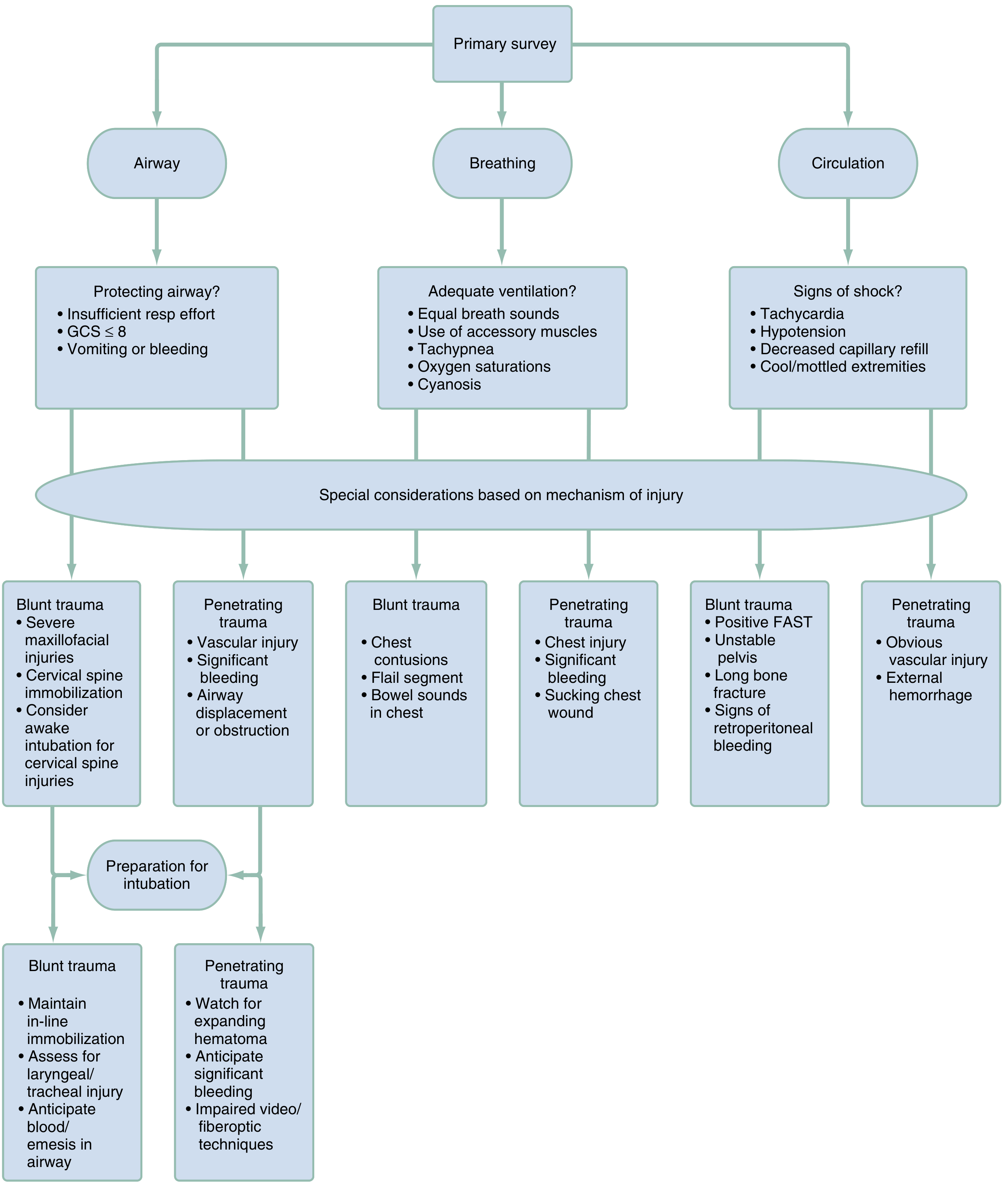
A - Airway (with Cervical Spine Protection)
- Assess, clear, and protect the airway (jaw thrust/chin lift, suctioning)
- Indicators for intubation: GCS ≤8, insufficient respiratory effort, vomiting or bleeding into airway
- Perform endotracheal intubation with in-line cervical stabilization
- Create a surgical airway if significant bleeding/obstruction or laryngoscopy cannot be performed
- Blunt trauma: maintain in-line immobilization; assess for laryngeal/tracheal injury
- Penetrating trauma: watch for expanding hematoma, anticipate significant bleeding
B - Breathing
- Ventilate with 100% O₂; monitor SpO₂
- Auscultate both lung fields; inspect thorax and neck
- Look for: deviated trachea, open chest wounds, abnormal chest wall motion, crepitus
- Immediate interventions:
- Tension pneumothorax → needle thoracostomy
- Hemopneumothorax → tube thoracostomy
- Flail chest, sucking chest wound → urgent management
- Blunt trauma clues: chest contusions, flail segment, bowel sounds in chest
- Penetrating trauma clues: chest injury, significant bleeding, sucking chest wound
C - Circulation
- Assess volume status: skin color, capillary refill, pulse quality (radial/femoral/carotid), BP
- Signs of shock: tachycardia, hypotension, decreased capillary refill, cool/mottled extremities
- Place two large-bore peripheral IV catheters
- Begin rapid infusion of warm crystalloid if indicated
- Apply direct pressure to external bleeding sites
- Central venous or intraosseous access if peripheral sites unavailable
- Pericardiocentesis for suspected cardiac tamponade
- Blunt trauma clues: positive FAST, unstable pelvis, long bone fracture, retroperitoneal bleeding
- Penetrating trauma clues: obvious vascular injury, external hemorrhage
D - Disability (Neurological Status)
- Pupil size and reactivity
- Limb strength and movement, grip strength
- GCS score and orientation
- Check capillary blood glucose in any patient with altered mental status
E - Exposure
- Completely disrobe the patient; inspect for burns and toxic exposures
- Logroll the patient (maintaining neutral spine and in-line neck stabilization) to inspect and palpate: thoracic spine, flank, back, and buttocks
- Prevent hypothermia (warm blankets, warm IV fluids)
Phase 3: Secondary Survey (Head-to-Toe Examination)
Done only after the primary survey is complete and the patient is stabilized. The goal is rapid identification and control of all other injuries.
| Region | Key Assessment | Critical Findings |
|---|---|---|
| General | Level of consciousness, GCS | GCS ≤8, focal motor deficit |
| Head | Pupils, contusions, lacerations | Herniation syndrome, open skull fracture, CSF leak |
| Battle's sign, raccoon eyes, hemotympanum | Basal skull fracture | |
| Face | Midface instability, malocclusion, conjunctiva | Airway obstruction from bleeding, facial/mandible fractures |
| Neck | Penetrating injury, tracheal deviation, JVD, subcutaneous emphysema, hematoma | Carotid injury, cardiac tamponade, tracheal/laryngeal fracture, vascular injury |
| Chest | Respiratory effort, rib tenderness, breath sounds, paradoxical movement | Impending respiratory failure, flail chest, tension pneumothorax, hemothorax |
| Abdomen | Distension, tenderness, penetrating injuries | Intraabdominal hemorrhage |
| Pelvis | Pelvic stability | Pelvic fracture, retroperitoneal bleed |
| Perineum | Lacerations, hematoma, urethral blood | Urethral/bladder injury |
| Extremities | Pulses, deformities, open fractures | Vascular compromise, compartment syndrome |
| Spine | Midline tenderness (thoracic) | Spinal fracture/dislocation |
Cervical Spine Imaging Decision: NEXUS Criteria
C-spine imaging can be omitted if ALL 5 criteria are met:
- No posterior midline cervical spine tenderness
- No evidence of intoxication
- Alert mental status
- No focal neurologic deficits
- No painful distracting injuries
Failure to meet any one criterion = imaging required.
Key Adjuncts During Primary Survey
| Tool | Purpose |
|---|---|
| FAST (Focused Abdominal Sonography in Trauma) | Rapid bedside detection of free intraperitoneal/pericardial fluid |
| Chest X-ray | Pneumothorax, hemothorax, mediastinal widening |
| Pelvic X-ray | Pelvic ring disruption |
| 12-lead ECG | Cardiac contusion, arrhythmia |
| ABG / Labs | Lactate, base deficit (marker of hemorrhagic shock) |
Sources:
- Rosen's Emergency Medicine, 9th Ed. - Primary Survey, Table 32.2 (Secondary Survey), Fig. 32.4
- Tintinalli's Emergency Medicine: A Comprehensive Study - Table 25A-3 (Primary and Secondary Survey in Trauma Resuscitation), NEXUS Criteria
This is a shared conversation. Sign in to Orris to start your own chat.