Gross features of lobular carcinoma of breast
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is a detailed response on the gross features of lobular carcinoma of the breast, drawn from authoritative textbook sources:
Gross Features of Invasive Lobular Carcinoma of the Breast
Invasive lobular carcinoma (ILC) is the most common "special type" of breast cancer, accounting for 10-15% of all invasive breast carcinomas.
1. Ill-Defined / Poorly Demarcated Borders
The single most characteristic gross feature of ILC is its lack of distinct margins. Unlike invasive ductal carcinoma (IDC), which typically forms a firm, stellate mass with obvious borders, ILC tends to infiltrate the breast parenchyma insidiously, blending imperceptibly into surrounding normal breast tissue. This makes the tumor borders poorly circumscribed and difficult to identify on both gross inspection and imaging.
- Robbins Basic Pathology: "...a significant subgroup invade without producing a desmoplastic response; such tumors may be clinically occult and difficult to detect by imaging."
- Schwartz's Surgery: "invasive lobular carcinoma varies from clinically inapparent carcinomas to those that replace the entire breast with a poorly defined mass."
2. Minimal or Absent Desmoplasia
ILC classically produces minimal desmoplasia (fibrous stromal reaction). This contrasts sharply with IDC, which induces a pronounced fibrous response producing its characteristic gritty, hard feel. Because ILC lacks this reaction, the tumor:
- Does not form the firm, chalky-white, gritty mass typical of IDC
- May feel only slightly firmer than normal breast tissue
- Is radiologically subtle and often underestimated in size on mammography
3. Clinical Spectrum - From Occult to Large
The gross appearance spans a wide range:
| Presentation | Description |
|---|---|
| Clinically inapparent | Some ILCs produce no palpable mass and are invisible on standard imaging |
| Palpable mass | When palpable, presents as a vague, rubbery thickening rather than a hard lump |
| Diffuse replacement | In advanced cases, the entire breast may be replaced by tumor with no discrete mass visible |
4. Multifocal, Multicentric, and Bilateral Tendency
A defining gross feature of ILC is its strong propensity to be:
- Multifocal - multiple tumor foci within the same quadrant
- Multicentric - foci in more than one quadrant of the same breast
- Bilateral - approximately 4-5% of women with breast cancer have bilateral primaries, and this rate is higher with lobular carcinoma
This diffuse, "spread-out" pattern reflects the biology of the tumor cells, which lose E-cadherin expression and therefore lose cohesion, spreading individually through the stroma rather than forming compact nodules.
5. Consistency and Color
When a discrete mass is present, it is typically:
- Rubbery to firm in consistency (not the hard, gritty quality of IDC)
- Gray-white in color on cut section
- Without the chalk-streak calcifications often seen in high-grade IDC with DCIS
6. Why ILC Looks This Way - Molecular Basis
The gross features are a direct consequence of loss of E-cadherin (encoded by CDH1). E-cadherin is a transmembrane adhesion protein that normally holds epithelial cells together. Its loss (through CDH1 mutation or methylation) causes:
- Dyscohesive cells that infiltrate individually rather than forming cohesive nests
- No mass effect, no desmoplasia, no necrosis
- The characteristic "single-file" (Indian-file) linear invasion pattern microscopically
Germline CDH1 mutations also predispose to lobular breast carcinoma and diffuse gastric (signet-ring cell) carcinoma.
Histological Hallmark (for context)
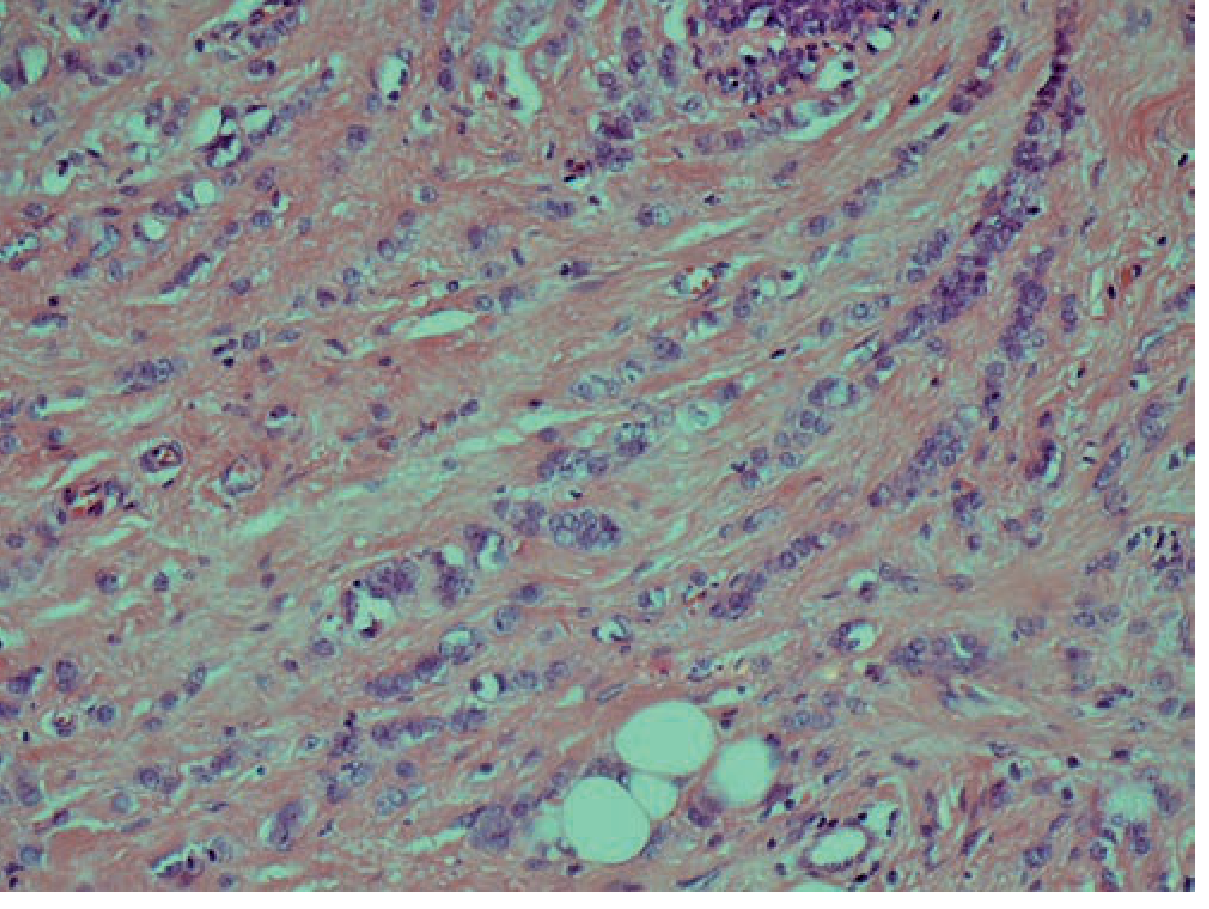
Lobular carcinoma cells arranged in single-file ("Indian file") orientation, infiltrating through a fibrous stroma. (Schwartz's Surgery, Fig. 17-17)
The dyscohesive tumor cells invade stroma individually and align in linear single-file cords ("Indian file" pattern). Some cells contain intracytoplasmic mucin, which may displace the nucleus to form signet-ring cells.
Pattern of Spread (Clinically Relevant)
ILC has a unique metastatic pattern, favoring:
- Peritoneum and retroperitoneum
- Gastrointestinal tract (especially stomach, simulating linitis plastica)
- Ovaries and uterus
- Leptomeninges (carcinomatous meningitis)
- Bone marrow
- CSF
This contrasts with IDC, which tends to metastasize to lung, liver, and bone.
Summary Table
| Feature | Invasive Lobular Carcinoma | Invasive Ductal Carcinoma |
|---|---|---|
| Borders | Ill-defined, insidious | Irregular but more defined |
| Desmoplasia | Minimal or absent | Prominent |
| Palpable mass | Often absent or vague | Usually distinct, hard |
| Consistency | Rubbery/firm | Hard, gritty |
| Calcifications | Rare | Common (with DCIS) |
| Bilaterality | High | Lower |
| Multifocal/multicentric | Common | Less common |
| Mammographic detection | Difficult (underestimates size) | Usually detectable |
Sources:
- [Robbins Basic Pathology](Robbins Basic Pathology, 17th ed., p. 715) - Morphology section
- [Robbins, Cotran & Kumar Pathologic Basis of Disease](Robbins, Cotran & Kumar, 10th ed.) - Invasive Carcinoma, Morphology
- [Schwartz's Principles of Surgery 11e](Schwartz's Principles of Surgery, p. 594) - Invasive Lobular Carcinoma section
- [Mulholland & Greenfield's Surgery 7e](Mulholland & Greenfield's Surgery) - Histologic Subtype and Tumor Grade
This is a shared conversation. Sign in to Orris to start your own chat.