Pituitary hypothelemic system drugs from lippincot
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the core content. Let me compile the complete answer from what I've gathered from Lippincott Illustrated Reviews Pharmacology, Chapter 23.
Pituitary-Hypothalamic System Drugs
Source: Lippincott Illustrated Reviews - Pharmacology, Chapter 23
Overview
The hypothalamus connects the nervous system to the endocrine system via the pituitary gland. It releases releasing or inhibitory hormones that travel via portal circulation to the anterior pituitary, triggering or suppressing hormone secretion. This axis regulates virtually all physiologic processes.
II. HYPOTHALAMIC AND ANTERIOR PITUITARY HORMONES
A. Growth Hormone (GH) and Related Drugs
Physiology: GH is released from the anterior pituitary under control of:
- GHRH (Growth Hormone-Releasing Hormone) - stimulates release
- Somatostatin - inhibits release
GH acts on the liver to produce IGF-1 (Insulin-like Growth Factor-1), which mediates most of GH's anabolic effects. GH also has direct lipolytic effects.
1. Somatropin (Humatrope, Genotropin) - GH Replacement
| Feature | Detail |
|---|---|
| Type | Recombinant human GH |
| Indications | GH deficiency in children and adults, Turner syndrome, Prader-Willi syndrome, renal insufficiency-related short stature, HIV-associated wasting |
| Mechanism | Binds GH receptors; stimulates IGF-1 production |
| Adverse Effects | Edema, arthralgias, myalgias, hyperglycemia, carpal tunnel syndrome |
| Contraindications | Active malignancy, closed epiphyses (for growth indications), acute critical illness |
2. Octreotide (Sandostatin) - Somatostatin Analog
| Feature | Detail |
|---|---|
| Type | Synthetic somatostatin analog |
| Indications | Acromegaly, carcinoid tumors (flushing/diarrhea), VIPomas, esophageal variceal bleeding, diarrhea |
| Mechanism | Mimics somatostatin - inhibits GH, glucagon, insulin, and TSH secretion; reduces splanchnic blood flow |
| Adverse Effects | GI upset (nausea, diarrhea, abdominal pain), cholelithiasis (reduced bile motility), hyperglycemia or hypoglycemia |
- Lanreotide (Somatuline Depot) is a longer-acting somatostatin analog used similarly for acromegaly.
B. Gonadotropin-Releasing Hormone (GnRH) Agonists and Antagonists
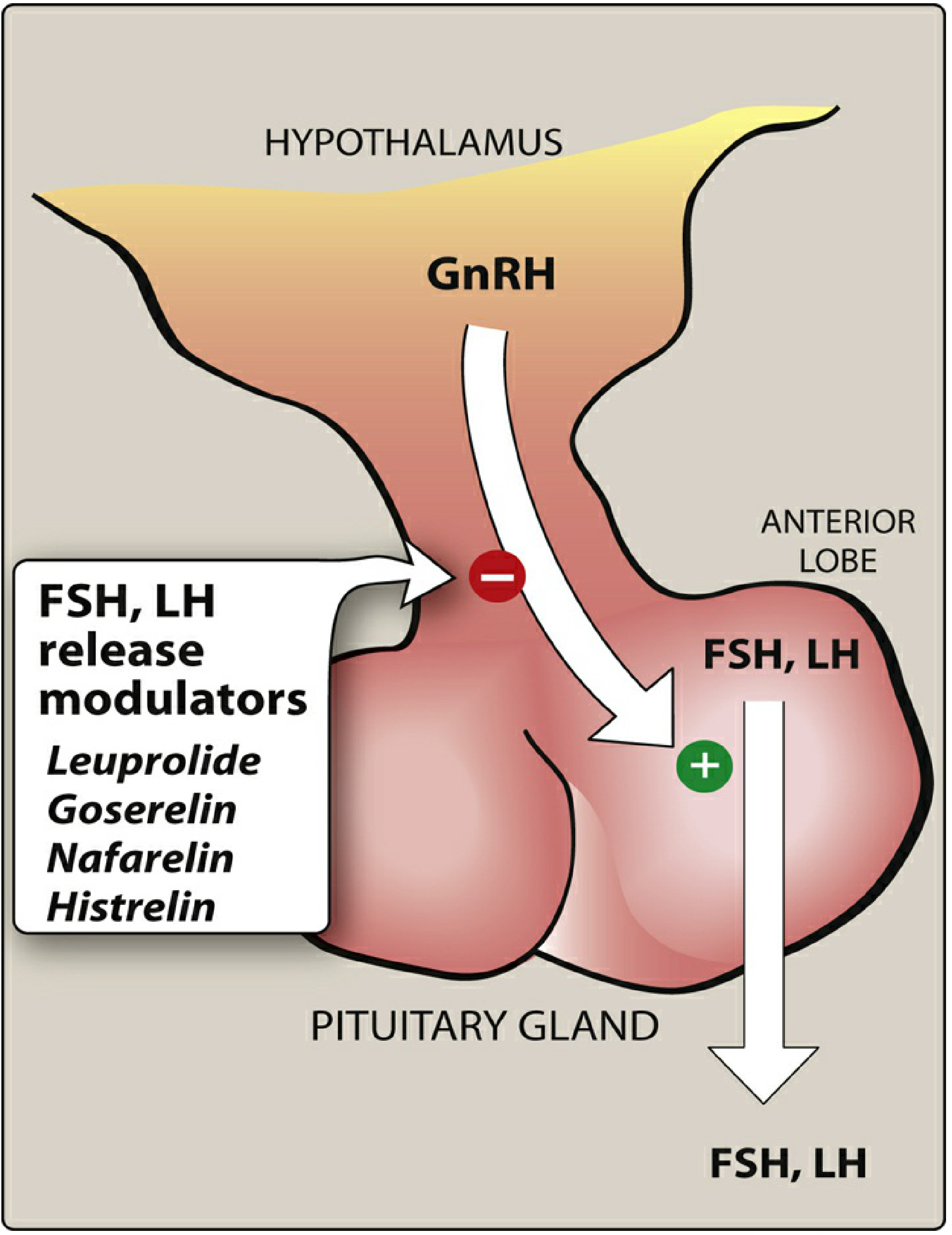
Key concept: GnRH is normally released in pulsatile fashion. Continuous (non-pulsatile) administration of GnRH agonists paradoxically suppresses gonadotropins (LH and FSH) due to receptor downregulation.
GnRH Agonists (Continuous use = suppression)
| Drug | Brand | Key Uses |
|---|---|---|
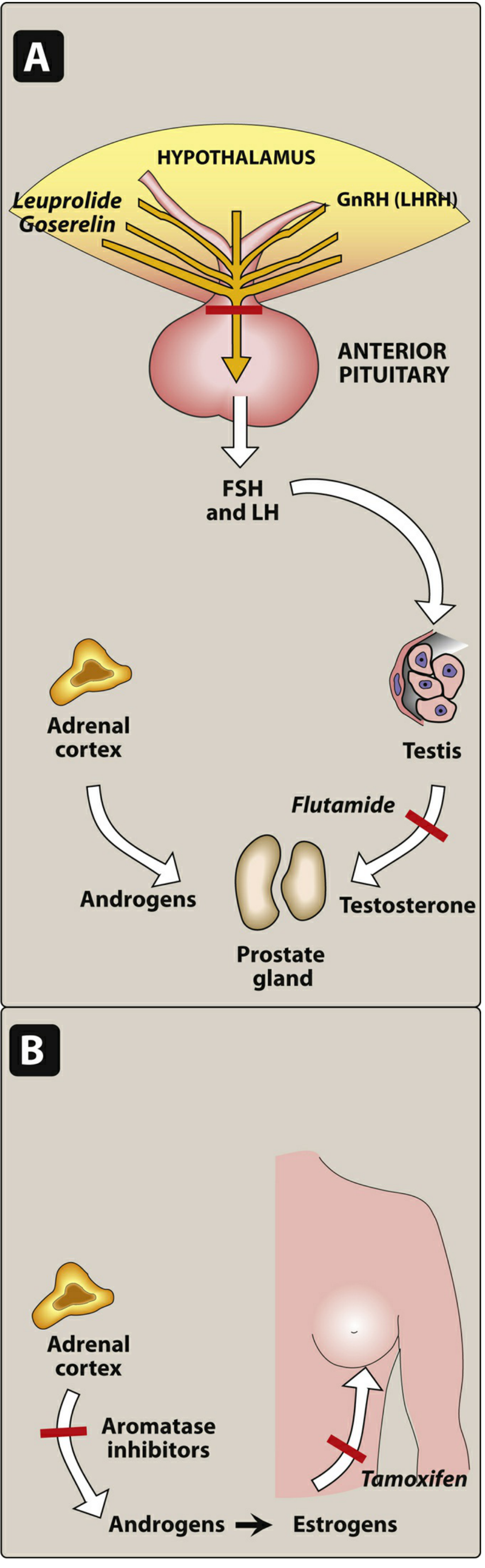
| Leuprolide | Lupron | Prostate cancer, endometriosis, uterine fibroids, central precocious puberty |
| Goserelin | Zoladex | Prostate/breast cancer, endometriosis |
| Nafarelin | Synarel | Endometriosis, central precocious puberty |
| Histrelin | Supprelin LA, Vantas | Central precocious puberty, prostate cancer |
Mechanism: Continuous stimulation → receptor downregulation → decreased LH/FSH → decreased sex steroids ("medical castration")
Adverse Effects:
- Initial flare effect (transient increase in testosterone/estrogen at start of therapy) - managed with anti-androgens in prostate cancer
- Hot flashes, decreased libido, impotence, osteoporosis (with prolonged use)
- In women: amenorrhea, vaginal dryness
Uses in Detail:
- Prostate cancer: Suppresses testosterone to castrate levels
- Endometriosis/fibroids: Reduces estrogen-driven growth
- Central precocious puberty: Suppresses premature pubertal development
- ART (IVF protocols): Used to prevent premature LH surge
C. Gonadotropins (FSH/LH Preparations)
Used in assisted reproduction and infertility:
| Drug | Type | Use |
|---|---|---|
| Follitropin alfa (Gonal-F) | Recombinant FSH | Ovulation induction, ART |
| Follitropin beta (Follistim AQ) | Recombinant FSH | Ovulation induction, ART |
| Urofollitropin (Bravelle) | Purified urinary FSH | Ovulation induction |
| Menotropins (Menopur) | FSH + LH (urinary) | Ovulation induction |
Main Adverse Effect: Ovarian Hyperstimulation Syndrome (OHSS) - abdominal pain, bloating, ascites, rarely severe (thromboembolism, renal failure)
D. Corticotropin (ACTH) and Cosyntropin
| Drug | Brand | Use |
|---|---|---|
| Corticotropin | HP Acthar | Infantile spasms (West syndrome), MS exacerbations |
| Cosyntropin | Cortrosyn | Diagnostic test for adrenal insufficiency (stimulation test) |
Mechanism: ACTH stimulates adrenal cortex to synthesize and release cortisol. Cosyntropin is a synthetic 24-amino acid analog of ACTH used diagnostically - a robust cortisol response rules out primary adrenal insufficiency.
III. POSTERIOR PITUITARY HORMONES
A. Vasopressin (ADH) and Desmopressin
Vasopressin (Vasostrict)
| Feature | Detail |
|---|---|
| Receptors | V1 (vasoconstriction), V2 (water reabsorption in collecting duct) |
| Indications | Septic shock (vasopressor), cardiac arrest (ACLS - no longer routinely recommended), variceal bleeding |
| Adverse Effects | Hypertension, cardiac ischemia, skin necrosis with extravasation, hyponatremia |
Desmopressin (DDAVP)
| Feature | Detail |
|---|---|
| Mechanism | V2 receptor agonist - increases water reabsorption in collecting duct |
| Indications | Central DI (diabetes insipidus), nocturnal enuresis, hemophilia A and von Willebrand disease type 1 (releases stored vWF and factor VIII) |
| Routes | Intranasal, oral, IV/SC |
| Adverse Effects | Hyponatremia, water intoxication, headache |
| Contraindication | Nephrogenic DI (kidneys don't respond to ADH) |
B. Oxytocin (Pitocin)
| Feature | Detail |
|---|---|
| Indications | Induction/augmentation of labor, control of postpartum hemorrhage |
| Mechanism | Stimulates uterine contractions (especially at term); also stimulates milk ejection (let-down reflex) |
| Adverse Effects | Uterine hyperstimulation (fetal distress), hyponatremia (antidiuretic effect at high doses), hypotension |
| Monitoring | Fetal heart rate monitoring during labor induction |
Drug Summary Table
| Drug Class | Drug | Key Use | Key Adverse Effect |
|---|---|---|---|
| GH analog | Somatropin | GH deficiency | Edema, hyperglycemia |
| Somatostatin analog | Octreotide, Lanreotide | Acromegaly, carcinoid | Gallstones, GI upset |
| GnRH agonist | Leuprolide, Goserelin | Prostate Ca, endometriosis | Initial flare, hot flashes |
| FSH | Follitropin alfa/beta | Infertility, ART | OHSS |
| ACTH | Cosyntropin | Adrenal stimulation test | - |
| ADH agonist | Desmopressin | Central DI, hemophilia A | Hyponatremia |
| ADH agonist | Vasopressin | Septic shock | Hypertension, ischemia |
| Uterotonic | Oxytocin | Labor induction | Uterine hyperstimulation |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 23 - Pituitary and Thyroid (Shannon A. Miller, Christina E. DeRemer), pp. 764-785
Gnrh drugs
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is the complete GnRH drug coverage from Lippincott Illustrated Reviews: Pharmacology, Chapter 23:
GnRH Drugs - Lippincott Pharmacology
The Core Concept: Pulsatile vs. Continuous
This is the single most important pharmacological concept for GnRH drugs:
| Mode | Effect |
|---|---|
| Pulsatile GnRH (physiologic) | Stimulates FSH and LH release from anterior pituitary |
| Continuous GnRH (pharmacologic) | Downregulates GnRH receptors on pituitary → inhibits FSH and LH |
Suppressed FSH/LH → reduced gonadal steroids (testosterone in men, estrogen in women). This is the basis for all GnRH agonist therapy.
A. GnRH Agonists (Continuous Use = Suppression)
Drugs
| Drug | Brand | Route/Formulation |
|---|---|---|
| Leuprolide | Lupron | SC daily injection, SC depot, IM depot |
| Goserelin | Zoladex | SC implant |
| Nafarelin | Synarel | Intranasal spray |
| Histrelin | Supprelin LA, Vantas | SC implant |
| Triptorelin | Trelstar | IM injection |
Mechanism
Synthetic GnRH analogs occupy the GnRH receptor on the pituitary → receptor desensitization → inhibition of FSH and LH release → reduced androgen and estrogen synthesis (equivalent to "medical castration").
Clinical Uses
| Indication | Rationale |
|---|---|
| Prostate cancer | Suppresses testosterone to castrate levels; response equivalent to orchiectomy with tumor regression and relief of bone pain |
| Endometriosis | Reduces estrogen-driven growth of ectopic endometrial tissue |
| Uterine fibroids | Estrogen-dependent tumors shrink with reduced estrogen |
| Central precocious puberty | Suppresses premature LH/FSH surge causing early puberty |
| Infertility / ART (IVF) | Prevents premature LH surge during controlled ovarian stimulation |
| Premenopausal breast cancer | Reduces estrogen in ER-positive tumors |
Adverse Effects
The "Flare" Reaction (Critical)
At the start of therapy, before downregulation occurs, GnRH receptors are briefly activated → transient rise in testosterone (men) or estrogen (women). This can cause:
- Worsening bone pain in prostate cancer
- Tumor flare in the first 1-2 weeks
- Management: Co-administer an antiandrogen (e.g., flutamide, bicalutamide) for the first few weeks in prostate cancer to block the testosterone surge
Chronic Effects (from sex steroid suppression):
In Women:
- Hot flashes and sweating
- Diminished libido
- Depression
- Ovarian cysts
- Decreased bone mineral density (osteoporosis with prolonged use)
- Amenorrhea, vaginal dryness
In Men:
- Hot flashes, edema
- Gynecomastia
- Diminished libido
- Sexual dysfunction
- Decreased bone mineral density
Contraindications: Pregnancy and breastfeeding
B. GnRH Antagonists
| Drug | Brand | Use |
|---|---|---|
| Cetrorelix | Cetrotide | Infertility (ART/IVF protocols) |
| Ganirelix | Orgalutran | Infertility (ART/IVF protocols) |
Mechanism
Directly block GnRH receptors on the pituitary → immediate inhibition of LH secretion. No initial flare effect (unlike agonists).
Use in Infertility
Used in controlled ovarian stimulation protocols to prevent a premature LH surge from causing early ovulation before egg retrieval. This is their primary clinical role.
Advantage over agonists in ART: No flare effect, faster onset of suppression, and shorter duration of use needed.
C. Comparison: GnRH Agonists vs. Antagonists
| Feature | GnRH Agonists | GnRH Antagonists |
|---|---|---|
| Mechanism | Receptor downregulation (continuous) | Direct competitive block |
| Onset of suppression | Delayed (days-weeks) | Immediate |
| Initial flare | Yes (testosterone/estrogen spike) | No |
| Main clinical uses | Prostate Ca, endometriosis, precocious puberty, ART | ART (prevent LH surge), prostate Ca |
| Examples | Leuprolide, Goserelin, Nafarelin | Cetrorelix, Ganirelix |
D. Gonadotropins (Related - FSH/LH Preparations)
These are used alongside GnRH drugs in infertility protocols:
| Drug | Content | Source |
|---|---|---|
| Menotropins (Menopur) | FSH + LH | Urine of postmenopausal women |
| Urofollitropin (Bravelle) | FSH only | Urine of postmenopausal women |
| Follitropin alfa (Gonal-F) | Recombinant FSH | Recombinant DNA |
| Follitropin beta (Follistim AQ) | Recombinant FSH | Recombinant DNA |
| hCG / Choriogonadotropin alfa | LH-like activity | Urine of pregnant women / recombinant |
Use in infertility: FSH products given over 5-12 days → ovarian follicular growth and maturation → then hCG triggers ovulation.
Key adverse effect: Ovarian hyperstimulation syndrome (OHSS) - ovarian enlargement, ascites, potential thromboembolism (can be life-threatening). Multiple births can also occur.
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 23 (pp. 772-773) and Chapter 37 (pp. 1259-1260)
Vasopressin
Finding Sources
Reading File
Loading Image
Vasopressin (Antidiuretic Hormone, ADH)
Source: Lippincott Illustrated Reviews - Pharmacology, Chapter 23
Origin and Synthesis
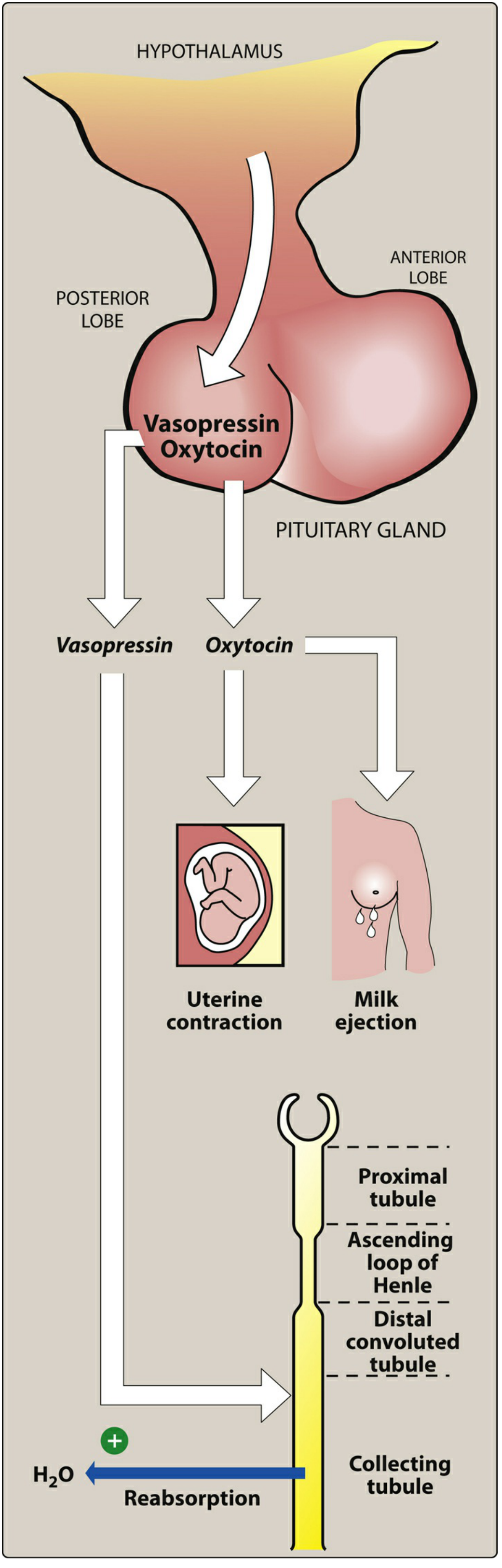
Vasopressin is synthesized in the hypothalamus, transported via axons, and stored/released from the posterior pituitary. It is NOT regulated by releasing hormones (unlike anterior pituitary hormones). Release is triggered by:
- High plasma osmolarity
- Low blood volume/pressure
- Pain, nausea, stress
Structure
Vasopressin is a neuropeptide structurally related to oxytocin - the two differ by only two amino acids.
Receptors and Actions
| Receptor | Location | Effect |
|---|---|---|
| V2 | Renal collecting tubules | Increases water permeability (aquaporin-2 insertion) → water reabsorption → concentrated urine |
| V1 | Vascular smooth muscle, liver, other tissues | Vasoconstriction (pressor effect) |
Clinical Uses
| Indication | Mechanism |
|---|---|
| Diabetes Insipidus (central) | V2 agonism → increased water reabsorption → decreased urine output |
| Septic shock | V1-mediated vasoconstriction → raises blood pressure |
| Esophageal variceal bleeding | Splanchnic vasoconstriction → reduces portal venous pressure |
Adverse Effects
| Effect | Mechanism |
|---|---|
| Water intoxication | Excess V2 stimulation → too much water retention |
| Hyponatremia | Dilutional - water retained without sodium |
| Abdominal pain, tremor, vertigo | Direct drug effects |
| Cardiac ischemia, hypertension | V1-mediated vasoconstriction |
Desmopressin (DDAVP) - The Preferred Analog
Desmopressin is a synthetic analog of vasopressin with key differences:
| Feature | Vasopressin | Desmopressin |
|---|---|---|
| V1 activity | Yes (pressor effects) | Minimal - largely free of pressor effects |
| V2 selectivity | V1 + V2 | Selective V2 agonist |
| Half-life | Short | Longer acting |
| Route | IV | Intranasal, oral, IV/SC |
Why Desmopressin is Preferred
Because it has minimal V1 activity, desmopressin avoids vasoconstriction and pressor adverse effects, making it safer for chronic use.
Clinical Uses of Desmopressin
| Indication | Notes |
|---|---|
| Central Diabetes Insipidus | Drug of choice; reduces excessive urine production |
| Nocturnal enuresis (bedwetting) | Oral route preferred; intranasal spray NOT recommended in children due to risk of seizures |
| Hemophilia A | Stimulates release of stored von Willebrand factor and Factor VIII from endothelium |
| von Willebrand disease type 1 | Same mechanism as above |
Adverse Effects of Desmopressin
- Hyponatremia / water intoxication (most important)
- Headache
- Local nasal irritation (with intranasal formulation)
- Seizures in children with nasal spray formulation (contraindicated for enuresis in children)
Quick Comparison Summary
| Feature | Vasopressin | Desmopressin |
|---|---|---|
| Receptors | V1 + V2 | V2 selective |
| Pressor effect | Yes | Minimal |
| Main uses | Septic shock, DI, varices | Central DI, enuresis, hemophilia A, vWD type 1 |
| Route | IV | Intranasal / Oral / IV |
| Key toxicity | Hyponatremia, water intoxication, hypertension | Hyponatremia, seizures (intranasal in children) |
Note: Desmopressin does not work in nephrogenic DI - because the kidneys are unresponsive to ADH regardless of dose.
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 23 - Pituitary and Thyroid, p. 776-777
Drug in hypothyroidism
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Drugs in Hypothyroidism
Source: Lippincott Illustrated Reviews - Pharmacology, Chapter 23
Understanding the Axis First
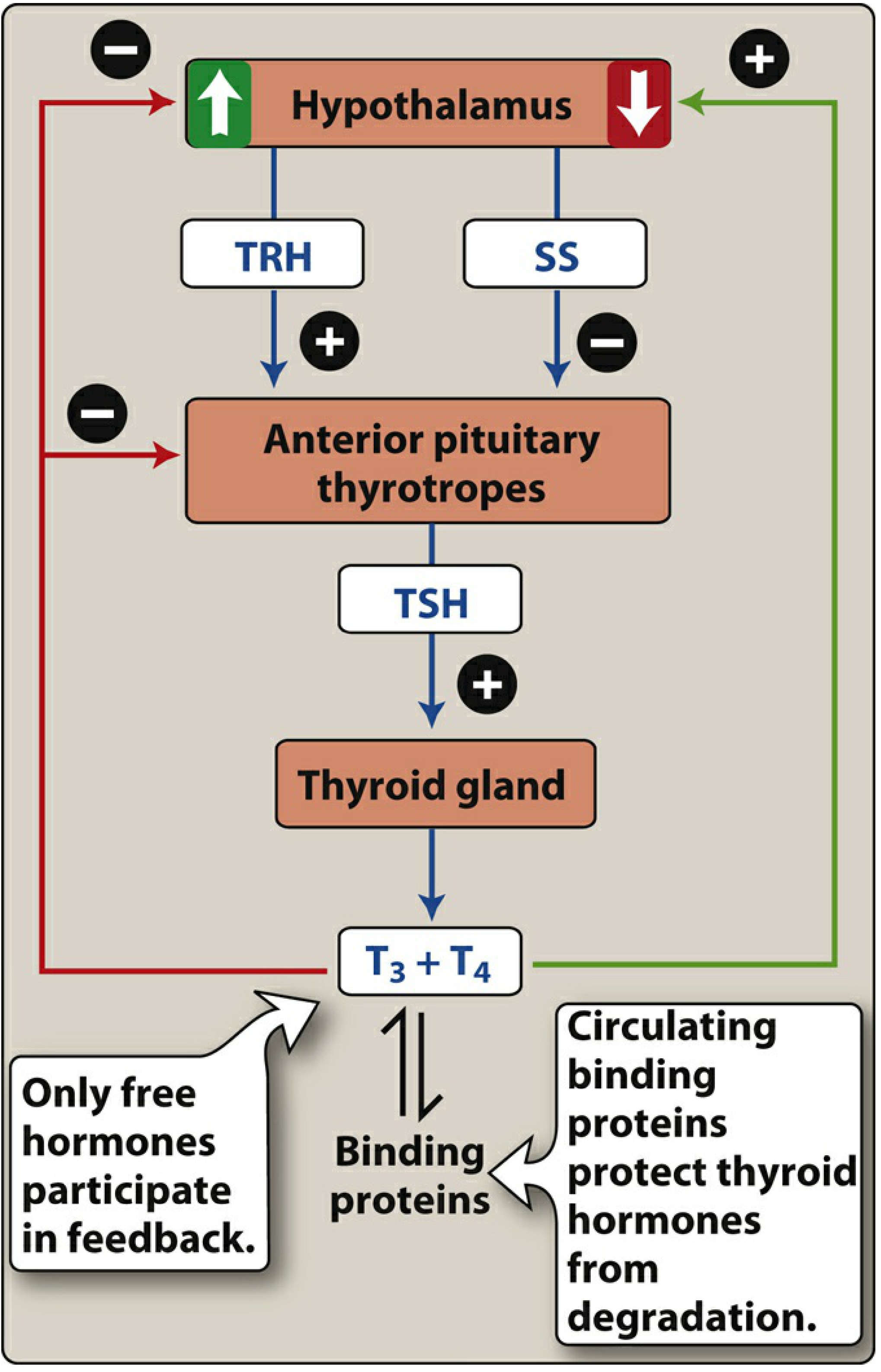
In hypothyroidism, TSH is elevated (anterior pituitary trying harder to stimulate an underperforming thyroid). This is the key diagnostic lab finding.
Common cause: Autoimmune destruction of the gland (Hashimoto thyroiditis - antibodies to thyroid peroxidase are diagnostic).
Symptoms of hypothyroidism:
- Bradycardia
- Cold intolerance
- Weight gain
- Fatigue
- Mental impairment
- In children: intellectual impairment and dwarfism
Thyroid Hormone Preparations
Three preparations are available, but Levothyroxine (T4) is the drug of choice:
| Drug | Brand | Content | Status |
|---|---|---|---|
| Levothyroxine | Synthroid, Levoxyl | Synthetic T4 | First-line, preferred |
| Liothyronine | Cytomel | Synthetic T3 | Less preferred |
| Liotrix | Thyrolar | T3 + T4 combination | Less preferred |
Levothyroxine (T4) - Drug of Choice
Why Levothyroxine is Preferred Over T3 Preparations
| Feature | Levothyroxine (T4) | Liothyronine (T3) |
|---|---|---|
| Tolerability | Better tolerated | Worse (more cardiac side effects) |
| Half-life | Long (7-10 days) | Short |
| Dosing | Once daily | Multiple times daily |
| Conversion | Converted to T3 in peripheral tissues | Active directly |
| Preference | Yes - first choice | Reserved for special situations |
Mechanism of Action
- T4 (levothyroxine) is absorbed and converted peripherally to the active T3 by deiodination
- T3 enters the nucleus, binds specific receptors, and stimulates:
- Oxygen consumption
- Mitochondrial gene expression
- Mitochondriogenesis (increased metabolic rate)
- Most circulating T3/T4 is bound to thyroxine-binding globulin - only free hormone is active and participates in feedback
Pharmacokinetics
- Dosed once daily
- Steady state achieved in 6-8 weeks
- Symptoms generally improve within a few weeks; complete recovery may take months
Goals of Therapy
- Normalize TSH (primary monitoring parameter)
- Improvement in symptoms of hypothyroidism
- TSH should be rechecked 6-8 weeks after initiation or any dose change
Toxicity (Overdose)
Too much levothyroxine mirrors hyperthyroidism symptoms:
- Nervousness and anxiety
- Palpitations and tachycardia
- Heat intolerance
- Unexplained weight loss
Toxicity is directly related to elevated T3/T4 levels.
Important Drug Interactions with Levothyroxine
CYP450 Inducers - Accelerate T4 Metabolism
Drugs that induce cytochrome P-450 enzymes accelerate metabolism of thyroid hormones and may decrease effectiveness of levothyroxine:
| Drug | Class |
|---|---|
| Phenytoin | Antiepileptic |
| Rifampin | Antibiotic (TB) |
| Phenobarbital | Antiepileptic/sedative |
Clinical implication: Patients on these drugs may need higher doses of levothyroxine.
Monitoring Summary
| Parameter | Timing | Goal |
|---|---|---|
| TSH | 6-8 weeks after start/dose change | Normal range |
| Symptoms | Weeks to months | Resolution of hypothyroid symptoms |
| Signs of toxicity | Ongoing | Absence of tachycardia, weight loss, nervousness |
Clinical Application (Lippincott Box 23.2)
Thyroid function is evaluated by TSH. Elevated TSH = hypothyroidism. Synthetic T4 (levothyroxine) is preferred. Due to the long half-life of T4 (7-10 days), improvement in symptoms often takes weeks, and TSH should be measured 6-8 weeks after initiation or a dosage change.
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 23 - Pituitary and Thyroid, pp. 778-782
Hyperthyroidism drugs
Reading File
Loading Image
Loading Image
Drugs in Hyperthyroidism (Thyrotoxicosis)
Source: Lippincott Illustrated Reviews - Pharmacology, Chapter 23
Overview
The most common cause of hyperthyroidism is Graves disease - an autoimmune condition where stimulating antibodies act like TSH. TSH levels are low (suppressed by negative feedback from excess T3/T4).
Symptoms: Tachycardia, cardiac arrhythmias, body wasting, nervousness, tremor, heat intolerance, palpitations, weight loss, mood disturbance.
Goal of therapy: Decrease synthesis and/or release of thyroid hormone.
Three Approaches to Treatment
1. Inhibition of Thyroid Function (Definitive)
a. Surgery (Thyroidectomy)
- Partial or total removal of the thyroid gland
- Used for severe hyperthyroidism requiring more immediate effects
- Iodide given pre-operatively to reduce vascularity of the gland
b. Radioactive Iodine (¹³¹I)
- Selectively taken up by thyroid follicular cells → destroys overactive tissue
- Effect takes several months
- Most patients develop hypothyroidism afterward and require lifelong levothyroxine
- Not useful short-term; definitive long-term solution
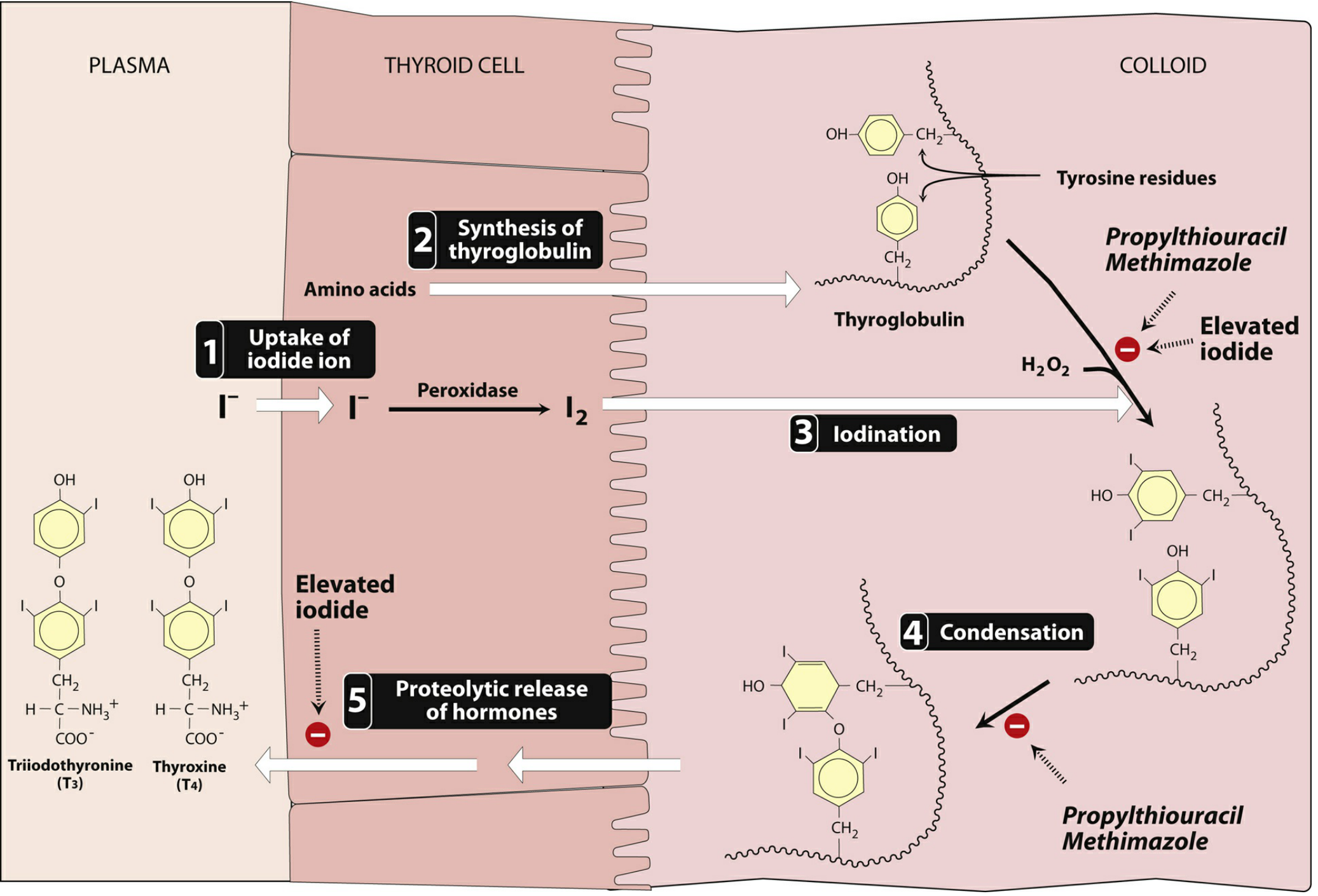
2. Inhibition of Thyroid Hormone Synthesis - The Thioamides
The two thioamide drugs are Propylthiouracil (PTU) and Methimazole:
Mechanism of Action (Both)
- Inhibit thyroid peroxidase → block oxidation of iodide to iodine
- Block iodination of tyrosyl groups on thyroglobulin (Step 3)
- Block condensation/coupling of iodotyrosines to form T3 and T4 (Step 4)
- PTU additionally blocks the peripheral conversion of T4 to T3 (in liver and other tissues)
Important: These drugs have no effect on thyroglobulin already stored in the gland. Clinical effects are therefore delayed until stored thyroglobulin is depleted.
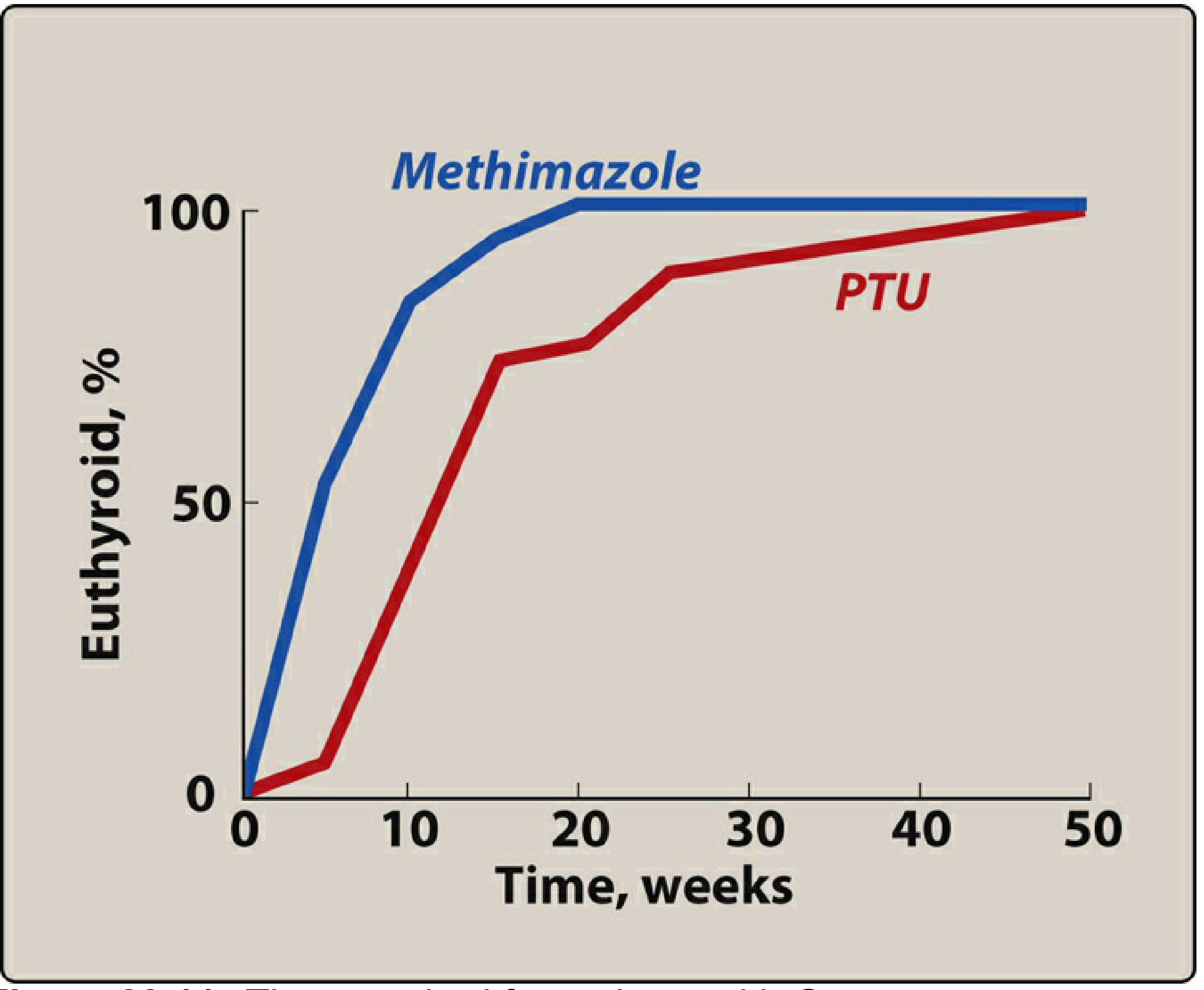
Methimazole vs. PTU - Key Comparison
| Feature | Methimazole | PTU |
|---|---|---|
| Blocks T4→T3 conversion | No | Yes (extra benefit in thyroid storm) |
| Half-life | Longer | Shorter |
| Dosing | Once daily | Multiple times daily |
| Preferred in general | Yes - first choice | Second choice |
| Pregnancy (1st trimester) | Teratogenic - avoid | Preferred (less teratogenic in 1st trimester) |
| Pregnancy (2nd/3rd trimester) | Switch back to methimazole | Avoid (risk of hepatotoxicity) |
| Hepatotoxicity | Less severe | More severe - risk of fatal acute liver failure |
| Time to euthyroid | Faster (~10 weeks) | Slower (~20 weeks) |
Adverse Effects of Both Thioamides
| Effect | Notes |
|---|---|
| Rash, pruritus, arthralgia | Common mild effects |
| Agranulocytosis | Both agents - most dangerous hematologic effect; patient should report sore throat/fever immediately |
| Hepatotoxicity | Both; PTU associated with potentially fatal acute liver failure |
3. Blockade of Hormone Release - Iodide
Preparations: Lugol's solution (iodine + potassium iodide), potassium iodide (SSKI)
Mechanism
- Wolff-Chaikoff effect: High pharmacologic dose of iodide inhibits iodination of tyrosines - but this effect lasts only a few days (escape occurs)
- More importantly: iodide inhibits proteolytic release of thyroid hormones from thyroglobulin (mechanism not fully understood)
- Decreases vascularity of the thyroid gland
Clinical Uses
| Use | Rationale |
|---|---|
| Pre-operative preparation | Reduces vascularity, making surgery safer |
| Thyroid storm | Rapidly blocks hormone release |
| NOT for long-term therapy | Escape from Wolff-Chaikoff effect limits prolonged use |
Adverse Effects of Iodide
- Sore mouth and throat
- Swelling of tongue or larynx
- Rashes
- Ulcerations of mucous membranes
- Metallic taste
4. Adjunct Therapy - Beta-Blockers
Beta-blockers (especially propranolol) are used as adjuncts to:
- Control sympathetic symptoms - tachycardia, palpitations, tremor, anxiety
- Propranolol also inhibits peripheral T4→T3 conversion at high doses
- Used in thyroid storm and pre-operatively while awaiting thioamide effect
5. Thyroid Storm
Thyroid storm = extreme/life-threatening hyperthyroidism.
Treatment is the same drugs as for hyperthyroidism, but given at higher doses and more frequently:
- PTU preferred (blocks T4→T3 conversion - extra advantage)
- High-dose iodide (given 1-2 hours after PTU to prevent iodide from being used for new hormone synthesis)
- Beta-blockers (propranolol) for cardiovascular control
- Glucocorticoids (also inhibit T4→T3 conversion)
- Supportive care
Complete Drug Summary
| Drug | Mechanism | Key Use | Key Adverse Effect |
|---|---|---|---|
| Methimazole | Blocks peroxidase, iodination, coupling | Hyperthyroidism (first choice) | Agranulocytosis, hepatotoxicity |
| PTU | Same + blocks T4→T3 conversion | 1st trimester pregnancy, thyroid storm | Fatal hepatotoxicity (more severe) |
| Radioactive ¹³¹I | Destroys follicular cells | Definitive treatment | Hypothyroidism (requires lifelong T4) |
| Iodide (Lugol's) | Blocks hormone release, reduces vascularity | Pre-op prep, thyroid storm | Metallic taste, mucosal ulceration |
| Propranolol | Beta-block + inhibits T4→T3 | Symptom control, thyroid storm | Bradycardia, bronchospasm |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 23 - Pituitary and Thyroid, pp. 783-785
Glucocorticoid drug along with it’s classification
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Glucocorticoids - Classification and Drug Details
Source: Lippincott Illustrated Reviews - Pharmacology, Chapter 26
Adrenal Axis Overview
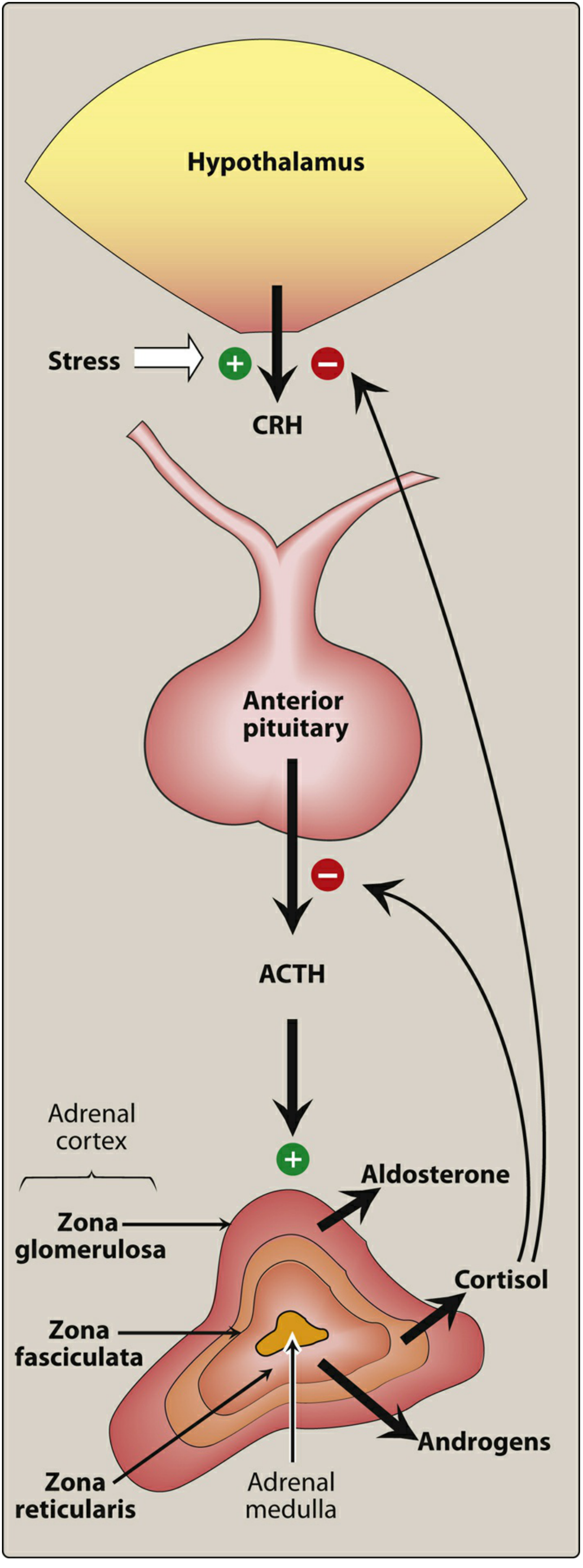
The adrenal cortex has three zones:
- Zona glomerulosa → Mineralocorticoids (aldosterone)
- Zona fasciculata → Glucocorticoids (cortisol) - controlled by ACTH
- Zona reticularis → Adrenal androgens - controlled by ACTH
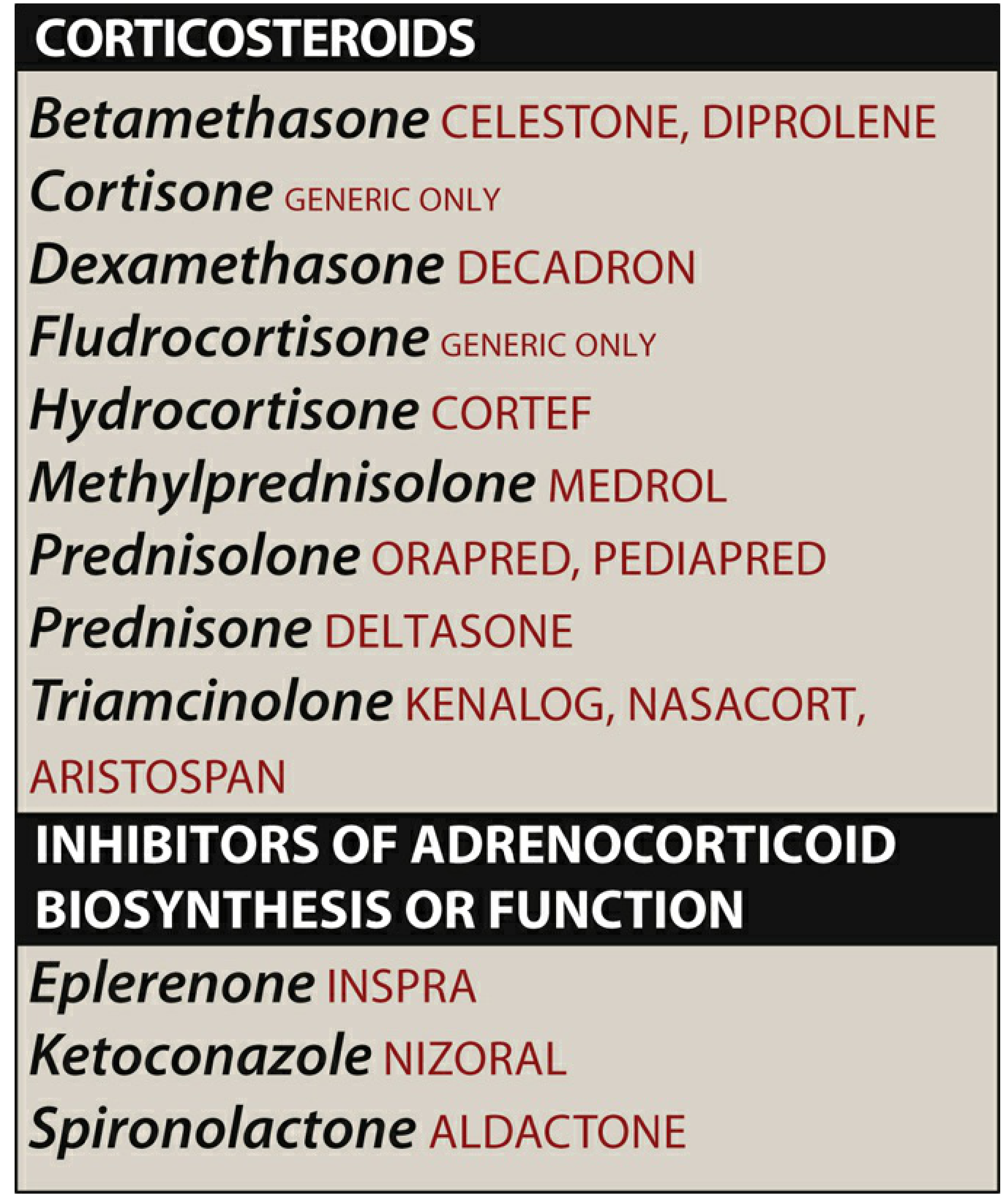
Drug List
Classification of Glucocorticoids
Glucocorticoids are classified by potency (anti-inflammatory) and duration of action:
Short-Acting (Biological half-life 8-12 hours)
| Drug | Brand | Glucocorticoid Potency | Mineralocorticoid Potency |
|---|---|---|---|
| Cortisol (Hydrocortisone) | Cortef | 1 (reference) | 1 |
| Cortisone | Generic | 0.8 | 0.8 |
Intermediate-Acting (Biological half-life 18-36 hours)
| Drug | Brand | Glucocorticoid Potency | Mineralocorticoid Potency |
|---|---|---|---|
| Prednisone | Deltasone | 4 | 0.25 |
| Prednisolone | Orapred, Pediapred | 4 | 0.25 |
| Methylprednisolone | Medrol | 5 | minimal |
| Triamcinolone | Kenalog, Nasacort | 5 | 0 |
Long-Acting (Biological half-life 36-72 hours)
| Drug | Brand | Glucocorticoid Potency | Mineralocorticoid Potency |
|---|---|---|---|
| Dexamethasone | Decadron | 25 | 0 |
| Betamethasone | Celestone, Diprolene | 25 | 0 |
Key point: As glucocorticoid potency increases, mineralocorticoid activity decreases. Dexamethasone and betamethasone are the most potent and have essentially zero mineralocorticoid activity.
Mechanism of Action
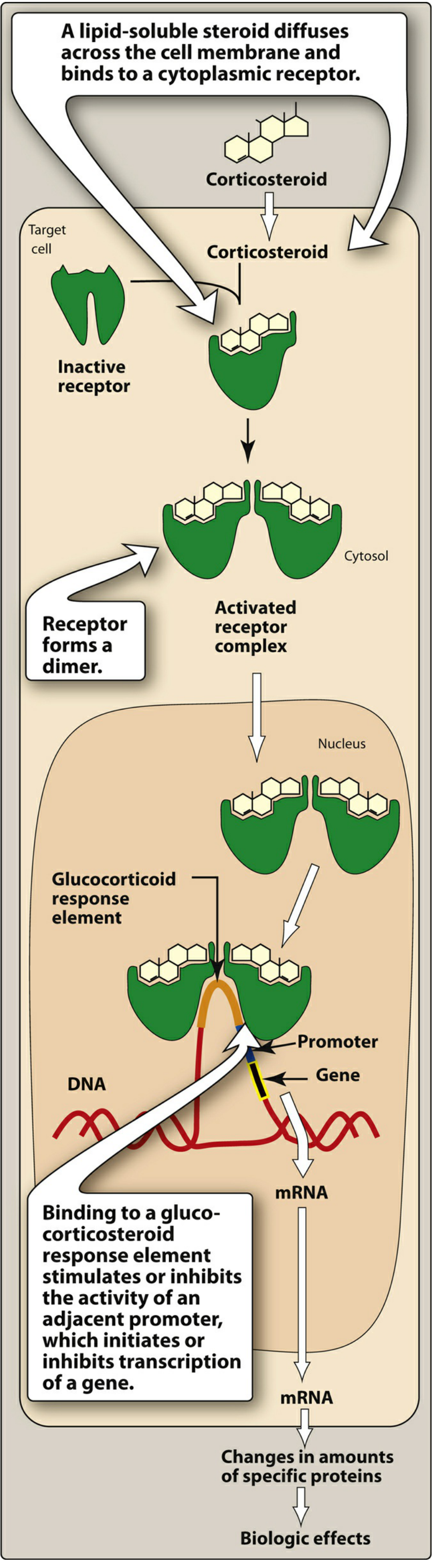
- Lipid-soluble steroid diffuses across cell membrane
- Binds intracellular cytoplasmic receptor
- Receptor-hormone complex dimerizes
- Recruits coactivator or corepressor proteins
- Translocates to nucleus → binds glucocorticoid response element (GRE)
- Acts as transcription factor → turns genes ON (coactivators) or OFF (corepressors)
- Effects take hours to days due to this genomic mechanism
Pharmacological Actions of Glucocorticoids
1. Metabolic Effects
- Stimulate hepatic gluconeogenesis (raise blood glucose)
- Mobilize amino acids from muscle (protein catabolism)
- Stimulate lipolysis → provide substrates for glucose synthesis
- Net result: hyperglycemia, muscle wasting, fat redistribution
2. Stress Response
- Raise plasma glucose to provide energy during trauma, fright, infection, bleeding
- GC insufficiency → hypoglycemia during stress (basis of adrenal crisis)
3. Blood Cell Effects
| Cell Type | Effect |
|---|---|
| Eosinophils, basophils, monocytes, lymphocytes | Decreased (redistributed to lymphoid tissue) |
| Neutrophils (PMNs), erythrocytes, hemoglobin, platelets | Increased |
4. Anti-inflammatory and Immunosuppressive Effects (Most Important Therapeutically)
- Decrease circulating lymphocytes
- Inhibit leukocyte and macrophage response to mitogens/antigens
- Decrease production of proinflammatory cytokines (IL-1, TNF, etc.)
- Induce synthesis of lipocortin → inhibits phospholipase A2 → blocks release of arachidonic acid → reduces prostaglandins AND leukotrienes
- Stabilize mast cell and basophil membranes → decreased histamine release
5. Other Effects
- High levels → negative feedback → suppress ACTH and CRH
- Suppress TSH synthesis
- Required for normal vascular responsiveness to catecholamines (pressor effect)
- CNS effects: mood changes, euphoria at low doses; psychosis at high doses
Therapeutic Uses
| Indication | Notes |
|---|---|
| Adrenal insufficiency (replacement) | Hydrocortisone or prednisone; primary (Addison) or secondary |
| Rheumatoid arthritis / inflammatory arthritis | Anti-inflammatory; lowest effective dose used |
| Asthma | Inhaled (beclomethasone, fluticasone) for maintenance; IV/oral for acute severe attacks |
| Allergic reactions / anaphylaxis | Adjunct to epinephrine |
| Inflammatory bowel disease | Prednisone, budesonide |
| Organ transplantation | Immunosuppression; often with other agents |
| Nephrotic syndrome | Reduce proteinuria |
| Cerebral edema | Dexamethasone (especially with brain tumors or meningitis) |
| Fetal lung maturity | Betamethasone - given to mother to accelerate surfactant production in premature fetus |
| Lymphomas / leukemias | Part of chemotherapy regimens (CHOP, etc.) |
| Septic shock / thyroid storm | High-dose glucocorticoids |
| Skin conditions | Topical corticosteroids for eczema, psoriasis |
Adverse Effects (The "CUSHINGOID" Mnemonic)
| System | Adverse Effect |
|---|---|
| Metabolic | Hyperglycemia (may precipitate diabetes), hyperlipidemia |
| Musculoskeletal | Osteoporosis, myopathy, muscle wasting, avascular necrosis of femoral head |
| Cardiovascular | Hypertension (Na/water retention), edema |
| Endocrine | Cushing syndrome (moon face, buffalo hump, central obesity), adrenal suppression |
| Immune | Increased susceptibility to infections (bacterial, fungal, viral) |
| GI | Peptic ulcers, GI bleeding (especially with NSAIDs) |
| Eye | Cataracts (posterior subcapsular), glaucoma |
| CNS | Mood changes, insomnia, euphoria, psychosis |
| Skin | Thin skin, striae, poor wound healing, bruising |
| Growth | Suppression of growth in children |
Discontinuation - Critical Warning
Abrupt withdrawal after prolonged use → Acute Adrenal Insufficiency (Adrenal Crisis):
- Manifestations: nausea, vomiting, fever, dehydration, hypotension, shock
- Also: hypoglycemia, hyperkalemia
- Cause: prolonged exogenous glucocorticoids suppress HPA axis → adrenal glands atrophy → cannot mount response when drug withdrawn
Rule: Always taper slowly - never stop abruptly after prolonged therapy.
Mineralocorticoid - Fludrocortisone
| Feature | Detail |
|---|---|
| Drug | Fludrocortisone (Generic) |
| Action | Pure mineralocorticoid - promotes Na reabsorption and K excretion in kidney |
| Use | Addison disease (with hydrocortisone), orthostatic hypotension |
Inhibitors of Adrenocorticoid Biosynthesis or Function
| Drug | Mechanism | Use |
|---|---|---|
| Ketoconazole | Inhibits ALL gonadal and adrenal steroid synthesis | Cushing syndrome (when surgery not an option) |
| Spironolactone | Mineralocorticoid receptor antagonist; also blocks aldosterone and testosterone synthesis | Hyperaldosteronism, resistant hypertension, heart failure, hirsutism |
| Eplerenone | Selective aldosterone receptor antagonist (less androgen affinity than spironolactone) | Hypertension, heart failure post-MI |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 26 - Adrenal Hormones, pp. 865-881
This is a shared conversation. Sign in to Orris to start your own chat.