Crisper in medicine
Reading File
Searching the Web
CRISPR medicine applications 2025 2026 clinical trials approvals
Searching PubMed
CRISPR gene editing clinical applications therapy
Finding Sources
Reading Article
PMID: 40268745
Reading Article
PMID: 40160040
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have rich textbook content and a clear mechanistic diagram. Here is a comprehensive overview of CRISPR in medicine:
CRISPR in Medicine
What is CRISPR?
CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats) was first described in 1987 in the genome of E. coli - five repeats of 29 nucleotides separated by spacer sequences of 32 nucleotides. These spacers were later found to form part of an adaptive, heritable immune system in bacteria and archaea, storing "memory" of past phage infections and using it to destroy re-invading DNA. - Tietz Textbook of Laboratory Medicine, 7th Ed.
The technology was adapted for human cells in 2012-2013 and has since become the dominant gene-editing platform.
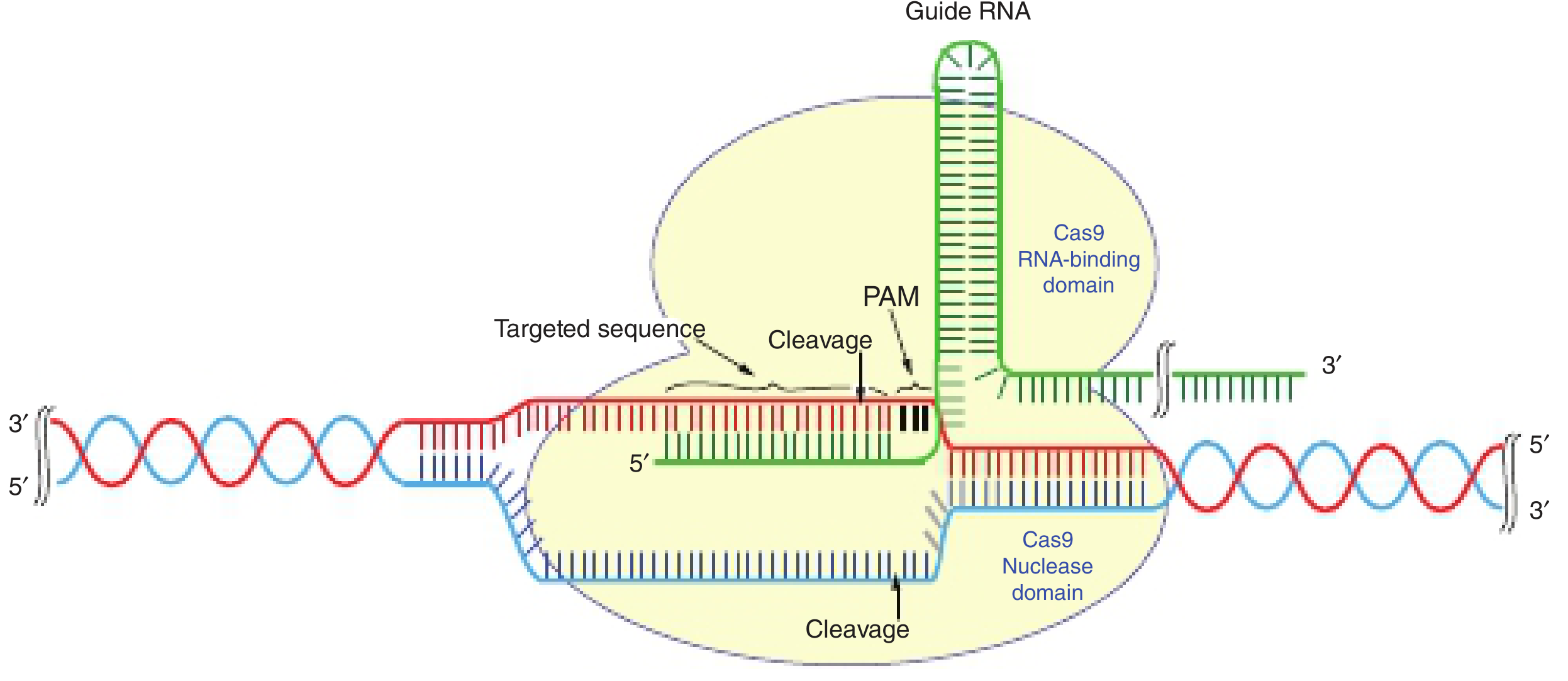
How the CRISPR-Cas9 System Works
The most widely used system pairs the Cas9 nuclease (from Streptococcus pyogenes) with a synthetic guide RNA (gRNA):
Three steps of the immune response (natural):
- Adaptation - invader DNA is integrated as a new spacer into the CRISPR array
- crRNA synthesis - the array is transcribed and processed by Cas proteins into mature CRISPR RNA
- Interference - crRNA directs Cas to cleave matching foreign sequences
In gene editing, once Cas9 makes a DSB, two repair pathways are exploited:
-
NHEJ (Non-Homologous End Joining) - error-prone; causes insertions/deletions (indels) → gene knockout
-
HDR (Homology-Directed Repair) - precise; uses a donor template → gene correction or insertion
-
Schwartz's Principles of Surgery, 11th Ed.
CRISPR Variants Beyond Cas9
| System | Target | Key Feature |
|---|---|---|
| Cas9 | dsDNA | Most widely used; introduces blunt-end DSBs |
| Cas12a | dsDNA | Staggered cuts; different PAM requirements |
| Cas13 | RNA | Targets mRNA; reversible; no permanent genome change |
| Base editors | dsDNA | Single nucleotide changes without DSBs; reduces off-target risk |
| Prime editors | dsDNA | "Search and replace" - precise insertions without DSBs or donor template |
| C2c2/Cas13 | RNA | RNA knockdown; useful for transient silencing |
- Zhang, Ma & Liu, Genomics Proteomics Bioinformatics, 2025 [PMID: 40268745]
Medical Applications
1. Hemoglobinopathies (FDA-Approved)
The landmark application: Casgevy (exa-cel, CTX001) received FDA approval in December 2023 - the first CRISPR-based drug. It:
- Edits autologous CD34+ hematopoietic stem cells ex vivo
- Reactivates fetal hemoglobin (HbF) by disrupting the BCL11A enhancer (which silences the γ-globin gene)
- Approved for sickle cell disease (SCD) and transfusion-dependent beta-thalassemia (TDT)
Clinical trials NCT03432364 and NCT03655678 demonstrated remarkable efficacy. - Rheumatology, 2-Vol Set, 2022; Cetin et al., Expert Rev Mol Med, 2025 [PMID: 40160040]
2. Cancer (CAR-T and Beyond)
- CRISPR is used to enhance CAR-T cell therapy - editing T cells to knock out immune checkpoint genes (e.g., PD-1) or HLA genes for allogeneic ("off-the-shelf") CAR-T products
- CRISPR screening (genome-wide loss-of-function screens) is identifying new cancer drug targets
3. Infectious Diseases
Diagnostics:
- SHERLOCK (CRISPR-Cas13): Specific High Sensitivity Enzymatic Reporter Unlocking - a SARS-CoV-2 SHERLOCK assay was the first CRISPR-based diagnostic to receive FDA Emergency Use Authorization
- DETECTR (CRISPR-Cas12): Used to detect HPV16/18 in clinical specimens
- CARVER (Cas13): Identifies viral infection AND directs RNA viral destruction
- FLASH (CRISPR-Cas9 + NGS): Detects antimicrobial resistance genes
Therapeutics:
-
HIV: gRNA-Cas9 constructs silence proviral HIV DNA in cell culture
-
Herpes viruses, HPV, HBV: targeted elimination in research models
-
"Resensitization to antibiotics": CRISPR targets ESBLs and restores β-lactam susceptibility in resistant bacteria
-
Tietz Textbook of Laboratory Medicine, 7th Ed.
4. Genetic / Rare Diseases (Pipeline)
- Duchenne Muscular Dystrophy - exon skipping to restore dystrophin reading frame
- Transthyretin amyloidosis - in vivo CRISPR (NTLA-2001) targets the TTR gene in the liver via lipid nanoparticles
- Retinal dystrophies - AAV-delivered CRISPR for CEP290 mutation (Leber congenital amaurosis)
- Chronic pain - CRISPR-based epigenome editing to silence pain genes without permanent DNA changes
5. Research Tools
- Large-scale genetic screening (CRISPR libraries)
- Lineage tracing in developmental biology
- Generating disease models (cell lines, animal models)
Challenges and Limitations
| Challenge | Details |
|---|---|
| Off-target effects | Cas9 may cleave at sites with partial complementarity to the gRNA |
| Delivery | Getting CRISPR components into target cells in vivo remains difficult; current vectors: AAV, lipid nanoparticles, electroporation |
| Immune response | Cas9 (bacterial protein) can trigger host immune reactions |
| Mosaicism | Incomplete editing across a tissue |
| Germline editing | Heritable edits raise profound ethical concerns; moratorium widely supported |
| Epigenetic effects | Long-term consequences of editing are not fully characterized |
| Scalability & cost | Manufacturing personalized ex vivo therapies (like Casgevy) is extremely expensive |
Recent Literature
- CRISPR Technology and Its Emerging Applications (Zhang et al., Genomics Proteomics Bioinformatics, 2025) - broad review of Cas9, Cas12a, Cas13, base editing, prime editing, and clinical applications [PMID: 40268745]
- Advancing CRISPR genome editing into gene therapy clinical trials (Cetin et al., Expert Rev Mol Med, 2025) - covers Casgevy approval, SCD/TDT outcomes, ongoing cancer and HIV trials, and challenges including off-target effects and delivery systems [PMID: 40160040]
Summary: CRISPR has moved from a bacterial immune curiosity to an FDA-approved therapeutic in under 15 years. The first approved drug (Casgevy) addresses sickle cell disease and beta-thalassemia. Active clinical trials are exploring applications in cancer, HIV, and multiple genetic disorders. Key bottlenecks now are safe in vivo delivery, minimizing off-target edits, long-term safety data, and cost - not the editing precision itself, which has improved dramatically with base and prime editors.
High yield Md exam oriented Dont miss important points Easy to remember and understand
Asking for Preferences
Here is a complete high-yield, exam-oriented CRISPR notes sheet - structured for maximum retention:
⚡ CRISPR - High Yield MD Exam Notes
🧠 FIRST, THE MNEMONIC
"CRISPR CUTS DNA SMARTLY"
| Letter | Stands for |
|---|---|
| C | Cas9 is the nuclease (scissors) |
| R | RNA guide directs it to target |
| I | Immune origin (bacterial adaptive immunity) |
| S | Spacers = memory of past infections |
| P | PAM sequence (NGG) required |
| R | Repair via NHEJ or HDR |
📌 ORIGIN - 1 LINE ANSWER
CRISPR = Part of bacterial adaptive immunity against bacteriophages First described in E. coli in 1987
🔧 MECHANISM (Most Asked)
Guide RNA (gRNA)
↓
Binds to TARGET DNA (Watson-Crick base pairing)
↓
Cas9 recognizes PAM sequence (5'-NGG-3')
↓
Cas9 cuts BOTH strands → Double Strand Break (DSB)
↓
Cell repairs the break via:
├── NHEJ → Indels → Gene KNOCKOUT ❌
└── HDR → Precise edit using template → Gene CORRECTION ✅
Exam trap: PAM = NGG (N = any nucleotide, GG = guanine-guanine). Required for Cas9 to work.
🔑 KEY COMPONENTS
| Component | Role | Remember as |
|---|---|---|
| gRNA | Directs Cas9 to target | GPS of the system |
| Cas9 | Nuclease - cuts DNA | Molecular scissors |
| PAM (NGG) | Recognition signal for Cas9 | Lock that must be present |
| NHEJ | Error-prone repair → knockout | "Messy fix" |
| HDR | Precise repair with template | "Clean fix" |
🧬 CAS PROTEIN VARIANTS (High Yield for Step 1 / NEET PG)
| Protein | Target | Key Point |
|---|---|---|
| Cas9 | dsDNA | Most common; blunt-end cut |
| Cas12a (Cpf1) | dsDNA | Staggered cuts; different PAM |
| Cas13 | RNA | Only RNA-targeting; reversible |
| Base editor | dsDNA | Single base change, NO DSB |
| Prime editor | dsDNA | "Find & replace" - no DSB, no template needed |
Exam tip: Cas13 targets RNA - useful for viral RNA destruction (CARVER system)
💊 FDA-APPROVED CRISPR DRUG (Highest Yield Clinical Fact)
Casgevy (exa-cel / CTX001) - Approved December 2023
| Feature | Detail |
|---|---|
| Disease | Sickle Cell Disease + β-Thalassemia |
| Mechanism | Edits CD34+ hematopoietic stem cells (ex vivo) |
| Target gene | BCL11A enhancer (suppressor of fetal Hb) |
| Effect | ↑ Fetal Hemoglobin (HbF) → compensates for abnormal HbS/absent HbA |
| Type | Ex vivo editing - cells taken out, edited, reinfused |
| Significance | FIRST CRISPR-based drug ever approved |
Memory trick: "CASgevy uses CAS9 to CASt away sickle cell disease"
🔬 CRISPR DIAGNOSTICS (Exam Favorite)
| Platform | Full Name | Target | Used For |
|---|---|---|---|
| SHERLOCK | Specific High-sensitivity Enzymatic Reporter unLOCKing | RNA (Cas13) | COVID-19 - 1st CRISPR Dx with FDA EUA |
| DETECTR | DNA Endonuclease Targeted CRISPR Trans Reporter | DNA (Cas12) | HPV 16/18 detection |
| CARVER | Cas13-Assisted Restriction of Viral Expression & Readout | RNA (Cas13) | Viral ID + destruction |
| FLASH | Finding Low Abundance Sequences by Hybridization | DNA (Cas9+NGS) | AMR gene detection |
Trick to remember: SHERLOCK = SARS-CoV-2. First EUA. Cas13 (RNA).
🦠 THERAPEUTIC APPLICATIONS BY DISEASE
| Disease | Approach | Status |
|---|---|---|
| Sickle cell / β-Thal | Reactivate HbF via BCL11A editing | FDA APPROVED |
| HIV | Excise proviral DNA using gRNA-Cas9 | Research/trials |
| HBV, HSV, HPV | Targeted elimination of viral genome | Research |
| MRSA / ESBL bacteria | "Resensitize" to antibiotics | Research |
| Duchenne MD | Exon skipping, restore dystrophin | Trials |
| Transthyretin amyloidosis | In vivo TTR gene knockdown via LNP | Trials |
| Leber Congenital Amaurosis | AAV-delivered CRISPR; CEP290 mutation | Trials |
| Cancer (CAR-T) | Knock out PD-1, HLA genes in T cells | Trials |
⚠️ CHALLENGES / LIMITATIONS (MCQ trap answers)
| Problem | One-liner |
|---|---|
| Off-target effects | Cas9 cuts wrong sites with partial gRNA match |
| Delivery | Hard to get CRISPR inside cells in vivo; use AAV or lipid nanoparticles (LNP) |
| Immune reaction | Cas9 is bacterial → host may mount immune response |
| Mosaicism | Not all cells in tissue get edited |
| Germline editing | Heritable; ethically banned (He Jiankui scandal - 2018, CCR5 editing) |
| Cost | Casgevy costs ~$2-3 million per patient |
⚡ REPAIR PATHWAY COMPARISON (High Yield)
| NHEJ | HDR | |
|---|---|---|
| Template needed? | ❌ No | ✅ Yes |
| Accuracy | Low (indels) | High |
| Result | Gene knockout | Gene correction |
| Cell cycle phase | Any | S/G2 only |
| Use in therapy | Disrupting bad gene | Fixing mutant gene |
🏆 ONE-LINERS FOR VIVA / SHORT ANSWER
- First CRISPR drug = Casgevy (sickle cell, Dec 2023)
- PAM sequence = NGG (required for Cas9)
- SHERLOCK = first CRISPR diagnostic with FDA EUA (for SARS-CoV-2)
- Cas13 = only targets RNA (all others target DNA)
- NHEJ = messy = knockout; HDR = precise = correction
- BCL11A = the target in Casgevy (suppressor of fetal Hb)
- Ex vivo = cells taken out for editing (like Casgevy); in vivo = editing inside the body
- He Jiankui scandal = first (illegal) human germline editing (CCR5 gene, HIV resistance, 2018)
- Base editing = single nucleotide change WITHOUT cutting both strands
- Prime editing = most precise; no DSB, no donor template needed ("the next generation")
🗂️ COMPARE WITH OTHER GENE EDITING TOOLS
| Tool | Mechanism | Precision | Notes |
|---|---|---|---|
| ZFN (Zinc Finger Nucleases) | Protein-DNA binding | Low | Old, difficult to design |
| TALEN | Protein-DNA binding | Moderate | Better than ZFN |
| CRISPR-Cas9 | RNA-DNA binding | High | Easy, cheap, programmable |
| Base editor | CRISPR + deaminase | Very high | No DSB |
| Prime editor | CRISPR + RT | Highest | No DSB, no template |
Why CRISPR won: RNA-guided (easy to reprogram) vs. protein-guided (ZFN/TALEN = must engineer new protein each time)
🎯 PREDICTED MCQ STEMS
- "A patient with sickle cell disease receives autologous stem cell therapy that reactivates fetal hemoglobin. What gene was targeted?" → BCL11A
- "Which CRISPR diagnostic received the first FDA EUA?" → SHERLOCK (COVID)
- "Which Cas protein targets RNA instead of DNA?" → Cas13
- "What repair pathway results in precise gene correction?" → HDR
- "The PAM sequence required by Cas9 is?" → 5'-NGG-3'
- "First FDA-approved CRISPR therapy?" → Casgevy (exa-cel)
- "CRISPR was adapted from which organism's immune system?" → Bacteria (originally E. coli)
📚 Sources: Tietz Textbook of Laboratory Medicine 7th Ed; Harper's Illustrated Biochemistry 32nd Ed; Schwartz's Principles of Surgery 11th Ed; Cetin et al., Expert Rev Mol Med 2025 [PMID 40160040]; Zhang et al., Genomics Proteomics Bioinformatics 2025 [PMID 40268745]
This is a shared conversation. Sign in to Orris to start your own chat.