Lymphatic drainage of lung and it's applied anatomy full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive, authoritative information from multiple textbooks. Let me now compile the complete MD exam answer.
Lymphatic Drainage of the Lung and Applied Anatomy
Introduction
The lung has a rich lymphatic system that serves three primary functions: fluid homeostasis, macromolecule clearance (including hyaluronan), and immune cell trafficking. Understanding the anatomy of pulmonary lymphatics is essential for clinical practice, particularly in thoracic surgery, oncology, and the management of pulmonary and pleural diseases.
Anatomy of the Pulmonary Lymphatic System
Two Plexuses (Dual Lymphatic Drainage)
The lungs drain through two distinct lymphatic plexuses that run parallel to the dual blood supply:
1. Superficial (Pleural) Plexus
- Located in the connective tissue of the visceral pleura (beneath the mesothelium)
- Drains the surface of the lung
- Vessels travel along the pleural surface toward the hilum
- Collecting lymphatics in the lung periphery drain toward the visceral pleura but do NOT connect to the pleural space
2. Deep (Peribronchial/Perivascular) Plexus
- Drains the lung parenchyma (interstitium, bronchovascular bundles, interlobular septa)
- Follows air passages (bronchi) and pulmonary blood vessels centrally toward the hilum
- Lymph nodes are found along the course of larger lymphatic vessels
- The vast majority of intralobular lymphatics are associated with blood vessels or located in bronchovascular bundles
- There are very few lymphatics alongside alveoli in the normal lung
Both plexuses converge at the hilum.
Microstructure of Lymphatic Vessels
- Initial lymphatic capillaries: small, thin-walled, blind-ended structures with discontinuous "button" junctions between adjacent endothelial cells - these flap-like openings allow fluid and cells to enter
- Collecting lymphatics: larger, contain valves and zipper-like continuous junctions; in the lung they have only sporadic smooth muscle cell coverage (unlike elsewhere in the body), so they cannot contract robustly - lung lymph flow is driven primarily by extrinsic forces (changes in thoracic pressure with ventilation)
Regional Lymph Nodes (TNM Classification)
The IASLC lymph node map, used in TNM staging for lung cancer, divides nodes into two main groups:
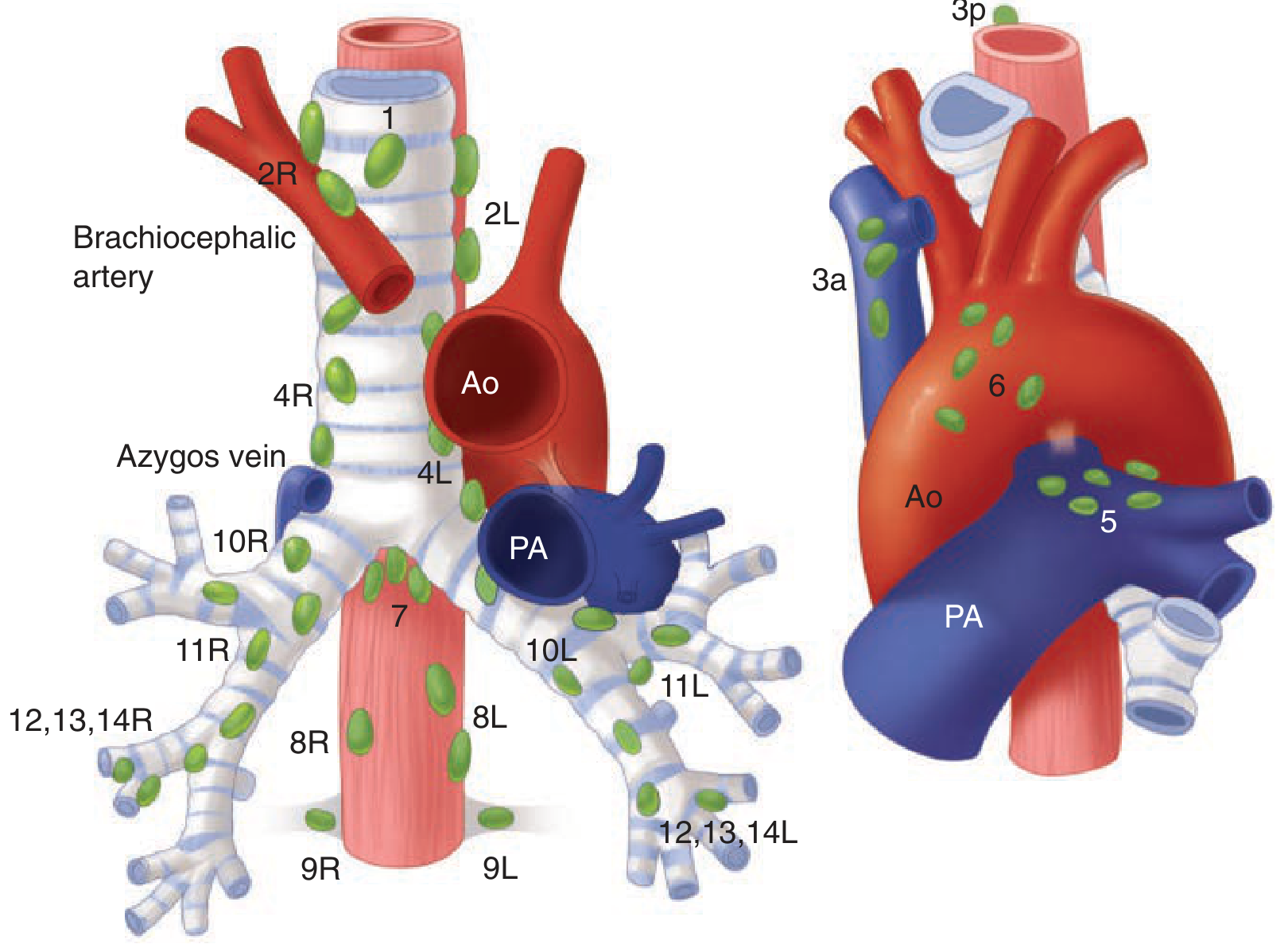
IASLC lymph node station map - Schwartz's Principles of Surgery, 11th ed.
N1 Nodes (Pulmonary / Ipsilateral Hilar)
These are intrathoracic nodes on the same side as the tumor, within the lung or at the hilum:
| Group | Location |
|---|---|
| Intrapulmonary/Segmental (12-14) | At bifurcations of segmental bronchi or pulmonary artery |
| Lobar (11) | Along upper, middle, and lower lobe bronchi |
| Interlobar (11) | In the angles formed where main bronchi bifurcate into lobar bronchi - "Lymphatic Sump of Borrie" |
| Hilar (10) | Along the main bronchi at the hilum |
Lymphatic Sump of Borrie - a key concept:
- The interlobar nodes in the depths of the interlobar fissure form a "sump" that receives drainage from ALL lobes of the corresponding lung
- On the right: nodes lie around the bronchus intermedius (bounded above by the right upper lobe bronchus, below by the middle and superior segmental bronchi)
- On the left: nodes lie in the angle between the lingular and lower lobe bronchi
- These nodes are in close proximity to pulmonary arterial branches - must be carefully dissected during lobectomy
N2 Nodes (Ipsilateral Mediastinal)
Four main groups within the mediastinum on the same side:
| Group | Location |
|---|---|
| Anterior mediastinal (3a, 5, 6) | Along upper pericardium, phrenic nerves, ligamentum arteriosum, and left aspect of innominate vein |
| Posterior mediastinal (8, 9) | Paraesophageal nodes within inferior pulmonary ligament; between esophagus and trachea near the azygos arch |
| Tracheobronchial (4, 7) | Three subgroups: subcarinal nodes (station 7, in the obtuse angle between trachea and each main stem bronchus) + nodes anterior to the lower trachea |
| Paratracheal (1, 2, 4) | Alongside the trachea in the superior mediastinum |
On the right: Paratracheal nodes form a chain with tracheobronchial nodes inferiorly and scalene nodes (deep cervical) above.
N3 Nodes (Contralateral / Supraclavicular)
- Contralateral mediastinal or hilar nodes
- Ipsilateral or contralateral scalene/supraclavicular nodes
Final Efferent Drainage
- Right lung lymph drains via the right lymphatic trunk into the right venous angle (junction of right internal jugular and subclavian veins)
- Left lung lymph drains into the thoracic duct, which empties into the left venous angle
Direction of Lymphatic Flow (Clinically Important Asymmetry)
| Side | Pattern of Mediastinal Drainage |
|---|---|
| Right lung | Ipsilateral (right-sided) drainage to mediastinal nodes; occasional bilateral drainage to superior mediastinum |
| Left lung | Particularly the left lower lobe - drainage occurs with equal frequency to ipsilateral AND contralateral (right-sided) superior mediastinal nodes |
Clinical significance: Left lower lobe lung cancer can spread to right-sided mediastinal nodes. This explains why contralateral mediastinal staging is important for left-sided tumors.
Applied Anatomy
1. Lung Cancer Staging (N-Descriptor)
Understanding lymph node stations is fundamental to TNM staging of non-small cell lung cancer (NSCLC):
- N0: No regional node involvement
- N1: Metastasis to ipsilateral intrapulmonary, lobar, interlobar, or hilar nodes (stations 10-14)
- N2: Metastasis to ipsilateral mediastinal or subcarinal nodes (stations 1-9)
- N3: Contralateral mediastinal/hilar nodes; ipsilateral or contralateral scalene/supraclavicular nodes
One-quarter to one-half of NSCLC patients have mediastinal lymph node metastases at diagnosis. Accurate staging requires adequate segmental, hilar, and mediastinal lymph node sampling - ideally a complete mediastinal lymph node dissection.
Mediastinal staging techniques: EBUS (endobronchial ultrasound), EUS-FNA (endoscopic ultrasound guided fine needle aspiration), mediastinoscopy, mediastinotomy, thoracoscopy.
The Lymphatic Sump of Borrie is surgically important: all lobes drain here, so a tumor in any lobe can spread to the interlobar nodes. These must be dissected carefully to identify pulmonary arterial branches during lung resection.
2. Pulmonary Edema
In the normal lung, fluid balance is governed by Starling forces (hydrostatic vs. oncotic pressure). Lymphatics maintain lung fluid homeostasis by draining excess interstitial fluid.
- At baseline (normal slow entry rate), lymphatics handle this drainage adequately
- In pulmonary edema (raised hydrostatic pressure - e.g., heart failure, ARDS), lymphatic flow increases substantially
- When lymphatic capacity is overwhelmed or impaired, interstitial and then alveolar edema follows
- The pulmonary lymphatics are most important in drainage during injury and inflammation, not at steady state
Post-lung transplantation: Disruption of lymphatic drainage increases extravascular lung water, predisposing the transplanted lung to pulmonary edema - fluid overload must be strictly avoided post-transplant.
3. Pleural Effusion
- Parietal pleural lymphatics drain the pleural fluid (not the visceral pleural lymphatics, which do not connect to the pleural space)
- At baseline, limited impairment of pleural lymphatic drainage has little consequence
- When fluid entry into the pleural space increases (e.g., heart failure, malignancy, infection), any limitation in lymphatic drainage contributes directly to pleural effusion formation
- Malignant pleural effusion: Lymph node obstruction by metastatic tumor blocks efferent lymphatic channels, raising pressure and promoting fluid accumulation
4. Chylothorax
- Results from disruption or obstruction of the thoracic duct or its major tributaries
- Causes: iatrogenic injury (esophagectomy, thoracic surgery), blunt trauma, malignancy (especially lymphoma), granulomatous disease (sarcoidosis), lymphangioleiomyomatosis
- Presents as milky pleural effusion on resumption of oral intake
- Diagnosis: pleural fluid triglycerides >110 mg/dL, lymphocyte predominance
- Management: chest drain for lung re-expansion, nil by mouth, somatostatin analogs; if high output persists (>50 mL/day), surgical ligation of the thoracic duct
5. Primary Tuberculosis (Ghon Complex)
In primary tuberculosis, the organism seeds the lung parenchyma, typically in the mid-zone (Ghon focus). The lymphatics carry mycobacteria to the regional lymph nodes at the hilum and mediastinum, producing lymphadenopathy. Together, the parenchymal focus + enlarged hilar/mediastinal nodes = the Ghon complex (or "primary complex"). Understanding the lymphatic drainage route explains:
- Why hilar lymphadenopathy is a hallmark of primary TB
- How mediastinal compression (of airways, veins, esophagus) can occur from massive adenopathy
- Why the infection can spread via lymphatics to other organs (miliary TB) when lymph node barriers are breached
6. Immune Surveillance and Antigen Trafficking
- The lung is constantly exposed to environmental antigens and pathogens
- Antigen-presenting cells (dendritic cells, macrophages) sample inhaled particles and migrate via the lymphatics to mediastinal lymph nodes, where adaptive immune responses are initiated
- This migration is mediated by CCL21 (on lymphatic endothelium) and its receptor CCR7 (on T cells and dendritic cells)
- Migration from airways to mediastinal nodes takes ~1-2 days
- This lymphatic route is the basis of T-cell sensitization in tuberculosis, sarcoidosis, and hypersensitivity pneumonitis
7. Sarcoidosis
- Characterized by non-caseating granuloma formation in hilar and mediastinal lymph nodes
- Bilateral hilar lymphadenopathy (BHL) - the classic radiological finding - reflects sarcoid involvement of the lymph nodes that are the primary drainage sites for lung lymph
- Increased FDG uptake on PET in mediastinal and hilar lymph nodes is characteristic
8. Lymphangitis Carcinomatosa
- Malignant cells spread via lymphatics into the peribronchial and perivascular lymphatics throughout the lung
- Produces characteristic radiological pattern of bilateral linear ("Kerley B") lines and ground-glass opacification
- Can occur with any adenocarcinoma but is classic with breast, stomach, and lung primaries
- Severely impairs lymphatic drainage capacity, contributing to interstitial edema and breathlessness
9. Surgical Relevance (Pneumonectomy / Lobectomy)
- Complete mediastinal lymph node dissection (MLND) is performed at lung resection for cancer
- The Lymphatic Sump of Borrie must be dissected to expose lobar and segmental pulmonary artery branches
- Cross-drainage from the left lower lobe to right-sided mediastinal nodes means left lower lobe tumors can be understaged if only ipsilateral mediastinal sampling is performed
Summary Table: Key Lymph Node Groups
| Station | Name | Group |
|---|---|---|
| 1 | Highest mediastinal | N2 |
| 2R/2L | Upper paratracheal | N2 |
| 3a | Pre-vascular | N2 |
| 3p | Retrotracheal | N2 |
| 4R/4L | Lower paratracheal | N2 |
| 5 | Subaortic (AP window) | N2 (left only) |
| 6 | Para-aortic | N2 (left only) |
| 7 | Subcarinal | N2 |
| 8R/8L | Paraesophageal | N2 |
| 9R/9L | Pulmonary ligament | N2 |
| 10R/10L | Hilar | N1 |
| 11R/11L | Interlobar | N1 |
| 12R/12L | Lobar | N1 |
| 13R/13L | Segmental | N1 |
| 14R/14L | Subsegmental | N1 |
Sources
- Schwartz's Principles of Surgery, 11th ed. (Lymphatic Drainage section, pp. 694-695)
- Murray & Nadel's Textbook of Respiratory Medicine (Chapter 7: Pulmonary Lymphatics)
- Harrison's Principles of Internal Medicine, 22nd ed. (Anatomic Staging of Lung Cancer)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Lymphatic Vessels of the Lung, p. 1817)
- Schwartz's Principles of Surgery (Chylothorax management, p. 3613)
This is a shared conversation. Sign in to Orris to start your own chat.