





I have seminar to explain for my prof this slide I need to explain and gat me the beat step to gat the full mark from the evaluation
🎓 Complete Seminar Guide: DKA Treatment
SLIDE 1 - Treatment Overview
"DKA is a life-threatening medical emergency. The patient must be admitted to a hospital - ideally a high-dependency unit - with a diabetes specialist team involved as early as possible. Clinical and lab monitoring is essential throughout the first 24 hours. For high-risk patients - specifically those aged 18-25, elderly, pregnant women, or anyone with heart or kidney failure - early specialist involvement is not optional, it is mandatory."
- You show you understand why it's an emergency, not just that it is
- Mentioning high-risk groups specifically shows depth of knowledge
SLIDE 2 - Fluid Replacement (Types & Rationale)
"Fluid replacement is the first and most urgent intervention. We use 0.9% isotonic saline (normal saline) as the default fluid of choice because DKA patients are severely volume depleted from osmotic diuresis and vomiting. However, if the patient's plasma sodium is above 155 mmol/L, we switch to 0.45% (half-normal) saline to avoid worsening hypernatremia. A critical point: in children and young adults, we must be cautious with rapid fluid administration because it is a major risk factor for cerebral edema - a life-threatening complication."
| Condition | Fluid |
|---|---|
| Default | 0.9% NaCl (isotonic saline) |
| Sodium > 155 mmol/L | 0.45% NaCl (half-normal saline) |
| Glucose falls below 14 mmol/L | Add 10% glucose alongside saline |
SLIDE 3 - Fluid Schedule & Glucose Introduction
"The fluid restoration schedule follows a specific protocol. We start aggressively: 1 liter in the first 30 minutes, then 1 liter over the next hour, then 1 liter over 2 hours, then 1 liter every 4 hours based on hydration status. The total target in 24 hours is approximately 6 liters - but in elderly patients we must avoid fluid overload. Once the patient is euvolemic (stable volume), we switch to half-normal saline at 150-200 mL/hour."
"Once blood glucose drops below 14 mmol/L, we introduce 10% glucose - not to stop saline, but to run both at the same time. This is important: we need to keep insulin running to clear ketones, and glucose prevents hypoglycemia."
SLIDE 4 - Insulin Therapy
"Insulin is the second pillar of DKA treatment. The standard route is intravenous infusion at 0.1 U/kg/hour. If IV access is not available, we can use intramuscular injection - a loading dose of 10-20 units followed by 5 units hourly. Alternatively, subcutaneous fast-acting insulin analogues can be used: 0.3 U/kg initially, then 0.1 U/kg hourly."
"We monitor the response to insulin by tracking two values: blood glucose should fall by 3-6 mmol/L per hour, and blood ketones should fall by at least 0.5 mmol/L per hour. We must avoid rapid correction - falling too fast risks hypoglycemia and cerebral edema, especially in children."
| Parameter | Target Rate of Reduction |
|---|---|
| Blood glucose | 3-6 mmol/L per hour |
| Blood ketones | ≥ 0.5 mmol/L per hour |
SLIDE 5 - Potassium Management
"Potassium is one of the most dangerous electrolyte problems in DKA. Both hypokalemia and hyperkalemia can be fatal - they cause cardiac arrhythmias. Here is the key clinical point: we do NOT give potassium in the very first liter of fluid, because the patient may have pre-renal failure from dehydration, and adding potassium too early can cause dangerous hyperkalemia."
"Once urine output is confirmed and serum potassium is below 5.5 mmol/L, we add 40 mmol/L of potassium chloride to the 0.9% saline. Our target range is 4.0 to 5.5 mmol/L. If potassium drops below 3.5 mmol/L, the replacement regimen must be urgently reviewed. Continuous cardiac monitoring (ECG) is required in severe DKA."
SLIDE 6 - Bicarbonate, Phosphate & Magnesium
"Bicarbonate is NOT routinely recommended in DKA - and this is counterintuitive because the patient is acidotic. The reason is threefold: first, adequate fluids and insulin will correct the acidosis on their own. Second, acidosis may actually be adaptive - it shifts the oxygen dissociation curve to improve oxygen delivery to tissues. Third, and most dangerously, bicarbonate can paradoxically worsen CSF acidosis and has been linked to cerebral edema in children and young adults."
"For phosphate and magnesium - no routine replacement is needed. Replace only if lab levels are confirmed to be low."
SLIDE 7 - Monitoring
"Monitoring in DKA is continuous and structured. Every hour: pulse, blood pressure, respiratory rate, urine output, neurological status. Blood glucose is monitored hourly until the anion gap normalizes, then every 4-6 hours. Serum electrolytes are checked every 4 hours. On admission, we do BUN and creatinine to assess renal function, and arterial blood gas (ABG) to quantify the severity of acidosis."
"Cardiac monitoring with ECG is essential - we need to catch potassium-related arrhythmias early. Continuous cardiac monitoring during electrolyte correction is strongly advisable."
SLIDE 8 - Complications
"DKA can damage multiple organ systems. Acute complications include cerebral edema, ARDS, acute kidney injury (AKI), thromboembolism, and metabolic abnormalities like hypokalemia and hypoglycemia. Chronic complications from severe episodes include cognitive impairment and cardiovascular disease. Late complications - especially in elderly patients - include pneumonia and thromboembolism. And treatment itself can cause complications: the two most common are hypoglycemia and hypokalemia, both from insulin and fluid therapy."
SLIDE 9 - Cerebral Edema
"Cerebral edema is the most feared acute complication of DKA. It is rare - under 1% incidence - but carries a mortality rate of 20-50%. It is most common in children under 5 and young adults. It typically occurs in the first 24 hours of treatment, especially when fluids are given too rapidly."
"Early symptoms: severe headache, blurred vision, irritability, vomiting. Advanced signs: papilledema, seizures, altered consciousness, focal neurological deficits. In the worst cases: coma, respiratory arrest, raised intracranial pressure signs - the Cushing triad of bradycardia, hypertension, and irregular breathing."
"Diagnosis is clinical first - physical exam and ophthalmoscopy to check for papilledema. MRI confirms it. Management: immediately slow down IV fluids, give IV mannitol 0.5-1 g/kg over 20 minutes. If no response in 30-120 minutes, repeat the mannitol or give hypertonic saline 3% at 5-10 mg/kg over 30 minutes. Severe cases need intubation and mechanical ventilation."
TOP TIPS TO GET FULL MARKS
- Always explain the "why" - not just what the treatment is, but why we do it (e.g., why we add glucose at 14 mmol/L, why we don't give bicarbonate, why we delay potassium)
- Use exact numbers - professors love when you cite doses, thresholds, and timeframes precisely (0.1 U/kg/hr insulin, 6 L in 24 hrs, K+ target 4.0-5.5 mmol/L)
- Connect complications to mechanism - e.g., "rapid fluid correction causes osmotic shifts leading to cerebral edema"
- Organize your answer - say "There are 3 reasons..." or "We manage this in 2 steps..." This shows structured thinking
- Anticipate questions - professors often ask: "Why not bicarbonate?" / "Why delay potassium?" / "What is the danger in children?" - prepare clear 2-sentence answers for each
- Mention monitoring alongside each treatment - showing you know how to track the response to each intervention is a sign of clinical maturity
Create a DKA treatment decision tree flowchart to use in your seminar
A clean professional medical flowchart titled "DKA Treatment Decision Tree" for a university seminar. The flowchart uses a top-down layout with color-coded boxes and arrows. Structure: TOP: Red box "SUSPECTED DKA" → Arrow down to diagnostic criteria box (glucose >11 mmol/L, ketones >3 mmol/L, pH <7.3 / HCO3 <15) Then splits into two parallel tracks side by side: LEFT TRACK (Blue header "1. FLUID RESUSCITATION"): - Box: "0.9% Normal Saline" - Schedule: 1L/30min → 1L/1hr → 1L/2hr → 1L/4hr - Diamond decision: "Sodium >155 mmol/L?" → YES → "Switch to 0.45% saline" / NO → Continue 0.9% - Diamond decision: "Blood glucose <14 mmol/L?" → YES → "Add 10% glucose (run alongside saline)" - Box: "Total: ~6L in 24hrs (caution in elderly)" MIDDLE TRACK (Green header "2. INSULIN THERAPY"): - Box: "IV Infusion: 0.1 U/kg/hr" - Diamond: "IV access available?" → NO → "IM: 10-20U loading, then 5U/hr" or "SC: 0.3U/kg then 0.1U/kg/hr" - Box: "Monitor response:" with "Glucose ↓ 3-6 mmol/L/hr" and "Ketones ↓ ≥0.5 mmol/L/hr" - Warning box (orange): "Avoid rapid decrease → risk of hypoglycemia & cerebral edema" RIGHT TRACK (Purple header "3. POTASSIUM"): - Box: "Do NOT give K+ in first litre" - Diamond: "K+ <5.5 mmol/L AND urine output confirmed?" → YES → "Add 40 mmol/L KCl to 0.9% saline" - Box: "Target K+: 4.0–5.5 mmol/L" - Warning: "If K+ <3.5 → review regimen urgently" - Box: "ECG monitoring in severe DKA" BOTTOM SECTION (unified): - Orange box "MONITORING (Hourly)": BP, HR, RR, urine output, glucose, neuro status, electrolytes q4h, ABG - Red box "WATCH FOR CEREBRAL EDEMA": Headache, vomiting, altered consciousness → Slow IV fluids + IV Mannitol 0.5–1 g/kg - Green box "RESOLUTION CRITERIA": Normal anion gap, pH >7.3, ketones <0.3 mmol/L Clean white background, professional font, color-coded sections, clear arrows, suitable for a medical seminar presentation
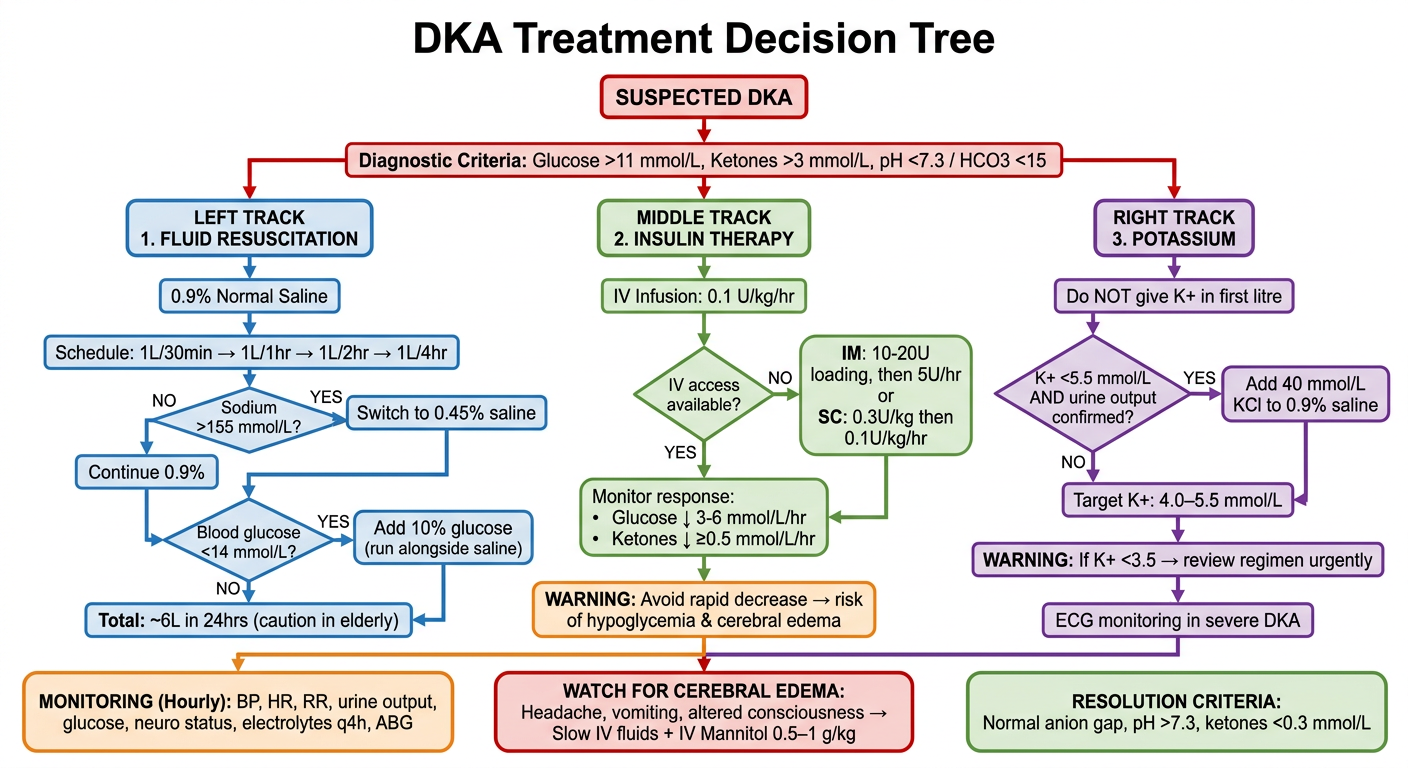
- 🔵 Blue - Fluid Resuscitation (with decision points for sodium level and glucose threshold)
- 🟢 Green - Insulin Therapy (IV, IM, and SC routes with monitoring targets)
- 🟣 Purple - Potassium Management (with safety checkpoints)
- 🟠 Orange - Hourly Monitoring parameters
- 🔴 Red - Cerebral Edema alert and resolution criteria at the bottom
- Display it as a reference visual while you talk through each section
- Use it to show the professor that you understand the decision logic behind each step, not just the facts
- Point to the decision diamonds (the "Yes/No" boxes) to demonstrate clinical reasoning - this is what earns top marks
Can you explain to my every one in this chart acording to the color
🔴 RED - "SUSPECTED DKA" (Top Box)
- Blood glucose > 11 mmol/L
- Ketones > 3 mmol/L
- Blood pH < 7.3 OR bicarbonate < 15 mmol/L
🔵 BLUE - Fluid Resuscitation (Left Track)
- Default: 0.9% Normal Saline for everyone
- If sodium is > 155 mmol/L → switch to 0.45% saline to avoid worsening the high sodium
| Time | Volume |
|---|---|
| First 30 minutes | 1 liter |
| Next 1 hour | 1 liter |
| Following 2 hours | 1 liter |
| Every 4 hours after | 1 liter |
| Total in 24 hours | ~6 liters |
- When blood glucose drops below 14 mmol/L → add 10% glucose running alongside the saline
- You do NOT stop the saline - you run both at the same time
- This prevents hypoglycemia while insulin keeps working to clear ketones
🟢 GREEN - Insulin Therapy (Middle Track)
- Intramuscular (IM): Loading dose of 10-20 units, then 5 units every hour
- Subcutaneous (SC): 0.3 U/kg initially, then 0.1 U/kg every hour (fast-acting analogue only)
- Blood glucose must fall by 3-6 mmol/L per hour
- Blood ketones must fall by at least 0.5 mmol/L per hour
🟣 PURPLE - Potassium Management (Right Track)
- Is K+ below 5.5 mmol/L AND is the patient passing urine?
- If YES → add 40 mmol/L of KCl to the 0.9% saline bag
🟠 ORANGE - Monitoring (Bottom Left)
- Pulse, Blood Pressure, Respiratory Rate, Urine Output
- Blood glucose (hourly until stable, then every 4-6 hours)
- Neurological status and mental state
- Serum electrolytes every 4 hours
- ABG on admission and as needed
- Blood ketones (optional but helpful to track DKA resolution)
- ECG - continuous cardiac monitoring during electrolyte correction
🔴 RED - Cerebral Edema Alert (Bottom Right)
- Severe headache, blurred vision, vomiting (early)
- Papilledema, seizures, altered consciousness (progressing)
- Bradycardia + hypertension + irregular breathing = raised intracranial pressure (late/severe)
- Slow down IV fluids immediately
- Give IV Mannitol 0.5-1 g/kg over 20 minutes to reduce brain swelling
- If no response in 30-120 minutes → repeat mannitol OR give 3% hypertonic saline at 5-10 mg/kg over 30 minutes
- Severe cases → intubation and mechanical ventilation
🟢 GREEN - Resolution Criteria (Bottom Center)
- pH > 7.3 (acidosis corrected)
- Ketones < 0.3 mmol/L (ketosis cleared)
- Normal anion gap (metabolic balance restored)
Quick Color Summary Card
| Color | Section | Priority |
|---|---|---|
| 🔴 Red (top) | Diagnosis | First - confirm before treating |
| 🔵 Blue | Fluids | Start immediately |
| 🟢 Green | Insulin | Start after fluids are running |
| 🟣 Purple | Potassium | Check before insulin, replace carefully |
| 🟠 Orange | Monitoring | Continuous throughout |
| 🔴 Red (bottom) | Cerebral Edema | Watch for, act fast |
| 🟢 Green (bottom) | Resolution | Goal of all treatment |