Give medical images for the topic dermoid cyst, molar and tubal pregnancy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive medical image gallery for all three topics, sourced from authoritative textbooks.
Dermoid Cyst
Image 1 - Laparoscopic Appearance (Ovarian Dermoid Cyst)
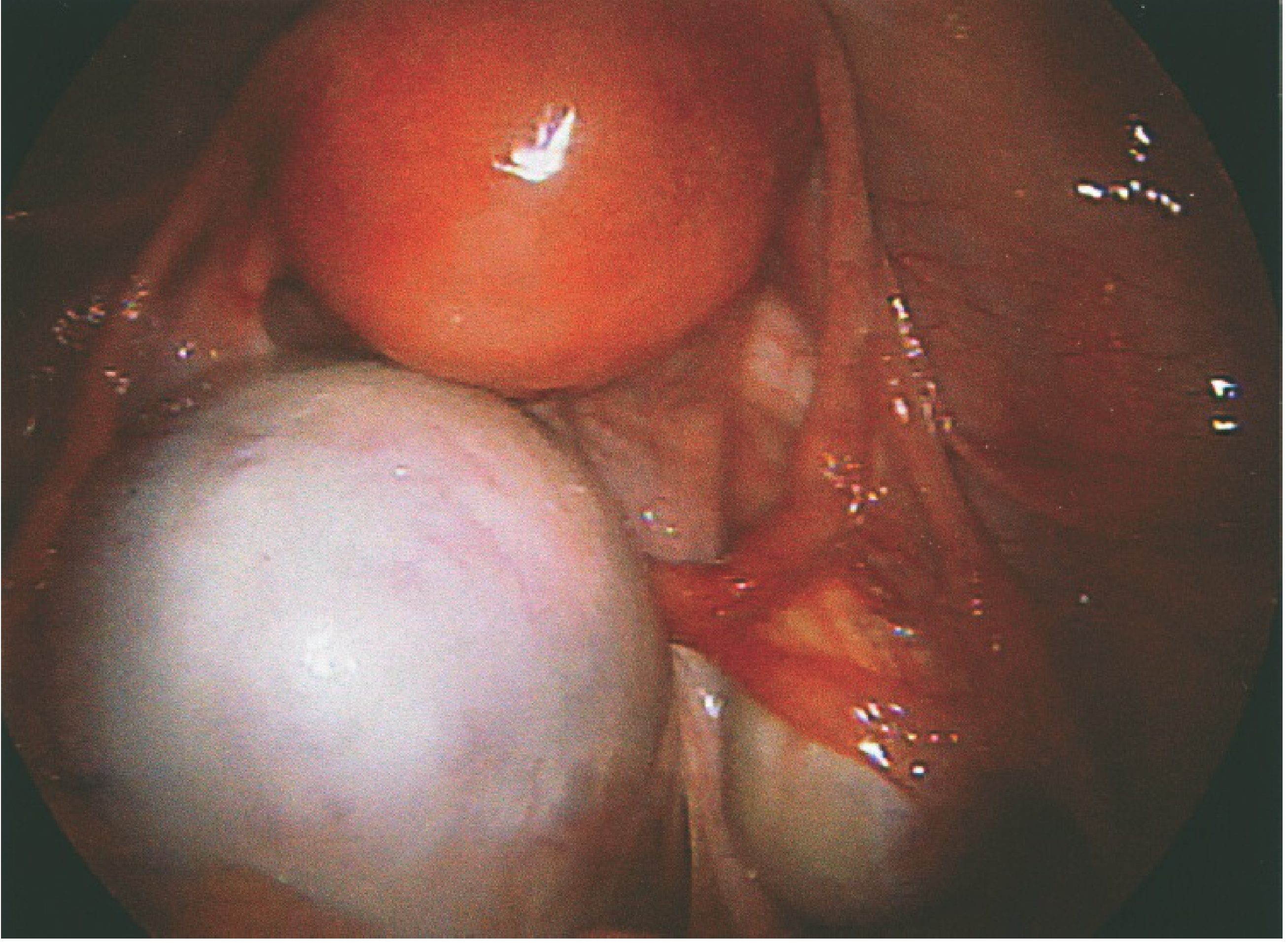
Fig. 1 Laparoscopic appearance of a benign ovarian dermoid cyst. Note the characteristic pearly-white, smooth-walled cystic structure adjacent to ovarian tissue. The dermoid (below) contrasts clearly with the normal ovarian tissue (above).
Source: Berek & Novak's Gynecology, Fig. 10-11
Image 2 - MRI of Dermoid Cyst (T1-weighted, Axial)
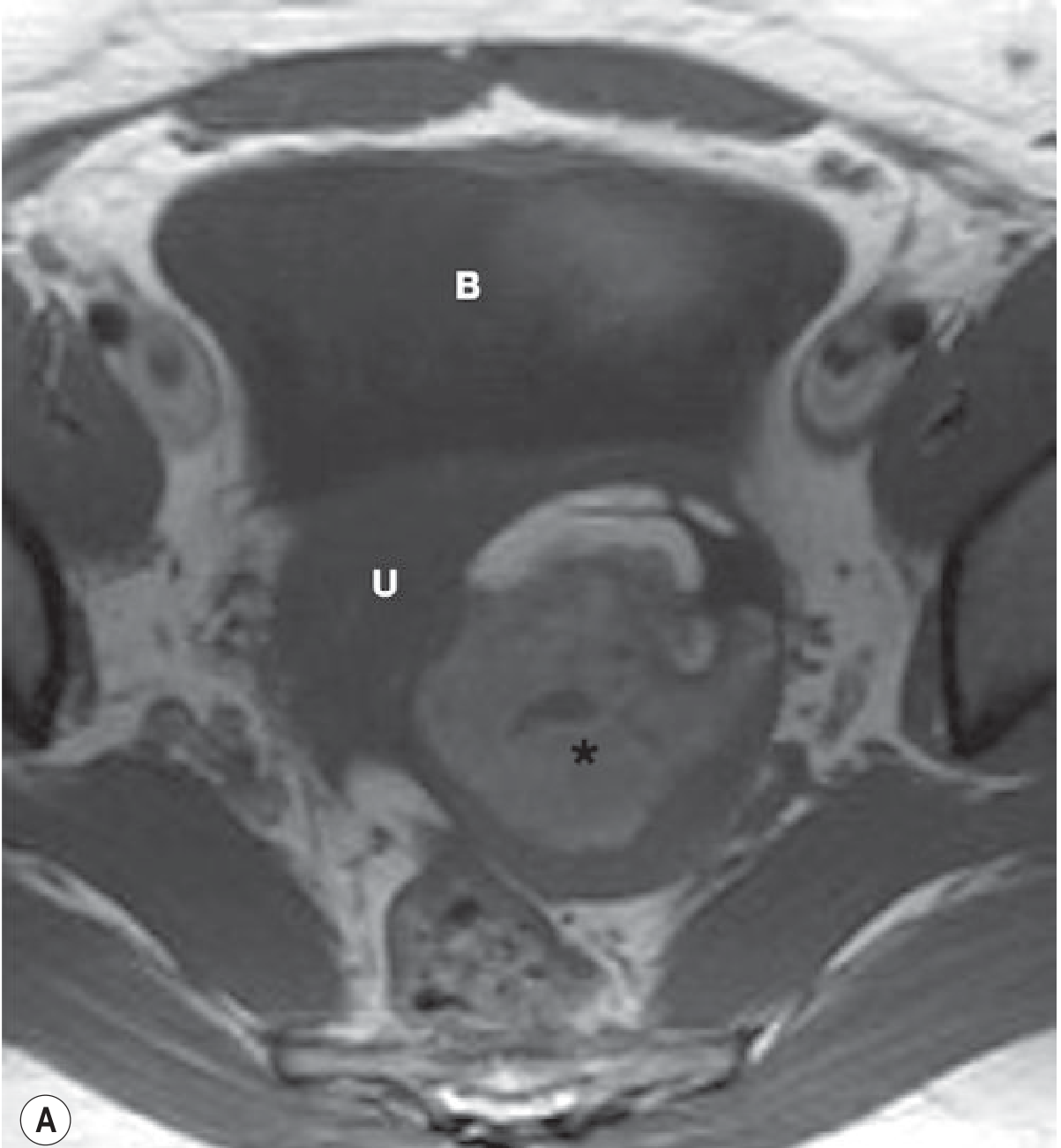
Fig. 2 MRI T1-weighted axial image of a dermoid cyst. The left adnexal mass (asterisk) shows areas of high signal intensity on T1-weighted imaging due to fatty content. B = Bladder; U = Uterus. On fat-suppression sequences, the high signal from the fat component is suppressed, confirming the diagnosis.
Source: Grainger & Allison's Diagnostic Radiology, Fig. 35.39A
Image 3 - Ultrasound of Dermoid Cyst (Torted)
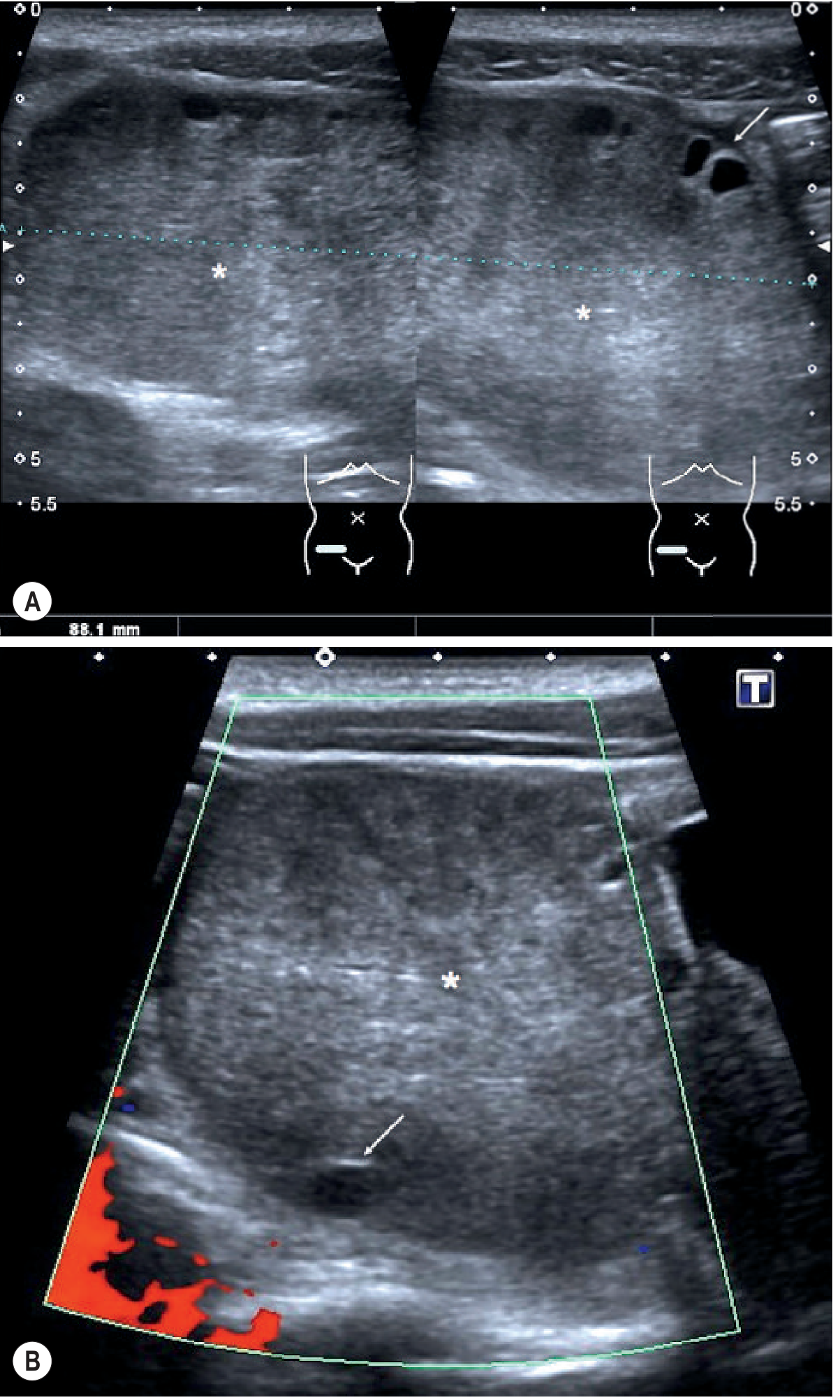
Fig. 3 Ultrasound of a torted ovarian dermoid. (A) Transverse and longitudinal transabdominal US images demonstrate the echogenic central ovarian stroma (asterisk) and peripherally displaced follicles (arrow). (B) Colour Doppler shows absent vascularity - a feature of torsion.
Source: Grainger & Allison's Diagnostic Radiology, Fig. 35.40
Image 4 - MRI Torsion of Ovarian Dermoid (T2W + Contrast)
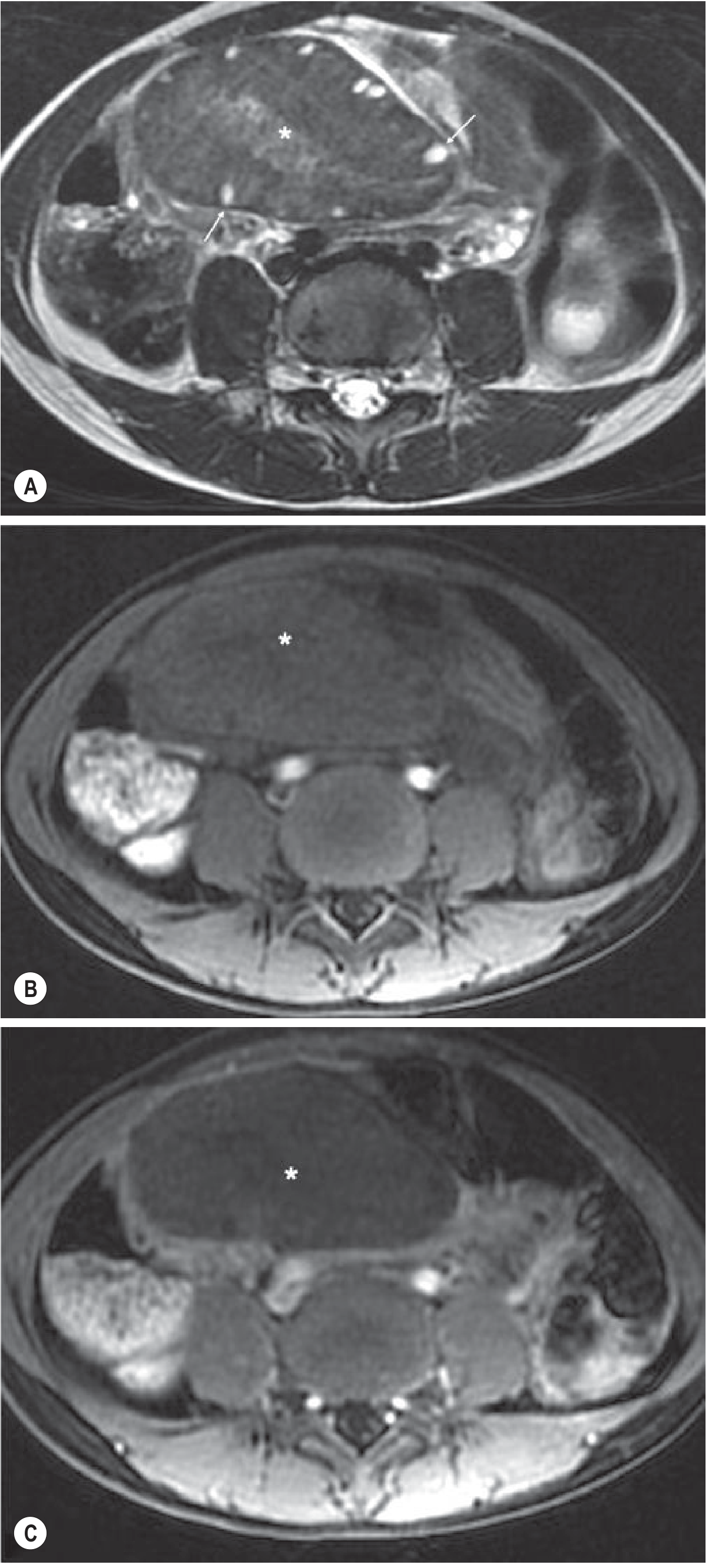
Fig. 4 MRI of torsion of an ovarian dermoid. (A) Axial T2-weighted MRI shows enlarged right ovary with increased T2 signal in the stroma (asterisk) and peripheral follicles displaced to the rim (arrows). (B) Pre-contrast and (C) post-contrast MRI demonstrate no enhancement within the torted dermoid (asterisk), confirming compromised vascular supply.
Source: Grainger & Allison's Diagnostic Radiology, Fig. 35.41
Molar Pregnancy (Hydatidiform Mole)
Image 5 - Pathogenesis Diagram: Complete vs Partial Mole
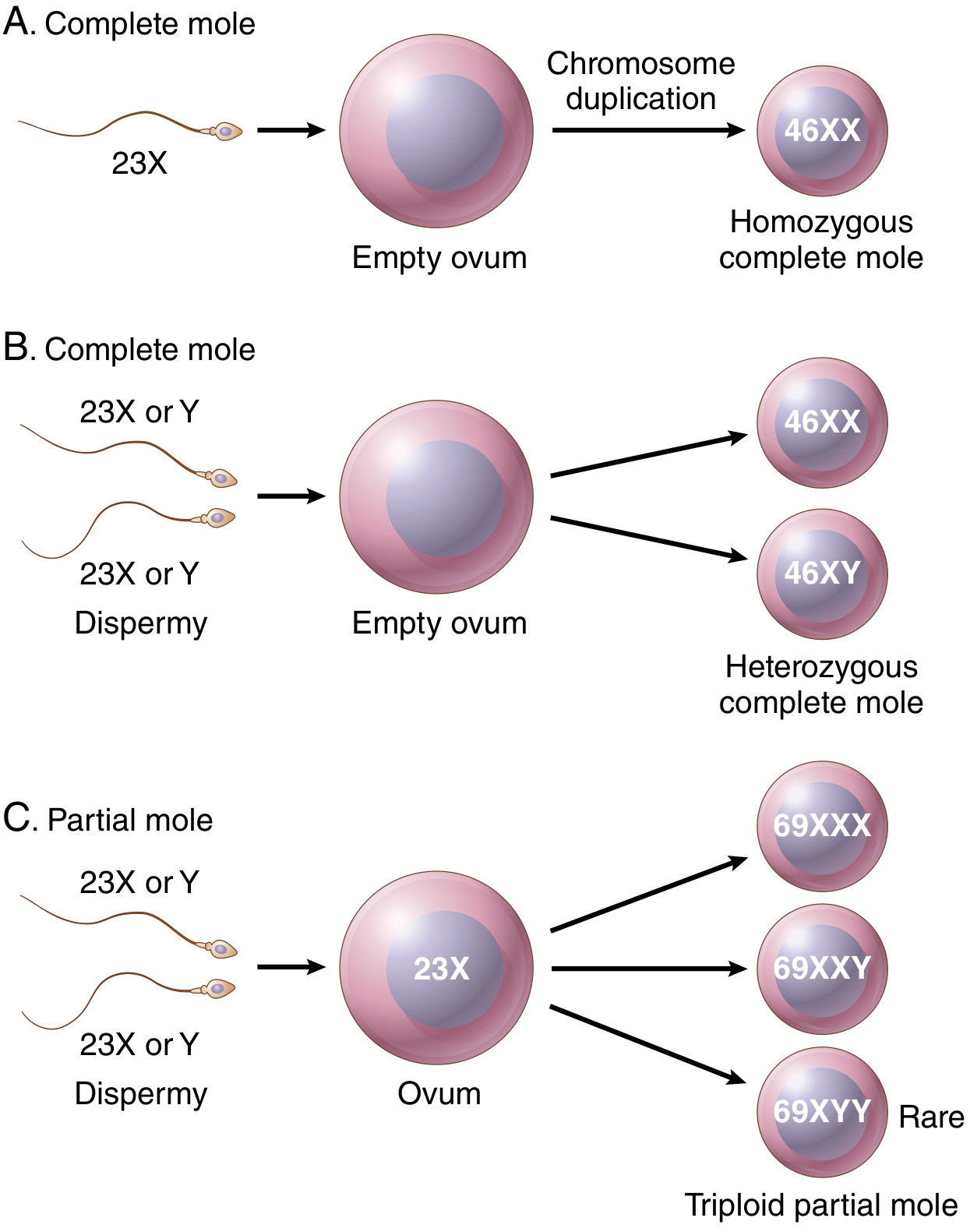
Fig. 5 Origin of complete and partial hydatidiform moles.
- (A) Complete mole (monospermic): a single sperm fertilizes an empty ovum, then undergoes chromosome duplication → 46XX karyotype.
- (B) Complete mole (dispermic): two sperm fertilize an empty ovum → 46XX or 46XY karyotype.
- (C) Partial mole: two sperm fertilize a normal ovum → triploid karyotype (69XXX, 69XXY, or 69XYY). Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 22.53
Image 6 - Gross and Histology of Complete Hydatidiform Mole
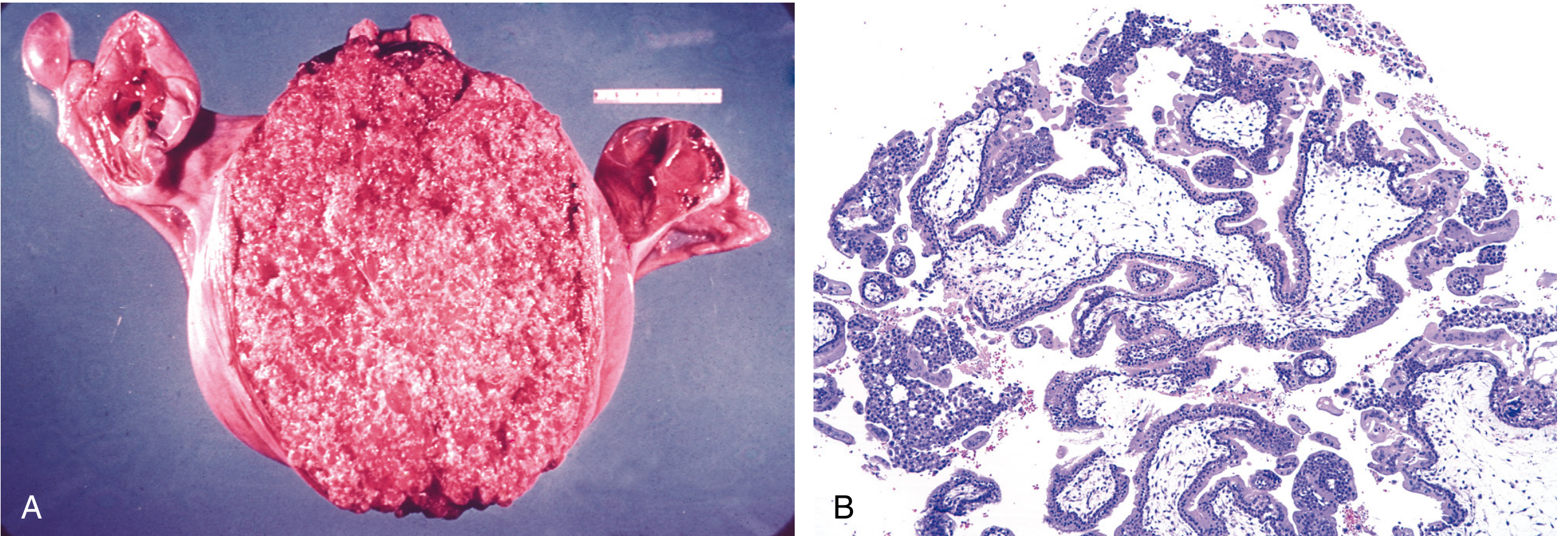
Fig. 6 Complete hydatidiform mole.
- (A) Gross specimen: the uterus is markedly distended by enlarged, vesicular, grape-like chorionic villi filling the endometrial cavity. The adnexa (ovaries and fallopian tubes) are visible on both sides.
- (B) Histology (H&E): marked villous enlargement, stromal edema with central cisternae, and circumferential trophoblast proliferation involving both cytotrophoblasts and syncytiotrophoblasts. Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 22.54
Image 7 - Histology of Partial Hydatidiform Mole
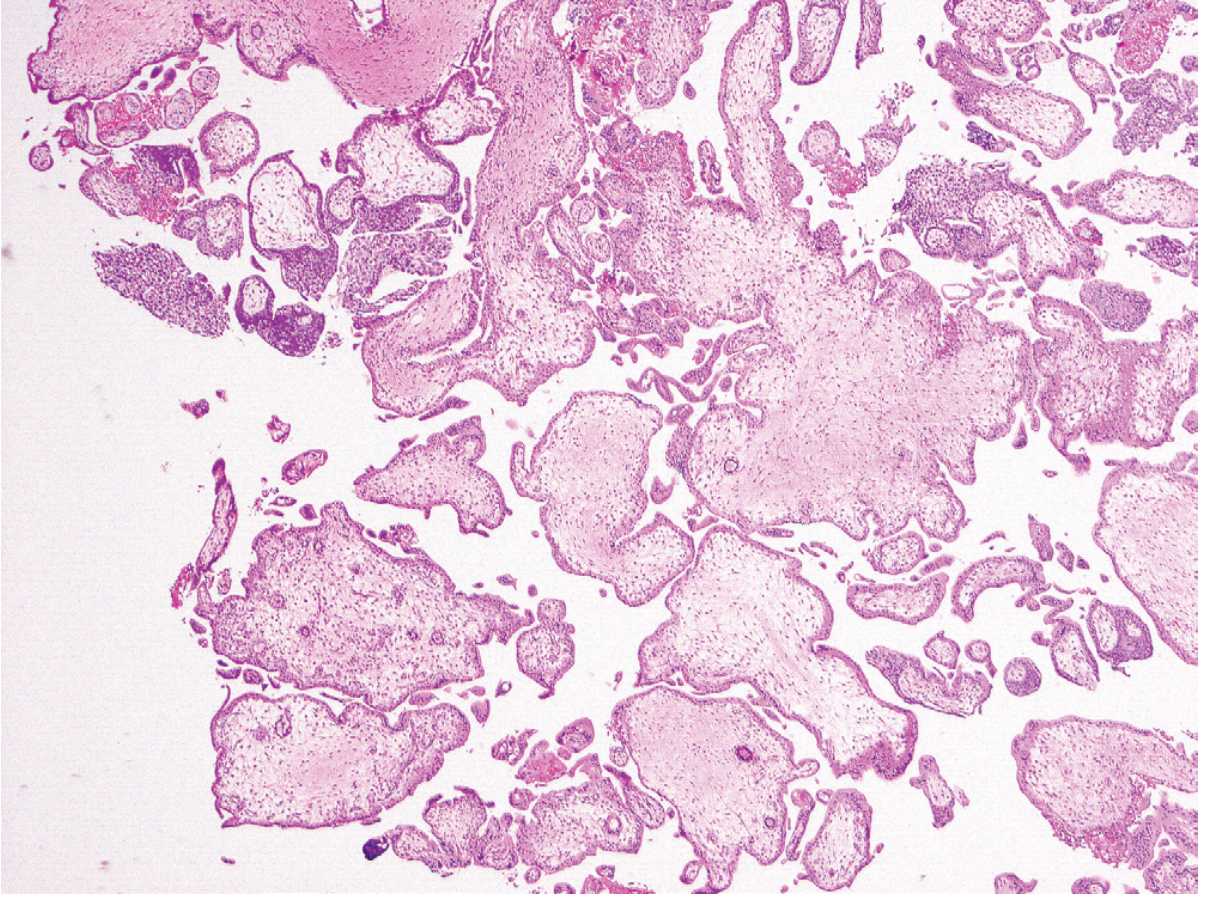
Fig. 7 Partial hydatidiform mole (H&E histology). Only a fraction of villi are enlarged with irregular, scalloped outlines (unlike the smooth round outline of complete moles). Syncytiotrophoblastic inclusions and focal trophoblastic hyperplasia are present. This partial mole was confirmed triploid.
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 22.55
Image 8 - Histology Partial Mole (Berek & Novak)
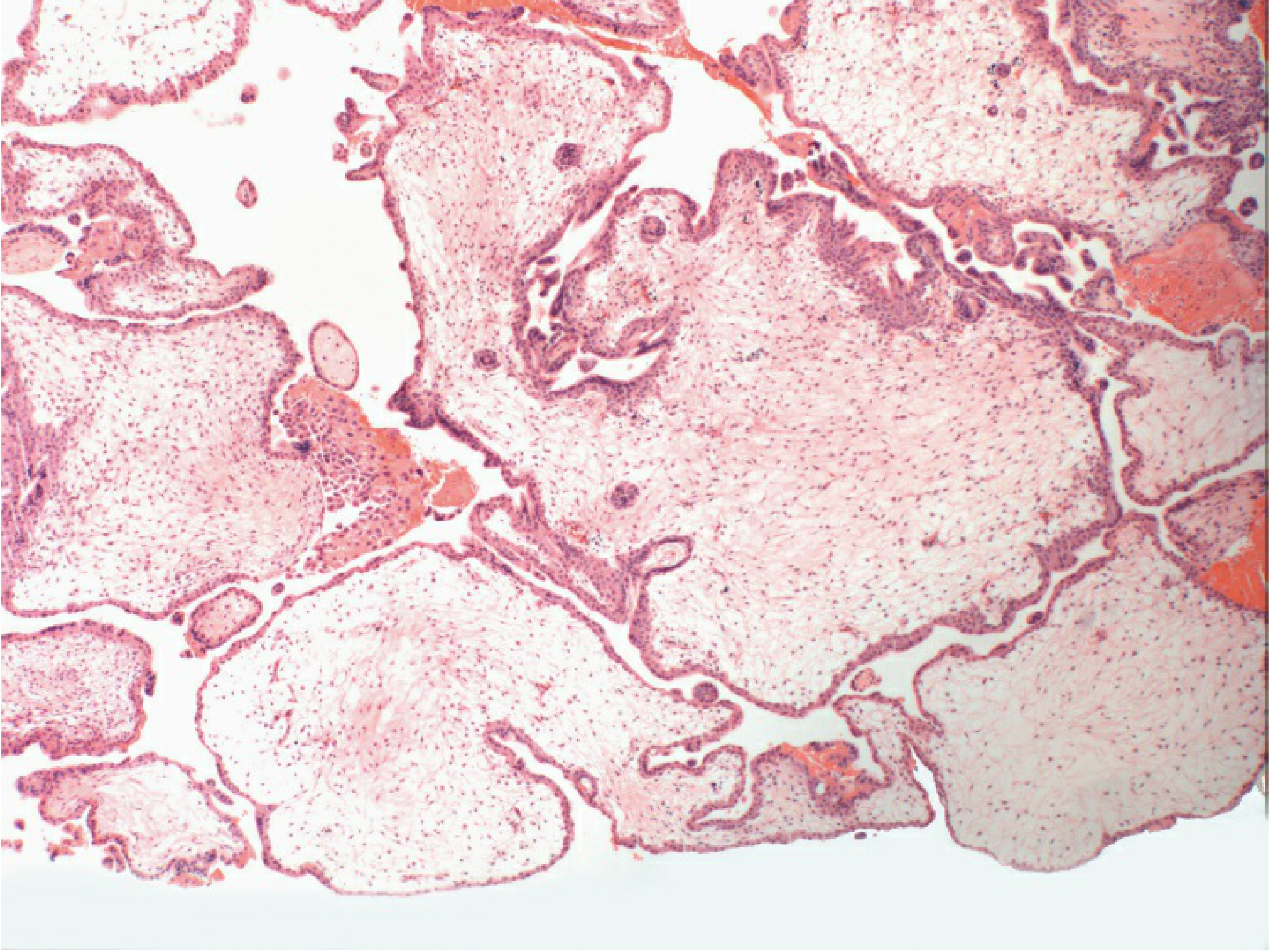
Fig. 8 Photomicrograph of a partial mole showing marked disparity in villous size, trophoblastic inclusions (center), and mild trophoblastic hyperplasia. The mixture of normal and abnormal-sized villi is a key distinguishing feature from complete mole.
Source: Berek & Novak's Gynecology, Fig. 41-3
Tubal (Ectopic) Pregnancy
Image 9 - Gross Pathology: Ruptured Tubal Ectopic Pregnancy
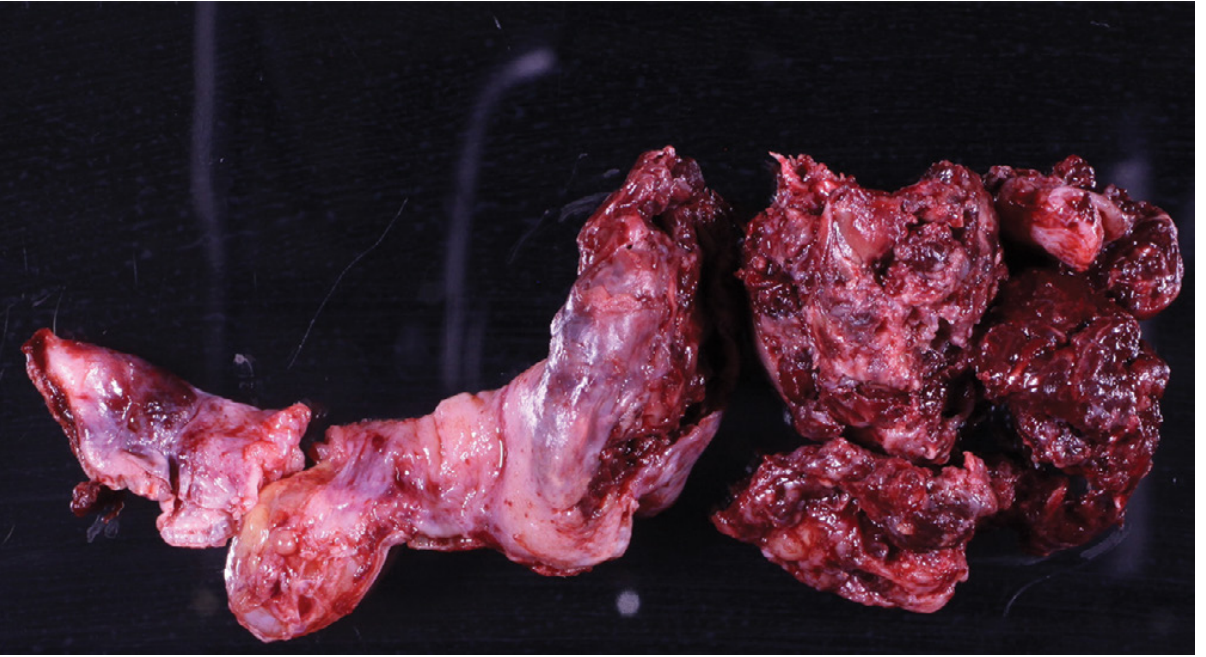
Fig. 9 Ectopic tubal pregnancy - gross pathology. The fallopian tube (left) is distended and has ruptured due to intratubal implantation of the embryo. On the right are the associated blood clot and products of conception expelled at rupture. Tubal rupture causes massive intraperitoneal hemorrhage and is a surgical emergency.
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 22.46
Image 10 - MRI of Ectopic Pregnancy (Coronal T2W)
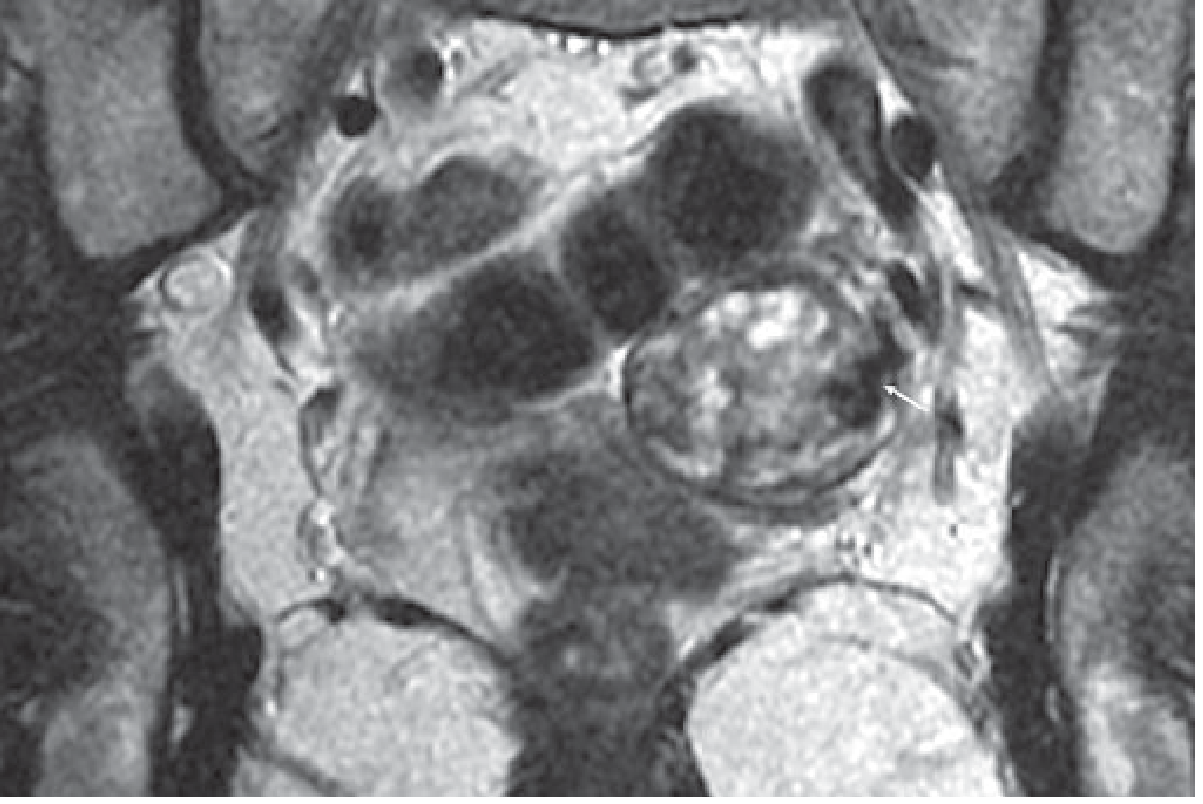
Fig. 10 Ectopic pregnancy on MRI. T2-weighted coronal MRI demonstrates a heterogeneous left adnexal mass with low T2 signal serpiginous structures (white arrow) consistent with flow voids in large vessels of the ectopic gestation. MRI is useful in diagnostically challenging cases where the beta-hCG is not elevated or when other pelvic masses must be excluded.
Source: Grainger & Allison's Diagnostic Radiology, Fig. 35.51
Key Teaching Points
| Feature | Dermoid Cyst | Molar Pregnancy | Tubal Pregnancy |
|---|---|---|---|
| Nature | Mature cystic teratoma (germ cell) | Gestational trophoblastic disease | Ectopic implantation in fallopian tube |
| Imaging modality | US (echogenic nodule/Rokitansky nodule), MRI (T1 bright fat) | Ultrasound (snowstorm pattern), hCG markedly elevated | Transvaginal US (adnexal mass, tubal ring), MRI |
| Key histology | Stratified squamous epithelium + skin appendages (hair, sebaceous glands) | Hydropic villi + trophoblastic hyperplasia | Chorionic villi within fallopian tube wall |
| Clinical risk | Torsion, rupture | Invasive mole (15%), choriocarcinoma (2.5%) | Rupture → hemorrhagic shock, death |
Give more real images and don’t give histological and diagrammatic images
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.