Peptic ulcer
Reading File
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here is the comprehensive coverage of Peptic Ulcer Disease:
Peptic Ulcer Disease (PUD)
Definition
A peptic ulcer is a breach in the mucosal lining of the gastrointestinal tract that extends through the muscularis mucosae, caused by the digestive action of gastric acid and pepsin. Although the name implies pepsin, acid is the decisive factor - peptic ulcers do not occur in its absence, and virtually all can be healed by rendering a patient achlorhydric with proton pump inhibitors (PPIs). - Bailey and Love's Short Practice of Surgery, p. 1178
Epidemiology
- More than 4 million individuals in the United States are treated annually
- Lifetime risk: ~10% in males, ~4% in females
- Worldwide, ~70% of duodenal ulcers and ~50% of gastric ulcers are related to H. pylori colonization
- In many developed countries, NSAIDs have overtaken H. pylori as the leading cause of gastric ulcers, partly due to aging populations on low-dose aspirin
- Duodenal ulcers are more common than gastric ulcers overall
- Robbins & Kumar Basic Pathology, p. 555; Harrison's Principles of Internal Medicine 22E, p. 1345
Sites
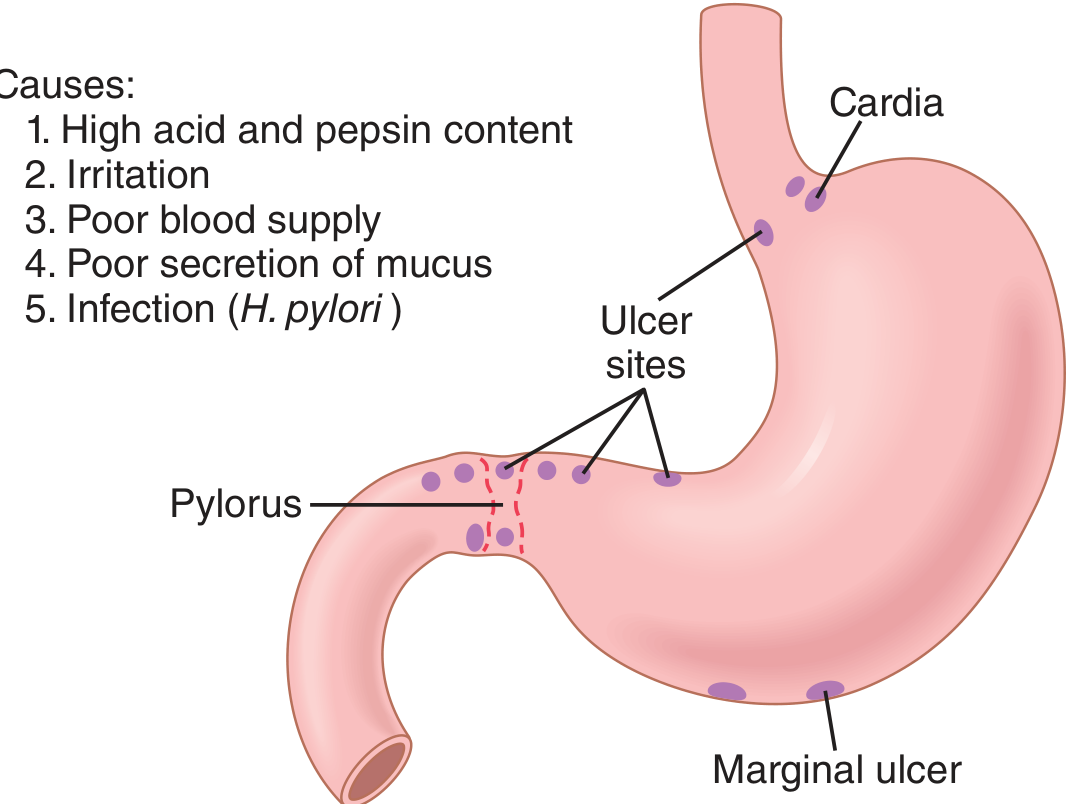
| Site | Notes |
|---|---|
| First part of the duodenum | Most common; ulcers occur within a few centimeters of the pyloric valve, usually anterior wall |
| Gastric antrum / lesser curvature | Interface of body and antrum; always biopsy to exclude malignancy |
| Pyloric channel / prepyloric | Behave like duodenal ulcers; malignancy possible |
| Stomal ulcer | After gastroenterostomy |
| Meckel's diverticulum | Contains ectopic gastric epithelium |
| Lower esophagus | Due to acid reflux (GERD) or ectopic gastric mucosa |
- Guyton and Hall Medical Physiology, p. 825; Bailey and Love, p. 1178; Robbins, p. 555
Pathophysiology
PUD arises from an imbalance between mucosal aggression and defense. - Guyton and Hall, p. 825
Mucosal Defense Mechanisms
- Mucus layer - secreted by surface epithelial cells, mucous neck cells, deep pyloric glands, and Brunner's glands of the duodenum
- Bicarbonate secretion - from pancreas, Brunner's glands, and bile neutralizes luminal acid
- Feedback inhibition - excess duodenal acid triggers:
- Neural reflexes inhibiting gastric secretion and emptying
- Secretin release → stimulates pancreatic bicarbonate secretion
- Mucosal blood flow - maintains cellular integrity and removes back-diffused H⁺
Aggressive Factors
- Hydrochloric acid (from parietal cells)
- Pepsinogen (activated to pepsin by low pH)
- H. pylori virulence factors
- NSAIDs/aspirin (topical injury + COX inhibition reducing prostaglandins)
- Bile salts (back-diffusion in gastric ulcers)
Etiology and Risk Factors
1. Helicobacter pylori (~70% of duodenal, ~50% of gastric ulcers)
- Only 5-10% of infected individuals develop ulcers, so host factors and strain variation matter
- Key evidence: (1) infection is a risk factor; (2) non-NSAID ulcers rarely occur without it; (3) eradication virtually abolishes long-term relapse; (4) experimental infection in gerbils produces gastric ulcers
- Mechanism: H. pylori breaks down the mucosal barrier by secreting urease (generates ammonia), proteases, phospholipases, and vacuolating cytotoxin (VacA); the cagA pathogenicity island strains are particularly virulent
- Harrison's, p. 1345; Robbins, p. 555
2. NSAIDs / Aspirin
- Dual mechanism: direct topical injury (weakly acidic drugs penetrate mucosal cells) + systemic COX-1 inhibition (reduces prostaglandin E₂ and I₂, impairing mucus/bicarbonate secretion and mucosal blood flow)
- In the US, NSAID use is becoming the most common cause of gastric ulcers as H. pylori rates fall
3. Hyperacidity States
- Zollinger-Ellison syndrome (gastrinoma): Multiple ulcers in stomach, duodenum, and even jejunum; massive acid production from unregulated gastrin
- Parietal cell hyperplasia, excessive secretory responses, or loss of inhibitory signals
4. Other Risk Factors
- Cigarette smoking - reduces mucosal blood flow, increases relapse rate
- Corticosteroids - suppress prostaglandin synthesis
- Alcohol-related cirrhosis, COPD, chronic renal failure, hyperparathyroidism (hypercalcemia stimulates gastrin → increased acid secretion)
- Stress ulcers (critically ill patients)
- Robbins & Kumar, p. 555-556; Bailey and Love, p. 1179
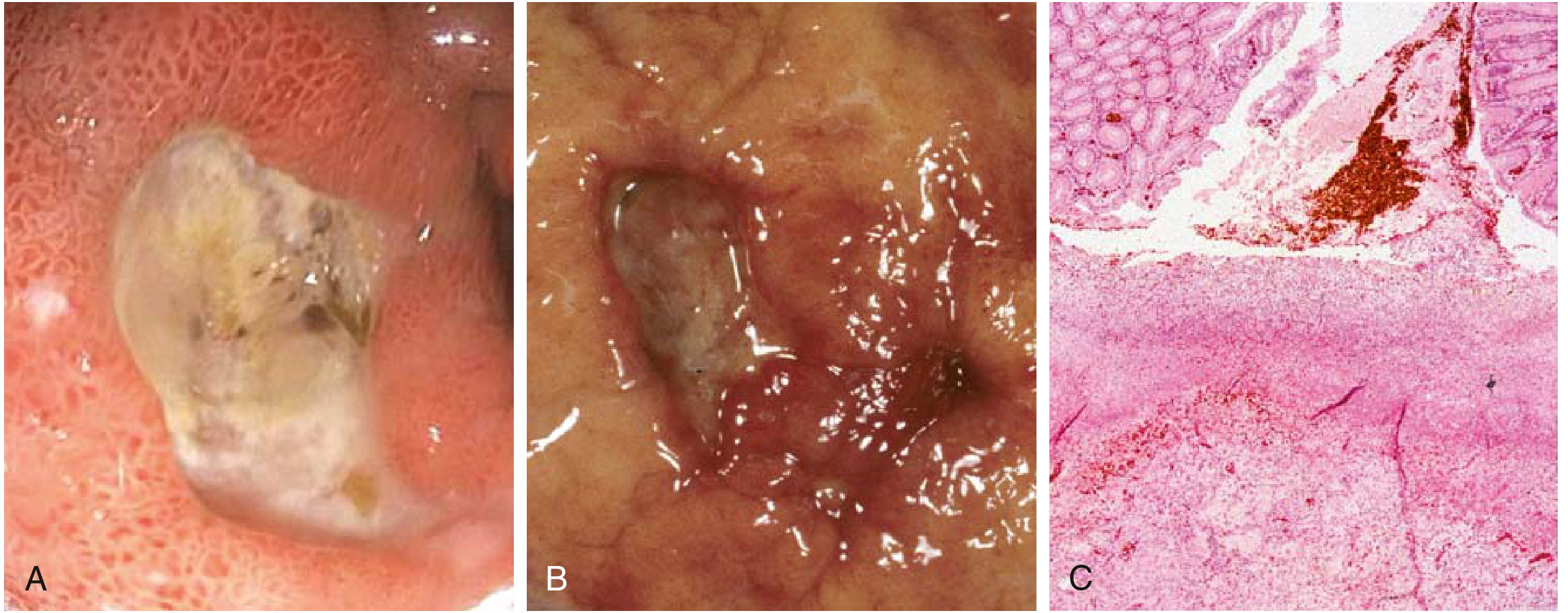
Morphology
The classic peptic ulcer is a round to oval, sharply punched-out defect with clean edges. Margins are indurated and regular. The ulcer base, on histology, is composed of vascular granulation tissue overlaid by degraded blood/necrotic debris. - Robbins & Kumar, p. 556
- Duodenal ulcers: 4x more common than gastric; usually anterior wall of duodenal bulb; anterior = perforate, posterior = bleed (by eroding the gastroduodenal artery)
- Gastric ulcers: Near the body-antrum interface; always biopsy (up to 10 targeted biopsies) to exclude malignancy
- Solitary in >80% of patients
- "Kissing ulcers" - both anterior and posterior duodenal walls involved simultaneously
Clinical Features
- Epigastric pain/burning - the cardinal symptom; occurs 1-3 hours after meals, worse at night
- Pain relieved by food or antacids (classically duodenal ulcer)
- Nausea, vomiting, bloating, belching
- A significant fraction present initially with complications: iron-deficiency anemia, hemorrhage, or perforation
- Pattern of remission and relapse is characteristic (unlike nonulcer dyspepsia, which tends not to remit)
- Robbins, p. 556; Bailey and Love, p. 1178
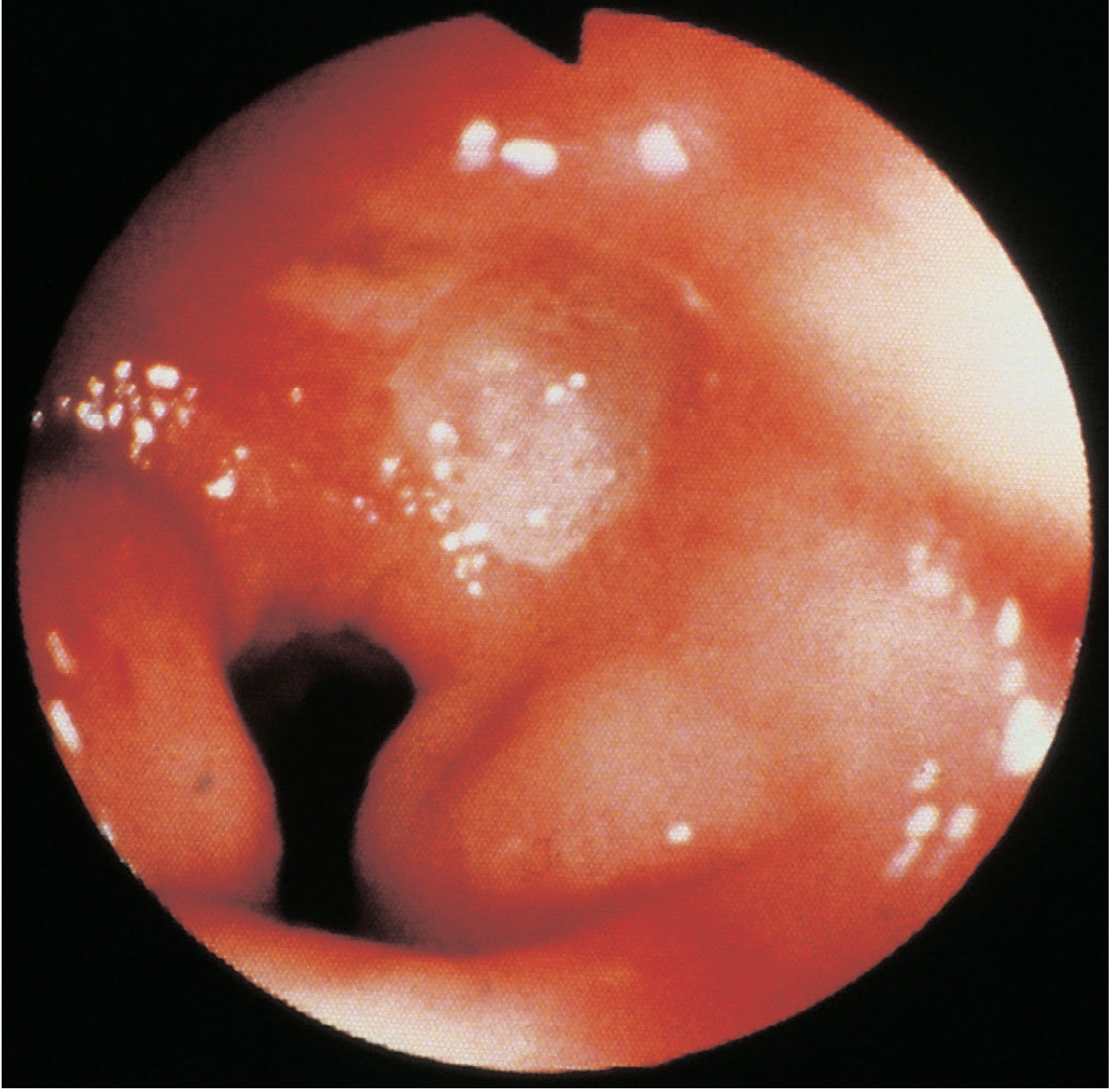
Endoscopic view - Duodenal Ulcer
Diagnosis
| Test | Notes |
|---|---|
| Upper GI endoscopy | Gold standard; most sensitive; biopsies for H. pylori and malignancy |
| Barium meal | Shows "niche" or crater; less sensitive; useful when endoscopy unavailable |
| Urea breath test (UBT) | Best non-invasive test for active H. pylori infection; preferred for test-of-cure |
| Stool antigen test | Good sensitivity/specificity; useful for diagnosis and cure testing |
| Serology (IgG) | Cannot distinguish active from past infection; not useful for test-of-cure |
| Biopsy urease test (CLO test) | Rapid; done at endoscopy |
| Fasting serum gastrin | If Zollinger-Ellison syndrome suspected (ulcers in unusual sites, diarrhea, refractory to treatment) |
- All gastric ulcers must be regarded as potentially malignant until proven otherwise by biopsy and follow-up re-endoscopy to confirm healing. Modern PPIs can heal the ulceration of a gastric cancer without treating the malignancy. - Bailey and Love, p. 1180
Medical Treatment
1. Acid Suppression
- Proton pump inhibitors (PPIs) are the mainstay - omeprazole, lansoprazole, esomeprazole, pantoprazole, rabeprazole
- H₂-receptor antagonists (ranitidine, famotidine) - second-line; less potent
- Antacids - symptomatic relief only
2. H. pylori Eradication
Eradication essentially changes the natural history of PUD - long-term relapse rates drop to near zero after successful eradication. Key factors for success: patient compliance and absence of antibiotic resistance. - Harrison's 22E, p. 1346
Recommended Eradication Regimens (Harrison's 22E, Table 16-2):
| Regimen | Drugs | Duration |
|---|---|---|
| OCM (first-line where clarithromycin resistance <20%) | Omeprazole 20 mg bid + Clarithromycin 500 mg bid + Metronidazole 500 mg bid | 14 days |
| OCA | Omeprazole 20 mg bid + Clarithromycin 500 mg bid + Amoxicillin 1 g bid | 14 days |
| OBTM (Bismuth quadruple) | Omeprazole + Bismuth subsalicylate + Tetracycline 500 mg qid + Metronidazole 500 mg tid | 14 days |
| Concomitant (4-drug) | Omeprazole + Amoxicillin + Clarithromycin + Tinidazole | 14 days |
| OAL (Levofloxacin-based) | Omeprazole + Amoxicillin + Levofloxacin 500 mg bid | 10 days |
- Bismuth quadruple therapy is recommended first-line in most countries; OCA/OCM only where clarithromycin resistance <20%
- Failure of triple therapy in a compliant patient is usually due to antibiotic resistance (especially clarithromycin)
- Test-of-cure with UBT or stool antigen at least 4 weeks after completion
3. NSAID-Associated Ulcers
- Discontinue NSAID if possible
- Start PPI; 4-8 week courses heal most ulcers
- If NSAID cannot be stopped: use lowest effective dose + long-term PPI, or switch to a selective COX-2 inhibitor
- A 2025 Cochrane review (PMID 40337979) confirms PPIs are effective for prevention of NSAID-induced ulcers and dyspepsia
Complications
| Complication | Features | Management |
|---|---|---|
| Hemorrhage (most common) | Hematemesis, melena; posterior DU bleeds into gastroduodenal artery | Endoscopic hemostasis (injection, thermal coagulation, clips); PPI infusion; surgery if rebleeding/failure |
| Perforation | Acute abdomen; free air under diaphragm on erect CXR; anterior DU most common | Emergency surgery (Graham patch repair); conservative (Taylor's method) in selected patients |
| Pyloric stenosis/obstruction | Repeated vomiting, succussion splash, projectile vomiting | Nasogastric aspiration, correction of hypochloraemic alkalosis, endoscopic dilatation or surgery |
| Penetration | Ulcer erodes into adjacent organ (pancreas, liver) | Surgery |
| Malignant transformation | Rare in gastric ulcers; mandatory biopsy | Gastrectomy |
Rockall Score (for upper GI bleed risk stratification):
- Based on: age, pulse, BP, comorbidity, diagnosis, endoscopic stigmata
- Score ≥8: rebleeding ~42%, mortality ~41% - Sleisenger & Fordtran's GI and Liver Disease, Table 20.3
Surgery (Now Rarely Required)
Currently reserved only for:
- Uncontrollable hemorrhage
- Perforation not managed conservatively
- Pyloric obstruction refractory to endoscopic dilatation
- Failure of medical therapy (rare)
There is no indication for elective surgery in uncomplicated ulcer disease in the era of PPIs and H. pylori eradication. - Maingot's Abdominal Operations; Bailey and Love, p. 1178
Historical operations (now rarely performed):
- Truncal vagotomy + pyloroplasty/gastroenterostomy
- Highly selective (proximal gastric) vagotomy
- Partial gastrectomy (Billroth I / Billroth II)
Summary
"No acid, no ulcer" - the old dictum remains valid. But H. pylori eradication has transformed PUD from a lifelong relapsing condition into a curable disease. The goals of management are: eradicate H. pylori, suppress acid, eliminate causative drugs, and confirm healing of all gastric ulcers endoscopically.
Sources: Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine 22E (2025) | Guyton and Hall Medical Physiology | Bailey and Love's Short Practice of Surgery 28e | Sleisenger and Fordtran's GI and Liver Disease
Absorption of protein from guyton
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content directly from Guyton & Hall. Here is the complete, illustrated answer:
Absorption of Protein — Guyton and Hall Textbook of Medical Physiology
Protein absorption is a two-step process: first digestion (breakdown of proteins into absorbable units), then absorption (transport across the intestinal epithelium into the blood).
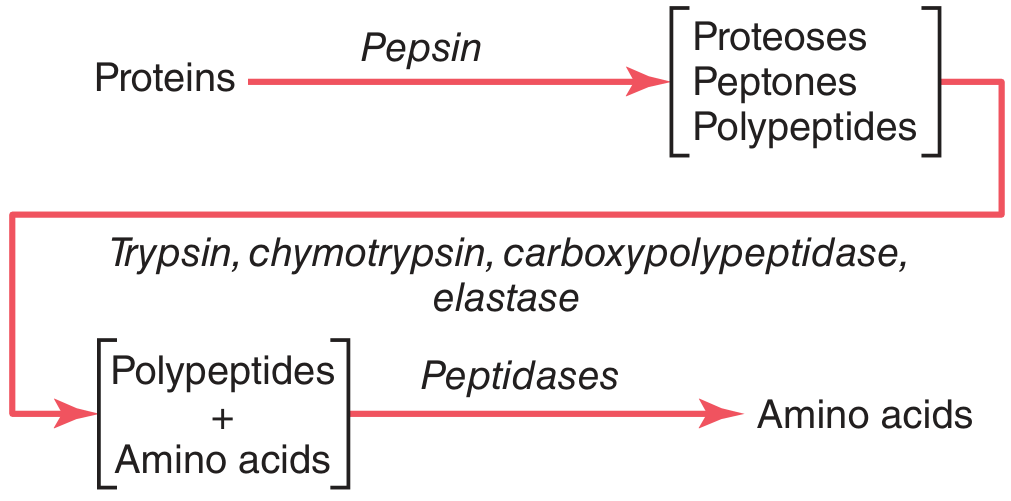
Step 1 — Digestion of Proteins
Stage 1: Stomach — Pepsin (10-20% of total digestion)
Dietary proteins are long chains of amino acids held together by peptide linkages. Digestion begins in the stomach under the action of pepsin, which:
- Is most active at pH 2.0–3.0 and inactive above pH 5.0
- Converts proteins into proteoses, peptones, and a few polypeptides (only 10–20% of total digestion)
- Uniquely digests collagen - an important first step, since collagen holds meat fibers together and must be broken down to allow other enzymes to reach the meat proteins
Stage 2: Small Intestine (Duodenum & Jejunum) — Pancreatic Enzymes (majority of digestion)
On entering the small intestine, the partially digested proteins are attacked by pancreatic proteolytic enzymes:
| Enzyme | Action |
|---|---|
| Trypsin | Splits proteins and polypeptides into smaller polypeptides |
| Chymotrypsin | Splits proteins/polypeptides into smaller polypeptides |
| Carboxypeptidase A & B | Cleaves individual amino acids from the carboxyl end of polypeptides |
| Elastase | Digests elastin fibers that hold meats together |
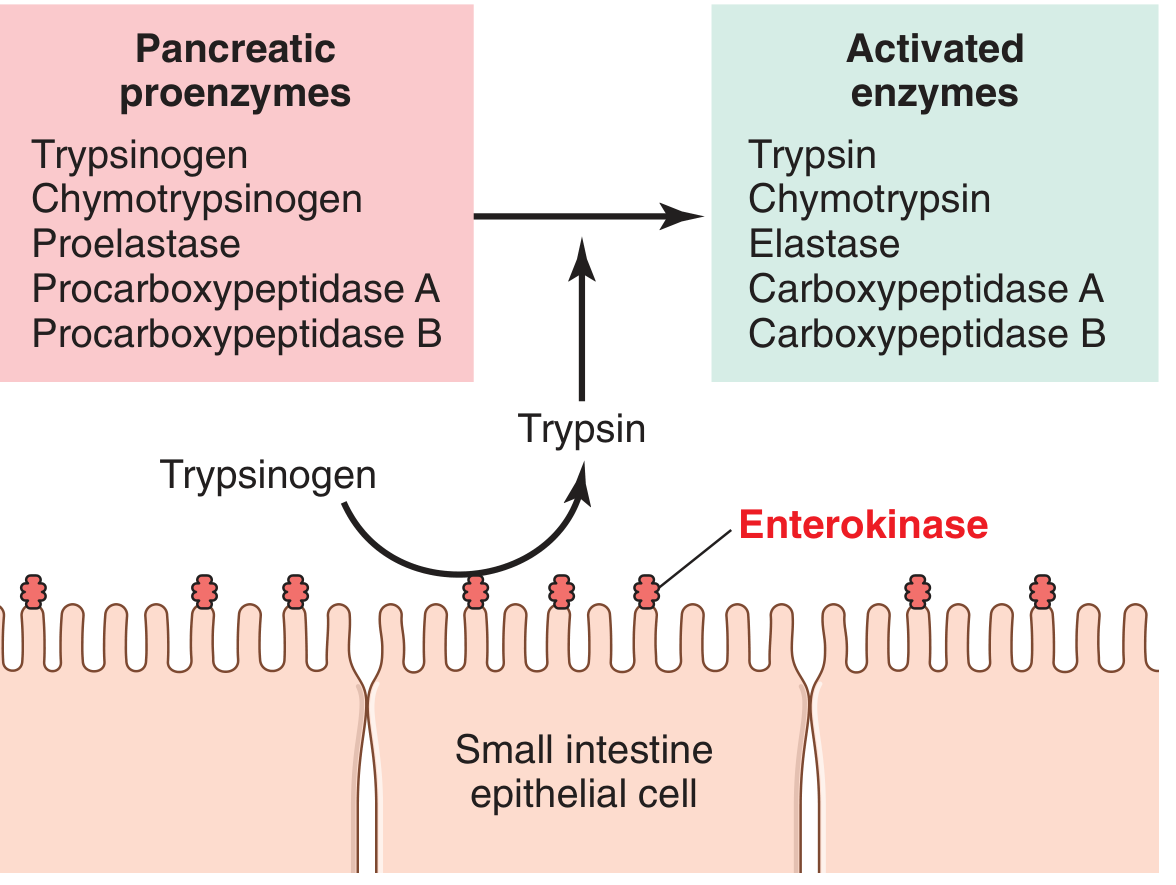
These enzymes are secreted as inactive proenzymes (zymogens):
- Trypsinogen → activated by enterokinase (expressed on the luminal membrane of small intestine epithelial cells)
- Trypsin then activates all the others (chymotrypsinogen, procarboxypeptidases A & B, proelastase) in a cascade
After pancreatic enzymes act, most proteins remain as dipeptides and tripeptides - only small percentages are digested all the way to free amino acids at this stage.
Stage 3: Brush Border — Enterocyte Peptidases (final luminal digestion)
The enterocytes lining the small intestinal villi have a brush border with hundreds of microvilli. Embedded in their membranes are peptidases that complete digestion:
- Aminopolypeptidase and multiple dipeptidases project through the microvillar membrane into the intestinal lumen
- They split remaining larger polypeptides into tripeptides, dipeptides, and some free amino acids
- These are then easily transported across the microvillar membrane into the enterocyte interior
Inside the cytosol of the enterocyte, additional peptidases specific for remaining peptide linkages complete the job - within minutes, virtually all remaining dipeptides and tripeptides are hydrolyzed to single amino acids.
Step 2 — Absorption (Transport Across the Intestinal Epithelium)
Form in which proteins are absorbed
More than 99% of the final protein digestive products absorbed are individual amino acids. Only rare absorption of peptides occurs, and very rare absorption of whole protein molecules. - Guyton and Hall, p. 821
The few whole protein molecules that are absorbed can sometimes trigger allergic or immunological reactions.
Mechanism of Transport — Sodium Co-Transport (Secondary Active Transport)
Most amino acids and peptides are absorbed by the same Na⁺ co-transport mechanism used for glucose:
- Na⁺-K⁺-ATPase on the basolateral membrane actively pumps Na⁺ out of the enterocyte → creates a low intracellular Na⁺ concentration
- On the luminal (brush border) membrane, a specific carrier protein will not transport the amino acid/peptide unless it also binds Na⁺
- Na⁺ moves down its electrochemical gradient into the cell and carries the amino acid or peptide along with it (co-transport)
- Once inside the cell, amino acids exit through the basolateral membrane (by facilitated diffusion or active transport) into the paracellular space → then into the blood
At least 10 different transport proteins for amino acids and peptides exist in the intestinal epithelial cells - this multiplicity is required because of the diverse binding properties of different amino acids and peptides.
A few amino acids do not require Na⁺ co-transport and are instead transported by facilitated diffusion via special membrane transport proteins (similar to fructose absorption).
After Absorption — Blood Amino Acids and Fate
- Normal blood amino acid concentration: 35–65 mg/dL (~2 mg/dL per amino acid on average)
- Amino acids exist in the blood in the ionized state and account for 2–3 mEq/L of anions
Why blood amino acid concentration rises only slightly after a meal:
- Protein digestion and absorption are spread over 2–3 hours → only small quantities absorbed at a time
- After entering the blood, amino acids are taken up by cells (especially the liver) within 5–10 minutes
Therefore, large concentrations of amino acids almost never accumulate in the blood. Nevertheless, the turnover is so rapid that many grams of protein can be transported per hour in the form of amino acids.
Renal handling:
Amino acids filtered by the glomerulus are reabsorbed by secondary active transport in the proximal tubule. When plasma concentration exceeds the tubular transport maximum, excess amino acids are lost in the urine.
Summary Flow
Dietary Protein
↓ [Stomach: Pepsin, pH 2-3]
Proteoses, Peptones, Polypeptides (10-20%)
↓ [Small intestine: Trypsin, Chymotrypsin, Carboxypeptidases, Elastase]
↓ [Activated by: Enterokinase → Trypsin → all others]
Dipeptides + Tripeptides + some Free Amino Acids
↓ [Brush border peptidases: Aminopolypeptidase, Dipeptidases]
Dipeptides, Tripeptides, Free Amino Acids
↓ [Absorbed across microvillar membrane by Na⁺ co-transport]
Inside Enterocyte → Cytosolic peptidases complete hydrolysis
↓
Free Amino Acids
↓ [Exit via basolateral membrane → Portal blood]
>99% absorbed as free amino acids
- Guyton and Hall Textbook of Medical Physiology, Chapter 66 (Digestion and Absorption in the GI Tract) and Chapter 70 (Protein Metabolism)
Again
Here is the full topic again, directly from Guyton & Hall:
Absorption of Protein — Guyton and Hall Textbook of Medical Physiology
Protein absorption is a two-step process: digestion (breakdown into absorbable units) followed by transport across the intestinal epithelium into the blood.
Step 1 — Digestion of Proteins
Stage 1: Stomach — Pepsin (10–20% of total digestion)
Dietary proteins are long chains of amino acids held by peptide linkages. Digestion begins in the stomach:
- Pepsin is active at pH 2.0–3.0 and inactive above pH 5.0
- Gastric HCl (secreted by parietal cells at pH ~0.8) acidifies the contents to pH ~2.0–3.0, creating ideal conditions for pepsin
- Pepsin converts proteins into proteoses, peptones, and a few polypeptides — only 10–20% of total protein digestion
- A key unique role of pepsin: it digests collagen, which holds meat fibers together. Without pepsin, other digestive enzymes cannot penetrate meats adequately → poor digestion
Stage 2: Small Intestine — Pancreatic Proteolytic Enzymes (majority of digestion)
On entering the duodenum, partially digested proteins are attacked by pancreatic enzymes:
| Enzyme | Action |
|---|---|
| Trypsin | Splits proteins/polypeptides into smaller polypeptides |
| Chymotrypsin | Splits proteins/polypeptides into smaller polypeptides |
| Carboxypeptidase A & B | Cleaves individual amino acids from the carboxyl end |
| Elastase | Digests elastin fibers that hold meats together |
Proenzyme activation cascade:
All pancreatic proteolytic enzymes are secreted as inactive zymogens (proenzymes):
- Trypsinogen → Trypsin via enterokinase (a proteolytic enzyme expressed on the luminal membrane of small intestine epithelial cells)
- Trypsin then activates all the others: chymotrypsinogen → chymotrypsin; proelastase → elastase; procarboxypeptidase A & B → carboxypeptidase A & B
After pancreatic enzyme action, most proteins remain as dipeptides and tripeptides — only small percentages are fully digested to free amino acids in the lumen.
Stage 3: Brush Border Peptidases of Enterocytes (final digestion)
Enterocytes lining the small intestinal villi have a brush border with hundreds of microvilli. Peptidases project through the microvillar membrane into the intestinal lumen:
- Aminopolypeptidase and multiple dipeptidases split remaining polypeptides into tripeptides, dipeptides, and free amino acids
- These small units are then transported into the enterocyte
- Inside the cytosol, further peptidases complete hydrolysis — within minutes, virtually all dipeptides and tripeptides are broken down to single amino acids
Step 2 — Absorption (Transport Across the Intestinal Epithelium)
Form in which proteins are absorbed
More than 99% of the final absorbed products are individual amino acids. Only rarely are peptides absorbed, and whole protein molecules are absorbed in very small amounts (sufficient to trigger allergic/immunological reactions in some individuals).
Mechanism — Sodium Co-Transport (Secondary Active Transport)
Most dipeptides, tripeptides, and amino acids cross the luminal (brush border) membrane by the same Na⁺ co-transport mechanism as glucose:
- Na⁺-K⁺-ATPase on the basolateral membrane pumps Na⁺ out of the enterocyte → creates low intracellular Na⁺
- On the luminal membrane, a carrier protein requires Na⁺ binding before it will transport the amino acid/peptide
- Na⁺ moves down its electrochemical gradient into the cell, pulling the amino acid or peptide with it — this is secondary active transport (co-transport)
- The energy ultimately comes from Na⁺-K⁺-ATPase on the basolateral side
- At least 10 different transport proteins exist for amino acids and peptides in the intestinal epithelial cells, required because of the diverse binding properties of different amino acids and peptides
- A few amino acids do not need Na⁺ co-transport; instead they use facilitated diffusion via special membrane carriers (similar to fructose absorption)
Exit from Enterocyte → Blood
After crossing the luminal membrane, amino acids pass through the basolateral membrane into the paracellular space and then into the portal blood, transported to the liver first.
After Absorption — Blood Amino Acids
- Normal blood amino acid concentration: 35–65 mg/dL (~2 mg/dL per amino acid on average)
- Amino acids exist in the ionized state in blood and account for 2–3 mEq/L of anions
Why blood amino acid level rises only slightly after a meal:
- Protein digestion and absorption are spread over 2–3 hours → only small quantities absorbed at a time
- After entering the blood, amino acids are rapidly taken up by cells (especially the liver) within 5–10 minutes
Despite this, the turnover is so rapid that many grams of protein can be transported per hour across the body in the form of amino acids.
Renal handling:
Amino acids filtered by the glomerulus are reabsorbed by secondary active transport in the proximal tubule. When plasma concentration exceeds the transport maximum (Tm), excess amino acids spill into the urine.
Summary Flow
Dietary Protein
↓ Stomach: Pepsin (pH 2–3) → 10–20% digestion
Proteoses, Peptones, Polypeptides
↓ Duodenum/Jejunum: Trypsin, Chymotrypsin,
Carboxypeptidases, Elastase
(Trypsinogen activated by Enterokinase → Trypsin
activates all other proenzymes)
Dipeptides + Tripeptides + some Free Amino Acids
↓ Brush border: Aminopolypeptidase + Dipeptidases
Dipeptides, Tripeptides, Free Amino Acids
↓ Absorbed via Na⁺ co-transport across luminal membrane
Inside Enterocyte → Cytosolic peptidases hydrolyze all residual di/tripeptides
↓
Free Amino Acids → exit basolateral membrane → Portal blood
>99% absorbed as free amino acids
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 66 (Digestion and Absorption) & Chapter 70 (Protein Metabolism)
This is a shared conversation. Sign in to Orris to start your own chat.