Ferguson reflex
Reading File
Finding Sources
Searching the Web
Ferguson reflex physiology cervix oxytocin uterine contractions
Reading File
Reading File
Reading File
Ferguson Reflex
The Ferguson reflex is a positive-feedback neuroendocrine mechanism that drives uterine contractions to completion during labor. It was described by J.K.W. Ferguson in 1941.
Mechanism (Step by Step)
- Stimulus: As labor progresses, the presenting fetal part (usually the head) presses against and distends the cervix.
- Afferent arc: Stretch receptors in the cervix and upper vagina send neural impulses via afferent sensory fibers through the spinal cord to the hypothalamus.
- Oxytocin (OT) release: The hypothalamus signals the posterior pituitary (neurohypophysis) to release oxytocin in pulsatile bursts. The frequency of these bursts increases as labor progresses.
- Uterine response: Oxytocin binds to Gαq-coupled oxytocin receptors (OTRs) on myometrial cells, triggering the phospholipase C cascade. IP3 releases Ca²+ from internal stores, raising intracellular [Ca²+], which activates calmodulin and myosin light-chain kinase, producing smooth muscle contraction and increased intrauterine pressure.
- Prostaglandin amplification: Oxytocin also binds to receptors on decidual cells, stimulating PGF2α production, which further intensifies contractions.
- Positive feedback loop: Stronger contractions stretch the cervix further, releasing more oxytocin, producing yet stronger contractions - the cycle continues until delivery.
- Medical Physiology (Boron & Boulpaep), pp. 1671-1672
Role of Oxytocin Receptors
Estrogen progressively upregulates OTRs in the myometrium and decidua throughout pregnancy:
- The uterus is insensitive to OT until ~20 weeks' gestation
- OTR numbers rise 80-fold above baseline by ~36 weeks
- During early labor, they rise further to 200-fold above baseline
This receptor upregulation explains why the uterus becomes increasingly responsive to oxytocin as term approaches, even when plasma OT levels remain relatively stable.
- Medical Physiology, p. 1671
Stages of Labor and OT Relevance
| Stage | Role of Ferguson Reflex |
|---|---|
| Stage 1 (early/active labor) | Cervical dilation progressively activates the reflex; OT bursts increase in frequency |
| Stage 2 (expulsive stage) | OT plays a synergistic role in fetal expulsion; also drives the urge to bear down ("pushing urge") |
| Stage 3 (placental delivery) | OT-induced uterine contractions constrict uterine blood vessels at the placental site, promoting hemostasis |
Maternal plasma OT returns to prepartum levels approximately 60 minutes after delivery.
Clinical Relevance
1. Regional anesthesia (epidurals)
Intense epidural analgesia/anesthesia can abolish the urge to bear down during the second stage by blocking the afferent limb of the Ferguson reflex. This can prolong the second stage of labor. Dilute local anesthetic-opioid mixtures (e.g., bupivacaine ≤0.125% + fentanyl ≤5 mcg/mL) are preferred because they preserve motor function and allow effective pushing.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1589
2. Exogenous oxytocin (Pitocin)
Synthetic oxytocin mimics the Ferguson reflex and is used to induce or augment labor (doses 0.5-8 mU/min IV). Overdose risks uterine hyperstimulation and fetal distress.
3. Intravenous fluid loading
Pre-block fluid loading in euvolemic patients has been shown to reduce endogenous oxytocin secretion from the pituitary and transiently decrease uterine activity.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1589
4. Species note
In some animal species (e.g., rabbits), stimulation of the cervix via the Ferguson reflex can also trigger reflex ovulation. This cross-species effect is not seen in humans.
- Berek & Novak's Gynecology
Summary
The Ferguson reflex is a positive-feedback loop: cervical stretch → posterior pituitary oxytocin release → stronger myometrial contractions → more cervical stretch. It is the principal mechanism sustaining and amplifying uterine contractions during active labor, complemented by a parallel PGF2α positive-feedback loop. Epidural anesthesia, if dense enough, can interrupt its afferent arc and impair the expulsive urge in second-stage labor.
Dysphagia and Achalesia cardia
Finding Sources
Searching the Web
achalasia cardia dysphagia pathophysiology diagnosis treatment 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive, textbook-sourced overview of both topics.
DYSPHAGIA
Definition
Dysphagia (Greek: dys = difficulty + phagia = to eat) is the sensation that food is hindered in its passage from the mouth to the stomach. Patients describe food "sticking," "hanging up," or "not going down right." It always indicates some malfunction in the oropharynx or esophagus.
- Sleisenger & Fordtran's GI and Liver Disease, p. 189
Pathophysiology
Normal swallowing transports solids and liquids from mouth to stomach within ~10 seconds via orderly oropharyngeal and esophageal peristaltic contractions. Dysphagia arises from:
- Neuromuscular failure - loss of strength or coordination of swallowing muscles
- Mechanical obstruction - fixed narrowing of the esophageal lumen
- Sensory/perceptual abnormality - aberrant visceral perception even after the bolus has cleared
Classification
1. Oropharyngeal (Transfer) Dysphagia
- Inability to initiate a swallow; bolus does not leave the oropharynx
- Coughing, choking, nasal regurgitation, drooling
- Symptoms occur immediately or within 1 second of swallowing
- Associated features: dysarthria, nasal speech, aspiration pneumonia
Causes:
| Category | Examples |
|---|---|
| Neuromuscular | Stroke, Parkinson's, ALS, multiple sclerosis, myasthenia gravis, polymyositis |
| Structural | Zenker's diverticulum, carcinoma, osteophytes, proximal esophageal web, thyromegaly |
| Other | Poor dentition, salivary dysfunction, post-radiation |
2. Esophageal Dysphagia
- Symptoms localized to lower sternum or epigastrium
- Can often be partially relieved by repeated swallowing, raising arms overhead, Valsalva maneuver
Key diagnostic questions:
- What type of food causes symptoms (solids only vs. solids + liquids)?
- Is the dysphagia intermittent or progressive?
- Does the patient have heartburn?
| Pattern | Likely Cause |
|---|---|
| Solids only, progressive | Mechanical obstruction (stricture, cancer) |
| Solids + liquids from onset | Motility disorder (achalasia, DES) |
| Intermittent, solids only | Esophageal ring (Schatzki) |
| Progressive + heartburn | Peptic stricture from GERD |
- Sleisenger & Fordtran's GI and Liver Disease, p. 189-190
ACHALASIA CARDIA
Definition
Achalasia is a primary esophageal motility disorder characterized by:
- Impaired LES relaxation with swallowing
- Aperistalsis of the smooth-muscle esophagus
Pathophysiology
The core defect is loss of inhibitory ganglion cells in the myenteric (Auerbach) plexus of the smooth muscle esophagus and LES.
Neurochemical basis:
- Inhibitory neurons (using nitric oxide [NO] and vasoactive intestinal peptide [VIP]) are selectively destroyed
- These neurons normally mediate: (1) deglutitive LES relaxation, and (2) sequential propagation of peristalsis
- Their loss causes impaired LES relaxation and aperistalsis simultaneously
- Excitatory cholinergic neurons are relatively preserved early, leading to paradoxically elevated LES resting tone
Molecular mechanism of LES pressure:
- Normally, CCK stimulates inhibitory neurons → reduces LES pressure
- In achalasia, CCK paradoxically increases LES pressure (because inhibitory neurons are absent, only excitatory pathway remains)
Etiology of ganglion cell degeneration (idiopathic):
- Likely autoimmune in genetically susceptible individuals (specific HLA alleles)
- Myenteric plexus infiltrate is predominantly cytotoxic T cells
- Suspected trigger: chronic latent HSV-1 infection
- Sleisenger & Fordtran's GI and Liver Disease, p. 729
Chicago Classification (HRM Subtypes)
| Type | Manometric Pattern | Features |
|---|---|---|
| Type I (Classic) | Absent peristalsis, minimal pressurization | End-stage, dilated esophagus |
| Type II (with compression) | Pan-esophageal pressurization | Early disease; best treatment response |
| Type III (Spastic) | Premature/spastic esophageal contractions | Unique pathogenesis; chest pain prominent |
Types I and II form a continuum (II → I as disease progresses). Type III is distinct.
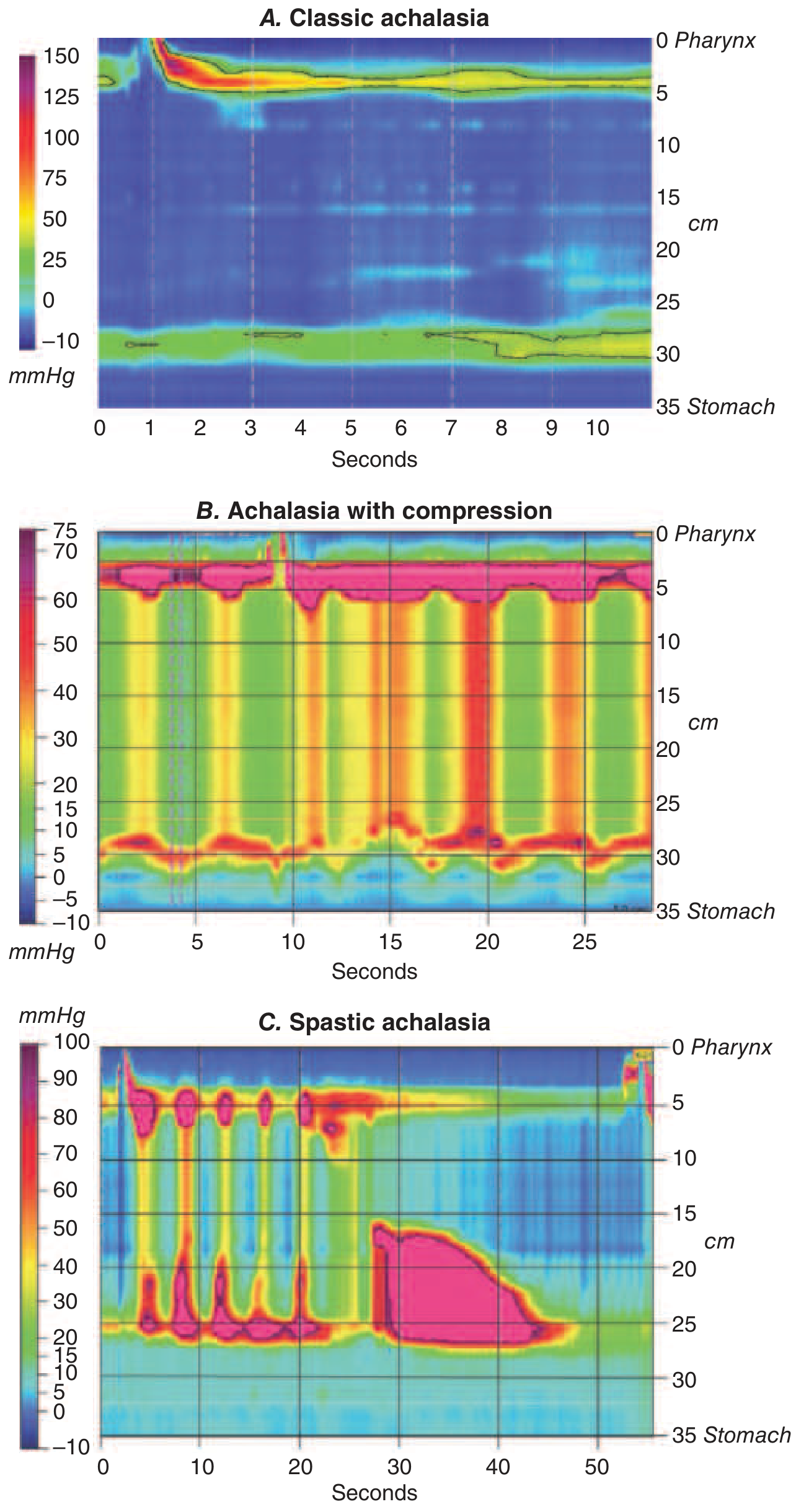
High-resolution manometry plots of the three achalasia subtypes. Harrison's Principles of Internal Medicine 22E (2025)
Clinical Features
- Dysphagia - all patients; both solids AND liquids (hallmark that distinguishes motility disorder from mechanical obstruction)
- Onset is gradual, often present for years before diagnosis
- Regurgitation - nonbilious, nonacid, mixed with saliva; food from hours or days earlier
- Chest pain - in ~2/3 of patients early in course; squeezing/pressure-like, radiating to neck, jaw, arms; does not reliably improve with treatment
- Weight loss - in long-standing disease
- Heartburn - paradoxically reported by many (caused by bacterial fermentation of retained food, NOT true acid reflux)
- Pulmonary complications - aspiration pneumonia, bronchitis, lung abscess in up to 10% of advanced cases
Investigations
1. Barium Swallow (Esophagogram)
Classic findings:
- Dilated esophagus with absent peristalsis
- Air-fluid level
- Smooth, symmetric tapering at the LES - the "bird's beak" sign
- Long-standing disease may show sigmoid deformity
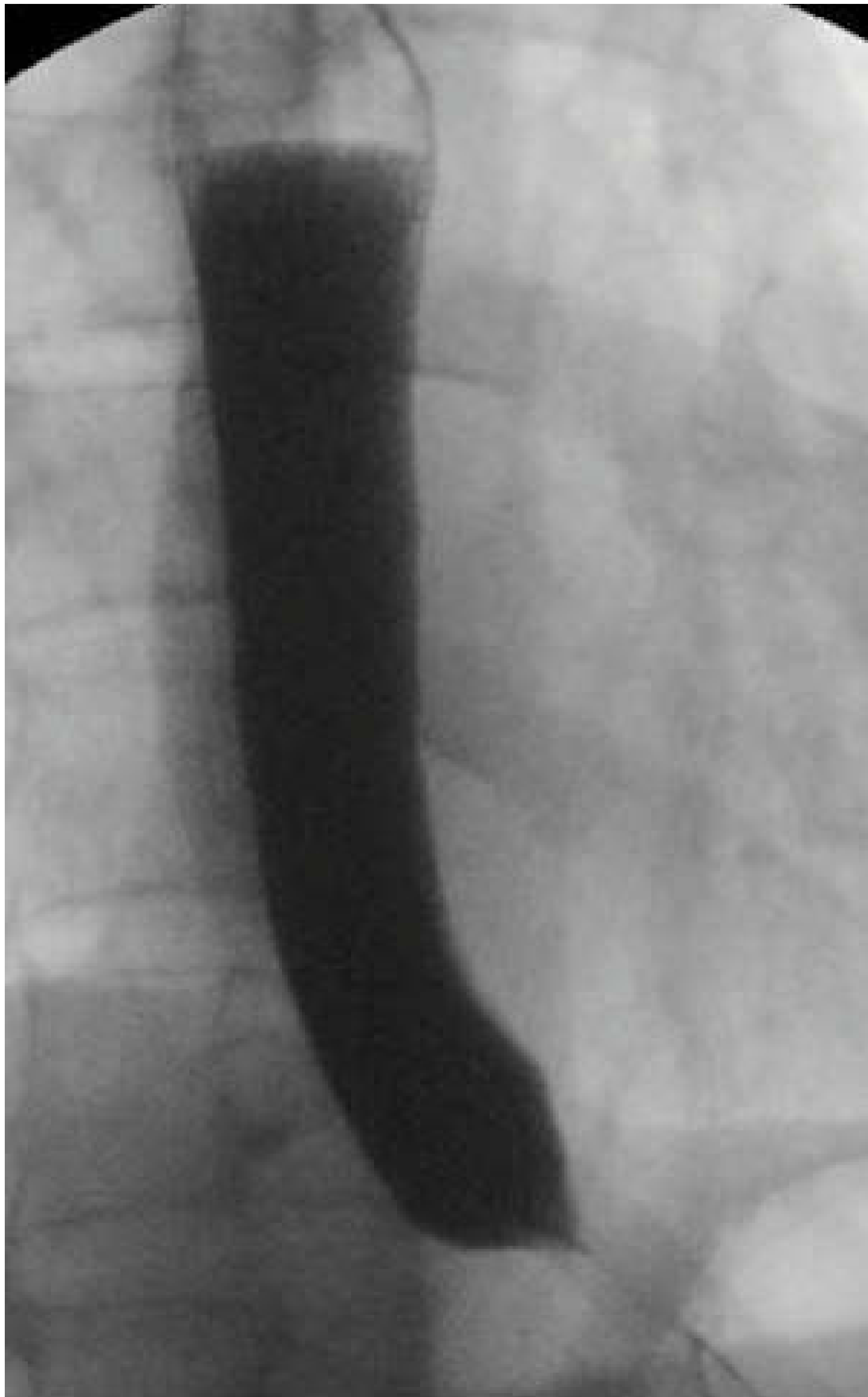
Classic bird's beak appearance on barium swallow in achalasia - Scott-Brown's Otorhinolaryngology
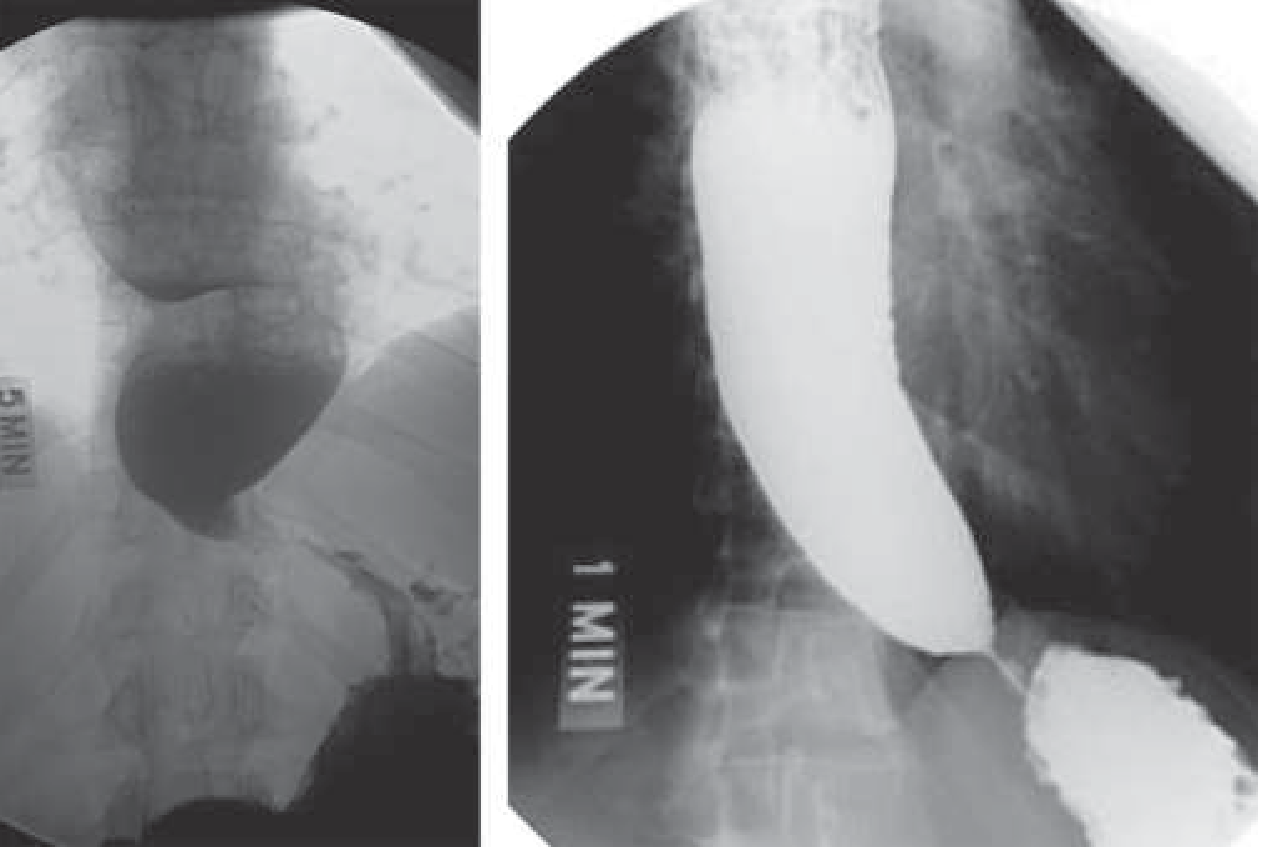
Barium esophagogram showing esophageal dilatation and sigmoid deformity in advanced achalasia - Harrison's Principles 22E
2. High-Resolution Manometry (HRM) - Gold Standard
- Diagnostic criteria: impaired LES relaxation + absent peristalsis
- Most sensitive test - identifies early disease before dilatation
- Subtyping (I, II, III) has critical treatment implications
3. Upper Endoscopy (EGD)
- Mandatory to exclude pseudoachalasia (cancer at gastric cardia/distal esophagus mimicking achalasia)
- Findings: tight gastroesophageal junction, dilated esophagus, food retention
- Early achalasia may show completely normal endoscopy
Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Pseudoachalasia | Rapid onset (<1 year), advanced age, marked weight loss; due to tumor infiltration of GEJ |
| Chagas disease | Endemic in South America; Trypanosoma cruzi destroys autonomic ganglion cells body-wide |
| DES (Diffuse Esophageal Spasm) | Peristalsis present but premature; chest pain dominant |
| Opioid-induced esophageal dysmotility | History of chronic opioid use |
| GERD stricture | History of heartburn; mechanical not motility-based |
Pseudoachalasia accounts for ~5% of suspected achalasia cases. CT scan or EUS is needed when clinical suspicion is high and endoscopy is nondiagnostic.
Treatment
The underlying neuropathology is irreversible, so treatment focuses on reducing LES pressure to allow gravity-assisted esophageal emptying.
Pharmacologic (temporizing only - not durable)
| Drug | Mechanism | Notes |
|---|---|---|
| Sublingual nifedipine (30-40 mg/day before meals) | Ca²+ channel blocker → smooth muscle relaxation | Limited efficacy; side effects: flushing, dizziness, edema |
| Isosorbide dinitrate / nitroglycerin | Nitrate → NO → LES relaxation | Headache common; short duration |
| Sildenafil | PDE-5 inhibitor → ↑ cGMP → LES relaxation | Effective but costly; effect lasts <1 hour |
| Botulinum toxin (intrasphincteric) | Blocks presynaptic ACh release | 66% response at 6 months; not durable; reserved for elderly/frail patients |
Durable Therapies
| Treatment | Efficacy | Notes |
|---|---|---|
| Pneumatic dilation | 60-90% | Rigiflex balloon inflated to 3.0-4.0 cm across LES; 0.5-5% perforation risk; preferred initial therapy for Type II |
| Laparoscopic Heller Myotomy | 62-90% | Surgical division of LES circular muscle; combined with partial fundoplication to prevent reflux; ~90% efficacy at 5 years |
| POEM (Peroral Endoscopic Myotomy) | >80% | Endoscopic submucosal tunnel → electrocautery myotomy; equivalent to Heller myotomy in RCTs; GERD common post-POEM but manageable |
Treatment choice by subtype:
- Type II: Pneumatic dilation preferred (100% efficacy in European RCT)
- Type III (spastic): Laparoscopic myotomy superior to dilation (86% vs. 40%)
- Type I: Either pneumatic dilation or Heller myotomy (~90% for both)
Refractory/end-stage disease: Esophageal resection with gastric pull-up or colonic interposition.
Complications of Untreated Achalasia
- Stasis esophagitis - from retained food
- Esophageal squamous cell carcinoma - after years of progressive dilatation; requires endoscopic surveillance
- Aspiration pneumonia / lung abscess - up to 10% of advanced cases
- Malnutrition and weight loss
- Harrison's Principles of Internal Medicine 22E (2025), p. 2551
- Sleisenger & Fordtran's GI and Liver Disease, p. 729-738
- Scott-Brown's Otorhinolaryngology, p. 883-884
This is a shared conversation. Sign in to Orris to start your own chat.