Explain brain and its parts . What is stroke. Why does it happens Parts of brain and stroke Treatment and diagnosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"stroke" AND "brain" AND "treatment"
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile a comprehensive, well-structured answer.
The Brain and Stroke - A Complete Overview
PART 1: THE BRAIN AND ITS PARTS
The brain is the most complex organ in the body. It sits within the skull, protected by three membranes (meninges) and bathed in cerebrospinal fluid. Without the cerebral cortex, a person would be blind, deaf, mute, and unable to initiate voluntary movement.
The brain has three major divisions: the forebrain (cerebrum + diencephalon), the brainstem, and the cerebellum.
The Cerebrum
The cerebrum is the largest part and is divided into two hemispheres (left and right), each covered by the cerebral cortex - a thin sheet of neurons. The surface is folded into ridges called gyri and grooves called sulci, which dramatically expand the surface area (about 1100 cm²) to fit within the skull.
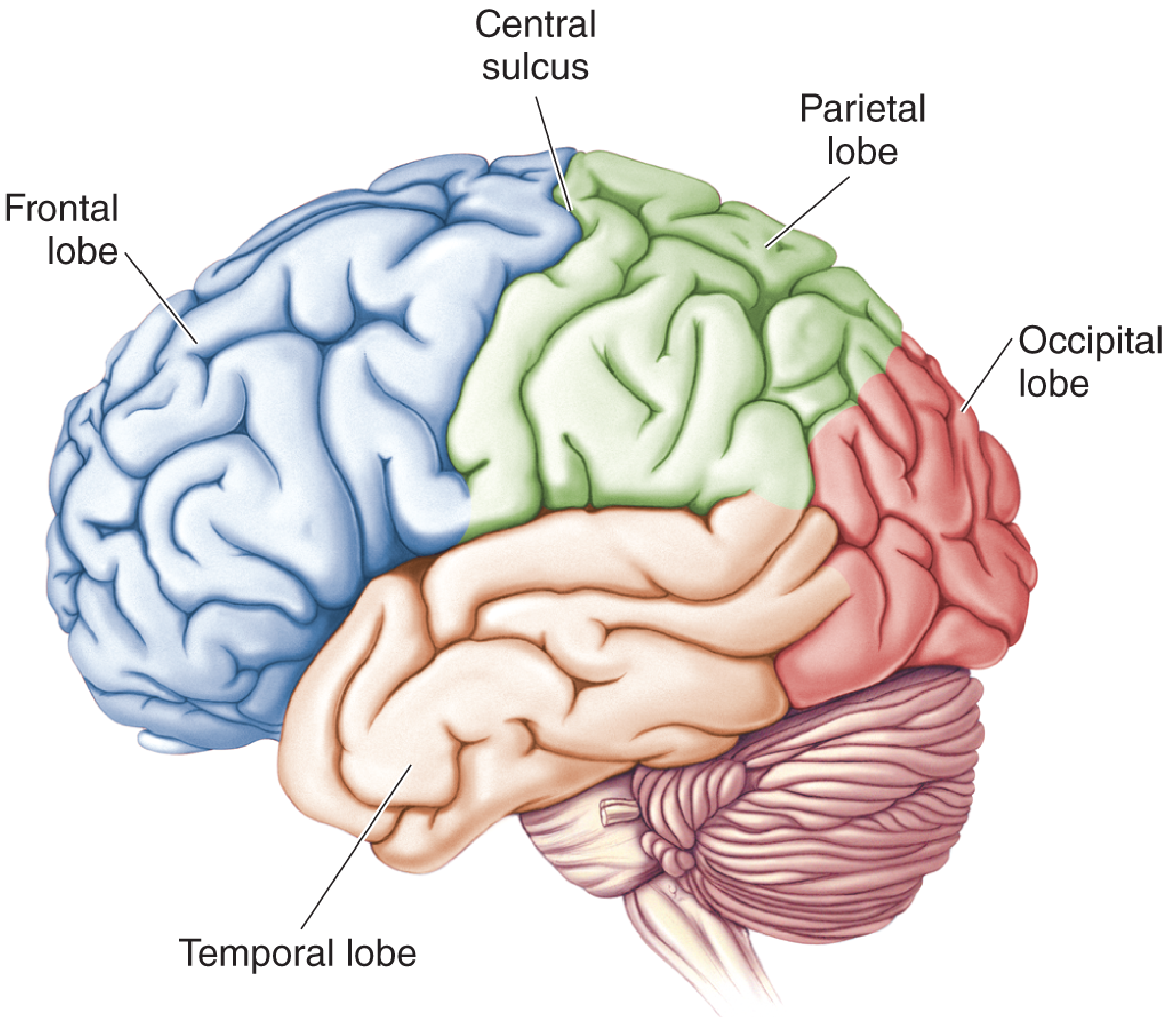
The cerebrum is divided into 4 lobes, each named after the skull bone overlying it:
| Lobe | Location | Main Functions |
|---|---|---|
| Frontal lobe | Front of brain, anterior to central sulcus | Voluntary movement, planning, reasoning, personality, speech (Broca's area) |
| Parietal lobe | Behind central sulcus, under parietal bone | Somatic sensation (touch, pain, temperature, proprioception), spatial awareness |
| Temporal lobe | Below lateral (Sylvian) fissure, under temporal bone | Hearing, memory, language comprehension (Wernicke's area) |
| Occipital lobe | Rear of cerebrum, under occipital bone | Vision and visual processing |
A buried piece of cortex called the insula lies under the lateral fissure, separating temporal and frontal lobes. It is involved in taste, pain perception, and autonomic regulation.
- Neuroscience: Exploring the Brain, 5th Ed., p. 632-662
Brainstem
The brainstem connects the cerebrum to the spinal cord and consists of three parts:
- Midbrain - controls eye movements, pupil reflexes, relays auditory/visual signals
- Pons - involved in breathing regulation, sleep, facial movements, relaying signals between cortex and cerebellum
- Medulla oblongata - controls vital automatic functions: breathing, heart rate, blood pressure, swallowing
Cerebellum
Located at the back/bottom of the brain. It coordinates movement, balance, and fine motor control. It does not initiate movement but fine-tunes it.
Diencephalon
Located deep in the brain, includes:
- Thalamus - relay station for almost all sensory information going to the cortex
- Hypothalamus - controls hormones, body temperature, hunger, thirst, sleep-wake cycles
Limbic System
A group of structures including the hippocampus (memory formation) and amygdala (emotional responses, fear). Lies on the inner border of the cerebral cortex.
PART 2: WHAT IS STROKE?
Stroke (also called cerebrovascular accident, CVA, or historically "apoplexy") is defined as a relatively sudden occurrence of a focal neurologic deficit caused by a vascular event in the brain.
"Among all the neurologic diseases of adult life, stroke ranks first in frequency and importance."
- Adams and Victor's Principles of Neurology, 12th Ed.
The hallmark features are:
- Abrupt onset - typically seconds to minutes
- Focal neurologic deficit - symptoms localized to a specific brain region
PART 3: WHY DOES STROKE HAPPEN? (Causes)
Strokes are broadly divided into two major categories:
1. Ischemic Stroke (~85% of cases)
Caused by occlusion (blockage) of a cerebral blood vessel, leading to brain infarction (tissue death from lack of oxygen).
Sub-types:
- Embolic stroke: A clot (embolus) forms elsewhere (usually the heart or large arteries) and travels to block a brain artery. Onset is typically sudden, deficit peaks almost immediately.
- Thrombotic stroke: A clot forms directly within a brain artery (usually at an atherosclerotic plaque). Evolves more slowly over minutes to hours, sometimes in a "saltatory" (step-by-step) fashion.
- Small vessel (lacunar) stroke: Occlusion of tiny penetrating arteries deep in the brain - often from chronic hypertension.
2. Hemorrhagic Stroke (~15% of cases)
Caused by rupture of a blood vessel with bleeding into or around the brain.
Sub-types:
- Intracerebral hemorrhage (ICH): Bleeding within brain tissue - most often from chronic hypertension, coagulopathies (bleeding disorders or anticoagulants), vascular malformations (arteriovenous malformations - AVMs).
- Subarachnoid hemorrhage (SAH): Bleeding into the space surrounding the brain (subarachnoid space) - most commonly from rupture of a saccular (berry) aneurysm of the Circle of Willis. Onset is almost instantaneous ("thunderclap headache").
Key Risk Factors / Causes Summary:
-
Atherosclerotic thrombosis
-
Cardiac embolism (atrial fibrillation, valvular disease, recent MI)
-
Hypertension (both ischemic and hemorrhagic)
-
Ruptured aneurysm or AVM
-
Arteritis (vasculitis, autoimmune, infectious)
-
Hematologic disorders (polycythemia, sickle cell disease, coagulopathies)
-
Trauma and arterial dissection (carotid or vertebral artery)
-
Venous thrombosis
-
Adams and Victor's Principles of Neurology, 12th Ed., Table 33-1
Transient Ischemic Attack (TIA)
A focal stroke syndrome that reverses itself completely within minutes to ~1 hour. Considered a serious warning sign - it indicates high risk of a full stroke.
PART 4: PARTS OF BRAIN AND STROKE - WHAT SYMPTOMS OCCUR WHERE?
The location of the stroke determines the symptoms. This is because different brain regions have specific functions:
| Brain Region Affected | Typical Symptoms |
|---|---|
| Frontal lobe | Weakness/paralysis on opposite side of body (hemiplegia), loss of speech (Broca's aphasia - can't speak), personality changes |
| Parietal lobe | Sensory loss (numbness, tingling on opposite side), inability to recognize objects, spatial neglect |
| Temporal lobe | Inability to understand language (Wernicke's aphasia - speech is fluent but meaningless), memory loss, hearing problems |
| Occipital lobe | Vision loss, visual field defects (e.g., hemianopia - loss of half the visual field) |
| Brainstem | Dizziness, double vision, facial weakness, difficulty swallowing, loss of consciousness, "locked-in" syndrome in severe cases |
| Cerebellum | Loss of coordination and balance (ataxia), unsteady gait |
| Basal ganglia / deep | Movement disorders, slurred speech |
A key principle: the brain controls the opposite side of the body (contralateral control). A left-hemisphere stroke causes right-sided weakness, and vice versa.
PART 5: DIAGNOSIS
All patients with suspected stroke should undergo urgent brain imaging.
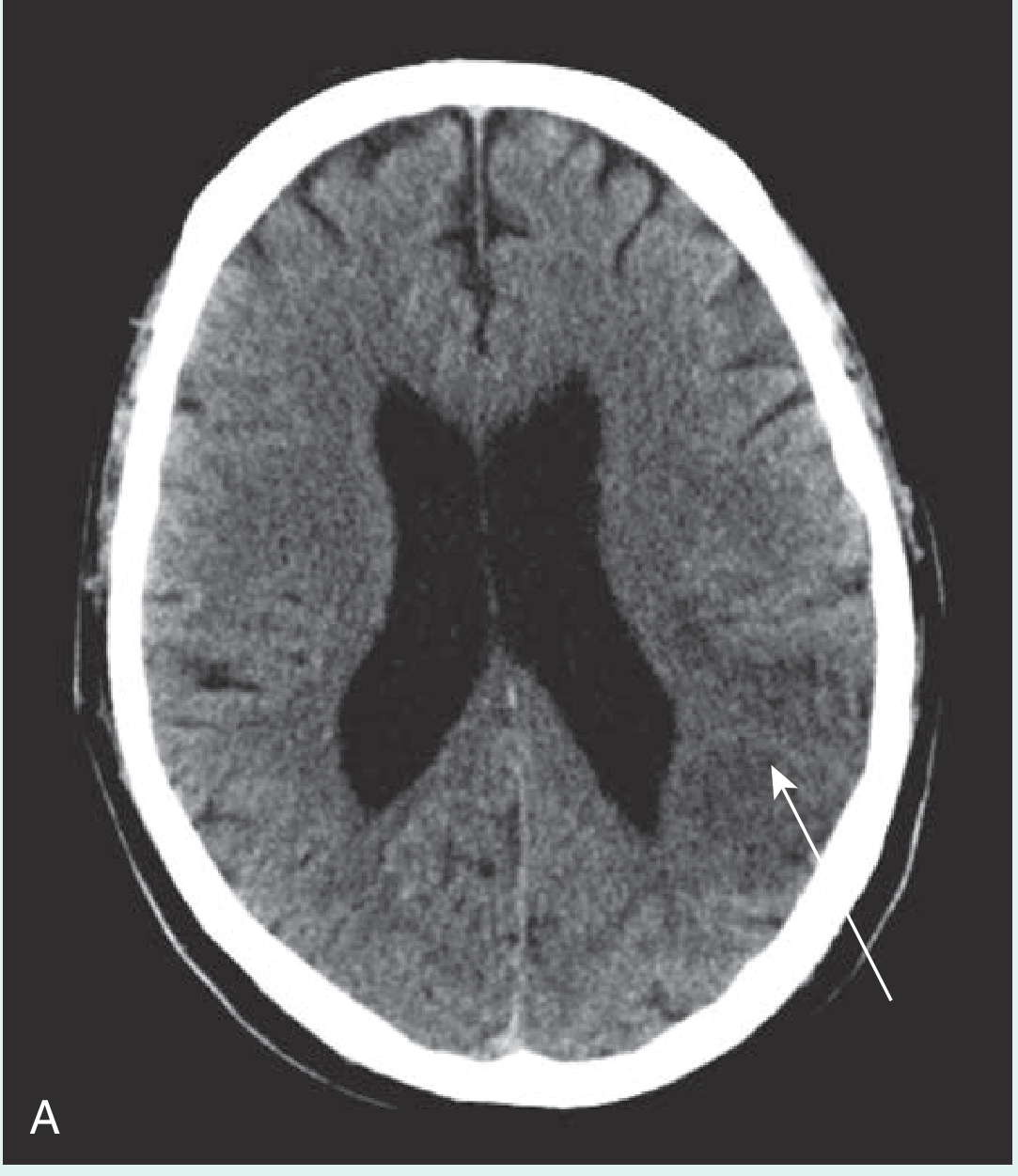
1. CT Scan (First-line, Done Immediately)
- Non-contrast CT is the first step to rule out hemorrhagic stroke (hemorrhage appears bright/white on CT)
- In ischemic stroke, early CT may be normal OR show a darker (low-density) area of abnormal perfusion
- Affected brain loses its normal sulcal pattern due to edema
- Done BEFORE giving thrombolytics (clot-busting drugs), since hemorrhagic stroke is a contraindication
2. MRI Brain
- Better soft tissue resolution than CT
- Identifies strokes too small to see on CT
- T2-weighted sequence: stroke appears as a bright region (acute or chronic)
- DWI (Diffusion-Weighted Imaging): bright on DWI + dark on ADC map = restricted diffusion = acute stroke (persists ~1 week)
- Preferred for posterior fossa (brainstem/cerebellum) strokes
3. Vascular Imaging
- Carotid/vertebral ultrasound - assesses for atherosclerosis and stenosis
- CT angiography (CTA) - rapid mapping of cerebral vessels, identifies occlusion site
- MR angiography (MRA) - alternative vessel imaging
4. Blood Tests
- Full blood count, coagulation screen, glucose (hypoglycemia can mimic stroke), electrolytes, lipid profile, toxicology screen
5. Cardiac Investigation
-
ECG and echocardiography to identify embolic sources (atrial fibrillation, valvular disease, thrombus)
-
Gray's Anatomy for Students; Adams and Victor's Principles of Neurology
PART 6: TREATMENT
A. Acute Ischemic Stroke
1. IV Thrombolysis (Clot-Busting)
- Drug: Alteplase (tPA) - converts plasminogen to plasmin, dissolving the clot
- Standard dose: 0.9 mg/kg IV (max 90 mg), 10% as a bolus, rest over 1 hour
- Time window: Must be given within 3-4.5 hours of symptom onset
- Benefit: ~30% increase in patients with little or no neurologic deficit at 3 months
- Risk: ~6% risk of symptomatic intracerebral hemorrhage
- Contraindicated in: hemorrhagic stroke, massive infarction (>2/3 of MCA territory), recent surgery, uncontrolled hypertension, recent anticoagulant use
- Tenecteplase is a newer alternative with higher fibrin specificity and longer duration of action - showing similar or improved outcomes in some trials
2. Mechanical Thrombectomy
- Physical removal of the clot using a catheter-based device
- Highly effective for large vessel occlusions
- Extended time windows possible with imaging-guided patient selection
3. Antiplatelet Therapy
- Aspirin given early in ischemic stroke (once hemorrhage excluded)
- Long-term antiplatelet therapy is key for secondary prevention
B. Hemorrhagic Stroke
- Blood pressure control to limit hematoma expansion
- Reversal of anticoagulation if relevant
- Neurosurgical intervention for selected cases (large hematomas, hydrocephalus, ruptured aneurysm clipping/coiling)
C. Supportive and Rehabilitation Care (All Stroke Types)
Management is multidisciplinary and includes:
-
Stroke unit care with continuous monitoring
-
Airway, breathing, circulation support
-
Blood sugar and blood pressure management
-
Speech and language therapy (for aphasia, swallowing difficulty)
-
Physiotherapy (for motor rehabilitation)
-
Occupational therapy (for daily activities)
-
Modification of cardiovascular risk factors (blood pressure, diabetes, lipids, smoking cessation)
-
Gray's Anatomy for Students, p. 1020-1021; Adams and Victor's Principles of Neurology, 12th Ed., p. 820-821
Quick Memory Aid: FAST
The most widely used public awareness tool for stroke recognition:
| Letter | Meaning |
|---|---|
| F | Face - drooping on one side |
| A | Arms - one arm weak or drifting down |
| S | Speech - slurred or unable to speak |
| T | Time - call emergency services immediately |
"Time is brain" - every minute of delay in ischemic stroke results in approximately 1.9 million neurons dying.
Sources: Adams and Victor's Principles of Neurology, 12th Ed. | Neuroscience: Exploring the Brain, 5th Ed. | Gray's Anatomy for Students | Fuster and Hurst's The Heart, 15th Ed. | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.