management of severe diarrhea explanation with flowchart
"acute diarrhea" AND management
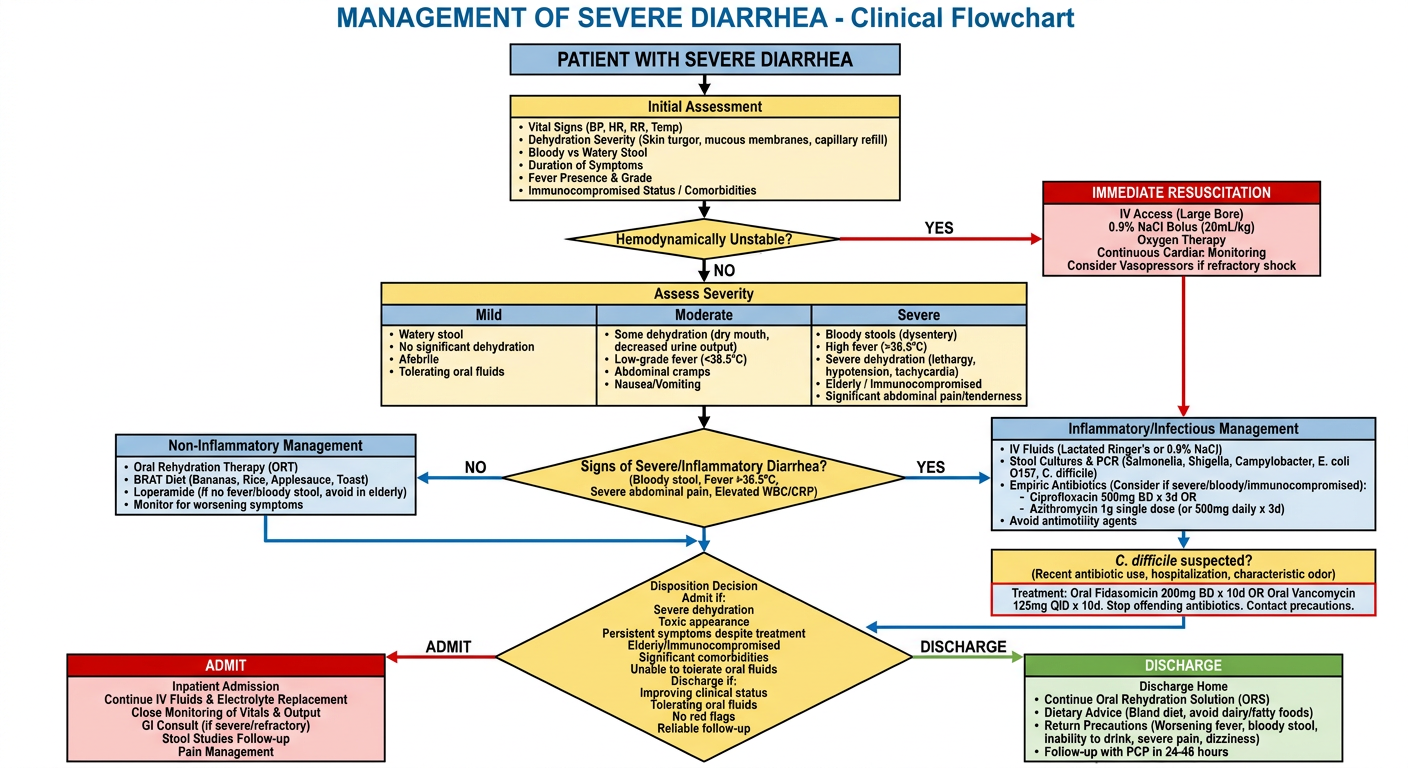
A detailed clinical management flowchart for severe diarrhea. Clean medical diagram with boxes, arrows, and decision diamonds. Flow starts at top with "PATIENT WITH SEVERE DIARRHEA" then branches through: 1) Initial Assessment box (vital signs, dehydration severity, bloody vs watery stool, duration, fever, immunocompromised status), 2) Decision diamond "Hemodynamically Unstable?" - YES leads to "IMMEDIATE RESUSCITATION: IV access, 0.9% NaCl bolus, oxygen, monitor", NO continues down, 3) "Assess Severity" box with three columns: Mild (watery, no dehydration, afebrile), Moderate (some dehydration, fever, cramps), Severe (bloody stools, high fever, severe dehydration, elderly/immunocompromised), 4) Decision diamond "Signs of Severe/Inflammatory Diarrhea?" (bloody stool, fever >38.5C, WBC elevated), 5) Two parallel branches: LEFT "Non-Inflammatory" - Oral rehydration therapy, BRAT diet, Loperamide, monitor; RIGHT "Inflammatory/Infectious" - IV fluids, stool cultures (Salmonella, Shigella, Campylobacter, C. diff), empiric antibiotics (Ciprofloxacin 500mg BD x3d or Azithromycin 1g), 6) Special box "C. difficile suspected?" - Metronidazole or oral Vancomycin, stop offending antibiotics, 7) "Disposition Decision" diamond - Admit if: severe dehydration, toxic appearance, persistent despite treatment, elderly/immunocompromised; Discharge if: improving, tolerating oral fluids, no red flags, 8) Bottom boxes: ADMIT - IV fluids, electrolyte monitoring, GI consult vs DISCHARGE - ORS, dietary advice, return precautions. Color coding: red for emergency actions, yellow for assessments, green for discharge, blue for treatment. Title at top: MANAGEMENT OF SEVERE DIARRHEA - Clinical Flowchart
Management of Severe Diarrhea
1. Definition and Initial Classification
2. Initial Assessment
History - Key Questions
| Question | Why It Matters |
|---|---|
| Bloody or melenic stool? | Suggests invasive infection (Shigella, E. coli O157), ischemia, IBD |
| Fever? | Points to inflammatory/invasive etiology |
| Recent antibiotics or hospitalization? | Risk for C. difficile |
| Travel history? | Traveler's diarrhea (Salmonella, E. coli, Campylobacter) |
| Immunocompromised? | Broadens differential; higher risk of serious infection |
| Food exposure? | Food poisoning, Giardia from rural water sources |
| Resolves with fasting? | Yes = osmotic diarrhea; No = secretory diarrhea |
Physical Examination
- Vital signs: fever, tachycardia, hypotension - signs of hemodynamic instability
- Hydration status: skin turgor, mucous membranes, capillary refill
- Abdominal exam: peritoneal signs, tenderness, masses, surgical scars
- Rectal exam: check for blood, fecal impaction (especially in elderly)
- Look for clues: thyroid enlargement (thyrotoxicosis), oral ulcers/erythema nodosum/anal fissure (IBD), arthritis + conjunctivitis + urethritis (Reiter's - suggests Salmonella/Shigella)
Red flag: An elderly patient with bloody diarrhea and abdominal pain out of proportion to examination may have mesenteric ischemia - a true emergency.
3. Severity Stratification
| Feature | Mild | Moderate | Severe |
|---|---|---|---|
| Stool character | Watery, non-bloody | Watery/mucoid, may be bloody | Grossly bloody, large volume |
| Dehydration | None | Mild to moderate | Severe |
| Fever | None/low grade | Moderate (38-38.5°C) | High (>38.5°C) |
| Systemic symptoms | Minimal | Cramps, nausea | Toxic appearance, prostration |
| Stool fecal WBCs | Absent | May be present | Present |
4. Immediate Resuscitation (if hemodynamically unstable)
- IV access x2, cardiac monitoring, pulse oximetry
- Fluid bolus: 0.9% Normal Saline or Lactated Ringer's 500 mL - 1 L IV over 30-60 minutes
- Correct electrolyte abnormalities (especially hypokalemia, hyponatremia)
- Check point-of-care glucose
- NPO initially until stabilized, then transition to oral fluids
5. Diagnostic Workup
- Diarrhea lasting >3 days
- Bloody stools or fecal leukocytes present
- Fever >38.5°C
- Immunocompromised host
- Signs of dehydration requiring IV fluids
- Suspected outbreak/public health concern
- Stool cultures: Salmonella, Shigella, Campylobacter, E. coli O157:H7
- C. difficile toxin PCR (if recent antibiotics or hospitalization)
- Ova and parasites (if travel or prolonged illness)
- Blood tests: CBC (leukocytosis suggests invasive infection), BMP (electrolytes, renal function), blood cultures if septic
- Abdominal imaging: Consider CT abdomen if peritoneal signs or suspected ischemia/perforation
6. Treatment
A. Rehydration
- WHO ORS formula, Pedialyte, Ceralyte 90
- Fluids: chicken broth with fruit juices, Gatorade, non-caffeinated drinks
- Foods: complex carbohydrates (bananas, rice, bread, apple juice, tortillas), crackers, Lactobacillus-containing yogurt (BRAT-style diet)
- Normal saline or Lactated Ringer's
- Monitor electrolytes every 4-6 hours during active resuscitation
B. Antimotility Agents (for non-inflammatory diarrhea)
| Drug | Dose | Notes |
|---|---|---|
| Loperamide (Imodium) | 4 mg initially, then 2 mg after each loose stool; max 16 mg/day x2 days | Preferred first-line; minimal central opioid effects; can combine with antibiotics |
| Bismuth subsalicylate (Pepto-Bismol) | 30 mL or 2 tablets every 30 min x8 doses | Risk of salicylate toxicity with excess; avoid in HIV patients |
| Diphenoxylate/atropine (Lomotil) | 4 mg four times daily x2 days | Second-line; more central opioid effects |
Important: Do NOT use antimotility agents in suspected invasive/bloody diarrhea, high fever, or C. difficile - they can worsen toxic megacolon and bacteremia.
C. Antibiotics (empiric and targeted)
- Moderate to severe traveler's diarrhea
- Immunocompromised host
- High fever with bloody diarrhea
- Clinical toxicity
| Antibiotic | Dose | Indications |
|---|---|---|
| Ciprofloxacin | 500 mg single dose OR 500 mg BD x3 days | First choice for moderately severe illness; most regions (except South/Southeast Asia) |
| Azithromycin | 1000 mg single dose | First choice in South and Southeast Asia; safe in children and pregnancy |
| Rifaximin | 200 mg three times daily x3 days | Moderately severe illness; do NOT use if fever or bloody stools; avoid in pregnancy |
D. C. difficile-Specific Treatment
- Stop the offending antibiotic if possible
- Mild to moderate C. diff: Oral metronidazole 500 mg three times daily x10-14 days
- Severe C. diff (WBC >15,000 or creatinine >1.5x baseline): Oral vancomycin 125 mg four times daily x10-14 days
- Fulminant C. diff (hypotension, ileus, megacolon): IV metronidazole + high-dose oral/rectal vancomycin; surgical consult
E. Special Situations
| Situation | Management |
|---|---|
| Traveler's diarrhea | Rehydration + Azithromycin (South/SE Asia) or Ciprofloxacin (elsewhere) + Loperamide for symptom control |
| IBD flare | IV steroids, GI consult, hold immunosuppressives if infection not excluded |
| Elderly with bloody diarrhea | Rule out mesenteric ischemia with CT; lower threshold for admission |
| Immunocompromised | Broad workup including CMV, Cryptosporidium, MAC; GI and ID consult |
| Children | ORS priority; avoid Loperamide under age 2; consider probiotics (Lactobacillus rhamnosus GG) |
7. Disposition Decision
Admit if:
- Severe dehydration not responding to initial IV therapy
- Toxic clinical appearance
- Symptoms persisting or worsening despite appropriate outpatient management
- Bloody diarrhea with fever in elderly or immunocompromised
- Suspected C. difficile with severe criteria
- Need for IV antibiotics
- Surgical concern (C. diff colitis, ischemia, obstruction)
Discharge if:
- Improving with treatment
- Tolerating oral fluids
- No red flags or high-risk features
- Reliable follow-up available
8. Summary
- Assess - severity, cause (inflammatory vs. non-inflammatory), host factors
- Resuscitate - IV fluids first if unstable
- Investigate - selectively, based on red flags
- Treat - rehydration + targeted therapy (antibiotics only when indicated)
- Decide - admit vs. discharge based on response and risk
parenteral rehydration pharmacological basis of uses in diarrhea. its use indication and criteria, its risk and effects...
"intravenous fluid" AND "rehydration" AND "diarrhea"
A detailed clinical flowchart titled "Parenteral Rehydration in Severe Diarrhea" with clean medical diagram style, boxes with rounded corners, decision diamonds, and color-coded sections. Flow: TOP: "Patient with Severe Diarrhea" → "Assess Hydration Status" with three severity columns (Mild/Moderate/Severe) → Decision diamond "Can patient tolerate oral intake?" YES leads to "Oral Rehydration Therapy (ORS)" box, NO leads to "PARENTERAL REHYDRATION INDICATED" red box → "Establish IV Access (Large bore 16G x2)" → "Choose IV Fluid" box showing: Normal Saline 0.9% (154 mEq/L Na+Cl-), Lactated Ringer's (Na 130, K 4, Ca 2.7, Lactate 28, Cl 109), Ringers with potassium → Decision diamond "Cholera/Massive Output?" YES → Rapid bolus 30 mL/kg in 30 min, NO → 500mL crystalloid over 20-30 min → "Monitor Response" box: urine output >0.5 mL/kg/hr, BP, HR, electrolytes → "Electrolyte Correction" box: Add KCl if K<3.5, NaHCO3 if acidotic, Correct hyponatremia slowly → Decision diamond "Stabilized?" YES → Transition to ORS, NO → Continue IV fluids + reassess → SIDE BOX: Red "Contraindications to Oral Route" listing: unconscious, vomiting, ileus, shock, severe dehydration → BOTTOM BOX: Green "Risks and Adverse Effects": fluid overload, pulmonary edema, hyperchloremic acidosis (NS), hyponatremia (hypotonic fluids), phlebitis, infection at IV site, rapid correction complications. Color: blue header, yellow for assessment, orange for indications, red for warnings, green for outcomes