Malaria (life cycle, pathogenesis, lab diagnosis, cerebral malaria, severe malaria criteria, Babesiosis)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have all the material needed to compile a comprehensive answer. Here is the full response:
Malaria: Complete Review
Sources: Harrison's Principles of Internal Medicine 22E (2025), Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease
1. LIFE CYCLE

Species
Six species infect humans: P. falciparum, P. vivax, P. ovale (curtisi and wallikeri), P. malariae, and P. knowlesi (Southeast Asia). Humans are also occasionally infected by monkey parasites P. simium and P. cynomolgi. Almost all deaths are caused by falciparum malaria, though P. knowlesi and occasionally P. vivax can cause severe illness.
Human (Asexual) Cycle
Step 1 - Hepatic (Pre-erythrocytic) Stage:
- Female Anopheles mosquito inoculates sporozoites from salivary glands during a blood meal
- Sporozoites travel rapidly to the liver via bloodstream
- Two surface proteins - thrombospondin-related adhesive protein and circumsporozoite protein - bind heparan sulfate proteoglycans on hepatocytes
- Inside hepatocytes: asexual reproduction (intrahepatic schizogony) - one sporozoite produces 10,000 to >30,000 daughter merozoites
- Infected hepatocytes burst, releasing merozoites into blood
- Hypnozoites: In P. vivax and P. ovale, a proportion of intrahepatic forms remain dormant for 2 weeks to ≥1 year - these cause relapses (not seen in P. falciparum or P. malariae)
Step 2 - Erythrocytic Stage:
- Merozoites bind erythrocytes via a lectin-like molecule on the merozoite surface binding to sialylated glycophorin (a red cell transmembrane protein)
- Merozoite invaginates into the RBC within a "digestive vacuole"
- Intraerythrocytic forms differentiate: ring stage → trophozoite → schizont
- Multiplication is 6- to 20-fold every 48 h (P. knowlesi: 24 h; P. malariae: 72 h)
- Schizonts differentiate back into merozoites → RBC lyses → new cycle begins
- When parasite density reaches ~50/μL (~100 million parasites), symptomatic stage begins
Gametocyte Formation (Sexual Stage - in Human):
- Some trophozoites develop into gametocytes (male = microgametocytes; female = macrogametocytes) - the infective stage for the mosquito
Mosquito (Sexual) Cycle
- Mosquito ingests gametocytes during a blood meal
- Male gametocyte exflagellates → 8 motile male gametes
- Fusion with female gametocyte → zygote in mosquito midgut
- Zygote matures into ookinete → penetrates mosquito gut wall → oocyst
- Oocyst expands by asexual division → bursts → liberates sporozoites
- Sporozoites migrate to salivary gland → ready for next human bite
Fever Periodicity
| Species | Fever cycle | Fever type |
|---|---|---|
| P. vivax / P. ovale | 48 h (erythrocytic cycle) | Tertian (every 3rd day) |
| P. falciparum | 48 h | Malignant tertian |
| P. malariae | 72 h | Quartan (every 4th day) |
| P. knowlesi | 24 h | Quotidian (daily) |
2. PATHOGENESIS
Erythrocyte Changes & Sequestration (P. falciparum)
The most critical pathogenic mechanism unique to P. falciparum is sequestration of parasitized RBCs in microvascular beds of vital organs.
Schizonts express PfEMP1 (P. falciparum erythrocyte membrane protein 1) - an adhesion molecule that forms knob-like extensions on the infected RBC surface. PfEMP1 binds endothelial adhesion molecules:
- ICAM-1 (intercellular adhesion molecule-1)
- VCAM-1 (vascular cell adhesion molecule-1)
- CD36
- Thrombospondin, E-selectin, chondroitin sulfate A (placenta)
This causes parasitized RBCs to arrest in capillary beds - especially brain, kidney, lung, gut, heart.
Three key processes:
- Cytoadherence - infected RBCs stick to endothelium via PfEMP1
- Rosetting - infected RBCs bind uninfected RBCs
- Agglutination - infected RBCs clump together
Consequences of Sequestration
- Microvascular obstruction → tissue hypoxia and lactic acidosis
- Impaired consciousness (cerebral malaria)
- Organ dysfunction
Fever Mechanism
- Synchronous rupture of schizonts releases merozoites + malaria pigment (hemozoin) + membrane glycolipids (GPI anchors) into bloodstream
- These trigger macrophage release of TNF-α, IL-1, IL-6 → fever, rigors, prostration
- Classic paroxysm: 15-60 min cold stage (rigors) → 2-6 h hot stage (fever 40-41°C) → 2-4 h sweating stage
Anemia
- Destruction of infected RBCs at schizont rupture
- Clearance of uninfected RBCs (bystander hemolysis)
- Dyserythropoiesis (bone marrow suppression by cytokines)
- Splenic sequestration
Hypoglycemia
- Parasite consumes glucose; P. falciparum consumes up to 75 times more glucose than uninfected RBCs
- Impaired hepatic gluconeogenesis
- Quinine/quinidine stimulate insulin release from pancreatic beta cells
Cytokine Storm
- TNF-α, IL-1, IL-6, IL-10, IFN-γ mediate systemic effects
- TNF-α upregulates ICAM-1 on endothelium → more cytoadherence (vicious cycle)
3. LABORATORY DIAGNOSIS
Gold Standard: Blood Smear Microscopy
Two types should always be prepared simultaneously:
| Feature | Thick Film | Thin Film |
|---|---|---|
| Preparation | Uneven thickness; stained unfixed (lysed RBCs) | Air-dried, methanol-fixed, then stained |
| Stain | Giemsa (pH 7.2), Field's, or Leishman's | Same |
| Reading | Parasites per 200 WBCs (>500 WBCs at low density) | Parasitized RBCs per 1000 RBCs |
| Sensitivity | 0.001% parasitemia (40-100x concentration) | <0.05% parasitemia |
| Advantage | Most sensitive | Species identification; morphology; prognostic staging |
| Disadvantage | Artifacts mimic parasites; experience needed | Insensitive at low parasitemia |
"Malaria is not a clinical diagnosis" - Harrison's 22E. If the smear is negative by an experienced microscopist, the patient does not have malaria.
Staining tip: Acridine orange (fluorescent dye) allows rapid diagnosis in low-level parasitemia but does NOT allow speciation.
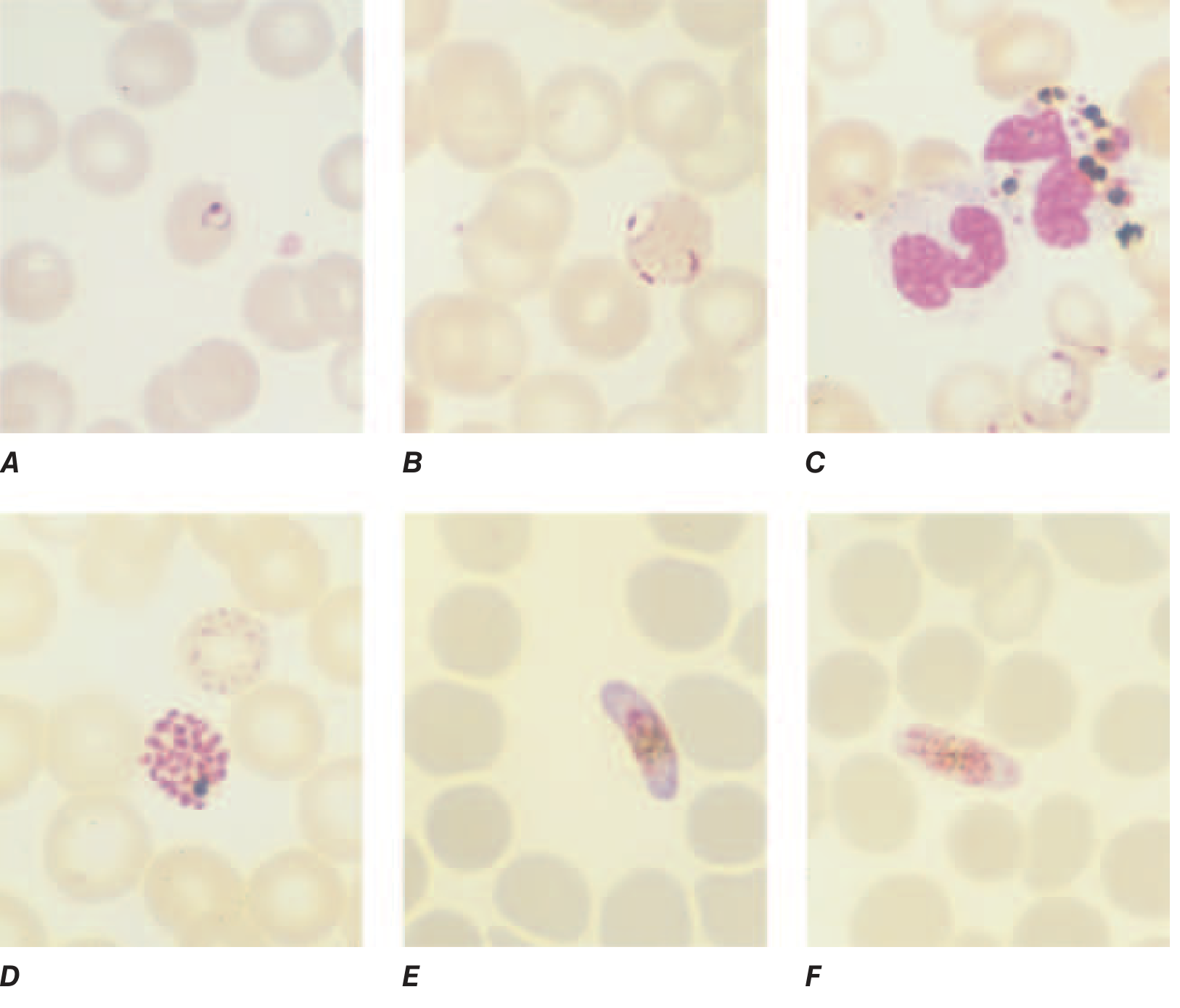
Morphological Clues for Speciation (Thin Smear)
| Feature | P. falciparum | P. vivax | P. ovale | P. malariae |
|---|---|---|---|---|
| RBC size | Normal or smaller | Enlarged | Enlarged, oval, fimbriated (James dots) | Normal |
| Stippling | Maurer's clefts | Schüffner's dots | Schüffner's dots | Ziemann's dots |
| Multiple infections/RBC | Common (2-3 rings) | Rare | Rare | Rare |
| Schizont | Rarely seen in peripheral blood (sequestered) | >12 merozoites (rosette) | 8 merozoites | "Daisy head" / band form trophozoite (8 merozoites) |
| Gametocyte | Banana/crescent shaped (diagnostic) | Round | Round | Round |
| Parasitemia | Can be very high (>5%) | <2% | <1% | <1% |
Rapid Diagnostic Tests (RDTs)
Antigen-based immunochromatographic tests detecting:
- HRP-2 (Histidine-rich protein 2) - P. falciparum specific; may remain positive for weeks after treatment (persists as free antigen)
- pLDH (parasite lactate dehydrogenase) - pan-malarial; becomes negative within days of effective treatment (useful for treatment monitoring)
- Aldolase - pan-malarial
RDTs: sensitivity ~95%, specificity ~90% for P. falciparum; less sensitive for non-falciparum species.
Other Laboratory Methods
| Method | Details |
|---|---|
| PCR | Most sensitive (detects submicroscopic infections); species + drug resistance typing; not for routine diagnosis |
| Serology (ELISA/IFA) | Detects antibodies; useful for retrospective diagnosis or blood donor screening; NOT for acute diagnosis |
| QBC (Quantitative Buffy Coat) | Fluorescence microscopy with acridine orange; sensitive but no speciation |
Laboratory Findings in Acute Malaria (non-specific)
- Anemia - normochromic normocytic
- Thrombocytopenia (characteristic; <150,000/μL common)
- Leukopenia or normal WBC (leukocytosis suggests bacterial superinfection)
- Elevated LDH, bilirubin (hemolysis)
- Elevated liver enzymes (mild)
- Low glucose, low sodium
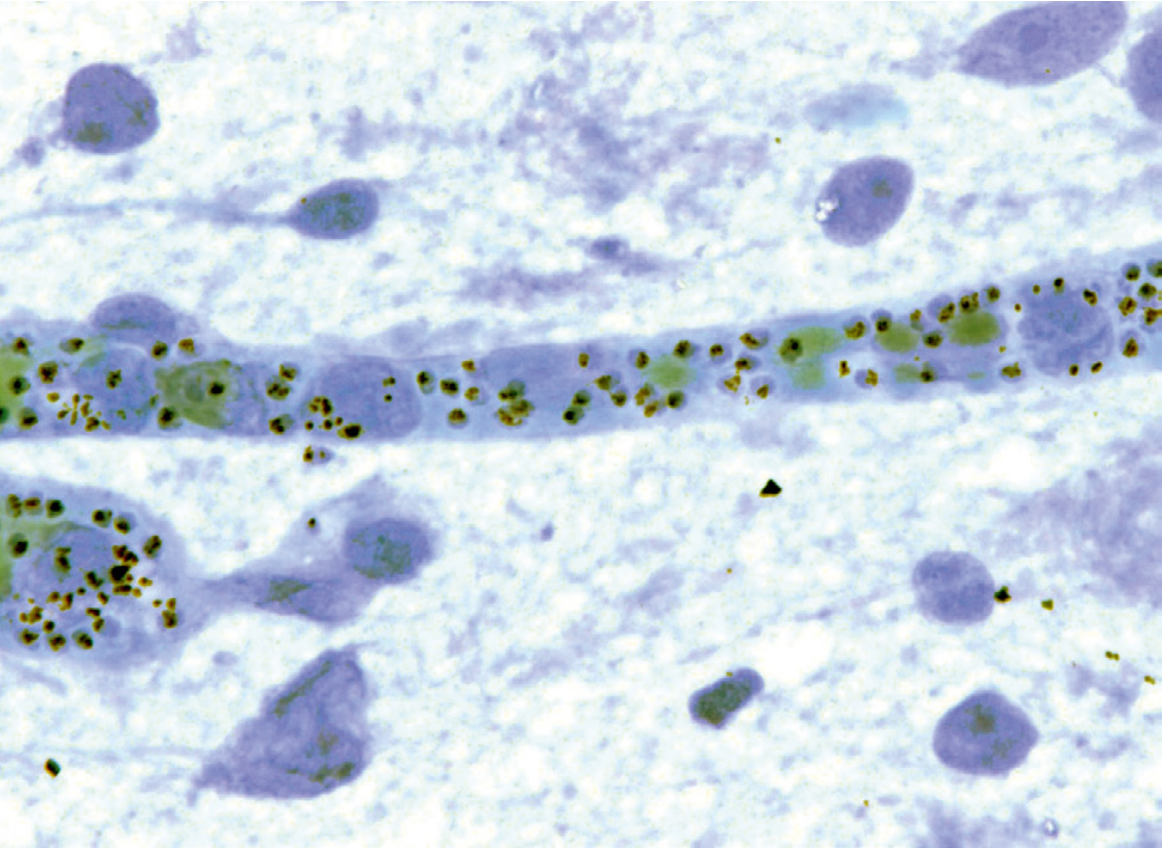
- Malaria pigment (hemozoin) in neutrophils and monocytes on peripheral smear - poor prognostic sign
4. CEREBRAL MALARIA
Definition
Unarousable coma in a patient with P. falciparum parasitemia, with no other identifiable cause of coma (meningitis, hypoglycemia, etc.).
- Glasgow Coma Score <11 in adults
- Blantyre Coma Score <3 in children
- Coma must persist >30 min after a generalized convulsion
Pathogenesis
- Sequestration of parasitized RBCs in cerebral microvessels (via PfEMP1/ICAM-1 binding)
- Mechanical obstruction → reduced oxygen delivery
- Inflammatory cytokines (TNF-α) upregulate ICAM-1 on cerebral endothelium → more sequestration
- Edema (cytotoxic > vasogenic)
- Petechial hemorrhages ("ring hemorrhages" around sequestered RBCs - Durck's granulomas seen histologically)
- Contribution of rosetting and agglutination
Clinical Features
- Diffuse, symmetric encephalopathy - focal neurologic signs are unusual
- Onset may be gradual or sudden after a convulsion
- Eyes: may be divergent; bruxism (jaw clenching); pout reflex common
- Corneal reflexes preserved except in deep coma
- Muscle tone may be increased or decreased; variable tendon reflexes; plantar reflexes may be flexor or extensor; abdominal and cremasteric reflexes absent
- Convulsions in ~10% of adults; up to 50% of children (often generalized, repeated)
- Subtle seizures in children: repetitive tonic-clonic eye movements, hypersalivation
Retinal Findings (Malarial Retinopathy - Pathognomonic)
- Retinal whitening/opacification - discrete pale spots (30-60%)
- Pale-centered retinal hemorrhages (flame-shaped with white center)
- Vessel decolorization (whitening of vessels or segments)
- Papilledema (8% in children, rare in adults)
- Routine fundoscopy: retinal hemorrhages in ~15%; with pupillary dilation + indirect ophthalmoscopy: 30-40%

Prognosis
- Even with treatment: mortality ~20% in adults, ~15% in children
- Neurologic sequelae in <3% of adults
- Neurologic sequelae in ~10% of children (hemiplegia, cerebral palsy, cortical blindness, deafness, impaired cognition, epilepsy)
- Most deficits improve within 6 months; ~10% have persistent language deficits
- Durck's granulomas - histological hallmark: microglial nodules around necrotic foci where a capillary was blocked by a parasitized RBC
5. SEVERE MALARIA CRITERIA (WHO / Harrison's 22E)
Mortality rises steeply once vital-organ dysfunction occurs OR parasitemia >2% (>10¹² parasites in adult). Parenteral artesunate reduces mortality by 35% in Asian adults/children and 22.5% in African children vs quinine.
Major Manifestations (Table 231-2, Harrison's 22E)
| Manifestation | Criteria |
|---|---|
| Unarousable coma / Cerebral malaria | Failure to localize or respond to noxious stimuli; coma >30 min after convulsion; GCS <11 or Blantyre Coma Score <3 in children |
| Acidemia / Acidosis | Arterial pH <7.25; base deficit >8 meq/L; serum HCO₃ <15 mmol/L; venous lactate ≥5 mmol/L; manifests as "respiratory distress" (labored deep breathing) |
| Severe normochromic normocytic anemia | Hematocrit <15% OR Hb <50 g/L (<5 g/dL) with parasitemia >10,000/μL |
| Renal impairment | Serum creatinine >265 μmol/L (3 mg/dL) or urine output <400 mL/24h |
| Pulmonary edema / ARDS | Non-cardiogenic; may develop even after treatment starts; mortality >80% |
| Hypoglycemia | Plasma glucose <2.2 mmol/L (<40 mg/dL) |
| Circulatory collapse / Shock | Systolic BP <70 mmHg + cold, clammy skin; "Algid malaria" - septicemic shock from gut-organism translocation |
| Abnormal bleeding / DIC | Spontaneous bleeding from gums, nose, GI tract |
| Hyperparasitemia | >5% parasitized RBCs in low-transmission areas; increased mortality at >100,000/μL, high mortality at >500,000/μL |
| Impaired consciousness | Not unarousable but any delirium or obtundation |
| Prostration / Weakness | Inability to sit unsupported |
| Repeated convulsions | >2 in 24 hours |
| Macroscopic hemoglobinuria (Blackwater Fever) | Dark/black urine from massive intravascular hemolysis |
| Jaundice | Bilirubin >50 μmol/L with other evidence of vital-organ dysfunction |
Poor Prognosis Markers (Table 231-3, Harrison's 22E)
Clinical:
- Hyperparasitemia (>10% in nonimmune)
- Deep coma, papilledema, decerebrate posturing
- Hypotension, pulmonary edema
- Hyperpyrexia (>40°C)
- Repeated convulsions
- Age <3 years
Laboratory:
| Category | Finding |
|---|---|
| Biochemistry | Acidemia (pH <7.25), elevated creatinine, elevated bilirubin, elevated AST/ALT (>3× ULN), elevated CPK/myoglobin, elevated urate (>600 μmol/L) |
| Hematology | Leukocytosis (>12,000/μL), severe anemia (PCV <10%), low platelets (<50,000/μL), prolonged PT (>3 sec), prolonged PTT, low fibrinogen (<200 mg/dL) |
| Parasitology | >100,000 parasites/μL (increased mortality); >500,000/μL (high mortality); >20% parasites as pigment-containing trophozoites and schizonts; >5% neutrophils containing visible malaria pigment |
Plasma bicarbonate or lactate levels are the best biochemical prognosticators in severe malaria.
6. BABESIOSIS
Overview
Babesiosis is caused by intraerythrocytic protozoan parasites of the genus Babesia - malaria-like organisms transmitted by Ixodid ticks (not mosquitoes).
Species and Epidemiology
| Species | Vector | Geography | Reservoir |
|---|---|---|---|
| B. microti | Ixodes scapularis (deer tick) | Northeastern + N. Midwestern USA | White-footed mouse |
| B. divergens | I. ricinus (sheep tick) | Europe | Cattle |
| B. duncani | I. pacificus | Western USA | Unknown |
| B. venatorum | I. persulcatus | Northwestern China, Europe | Roe deer |
- Incidence in the USA has significantly increased in the past 2 decades alongside expansion of tick populations and geographic range
- Transfusion-transmitted babesiosis is well-recognized - B. microti survives well in refrigerated blood → specific screening tests are now used for donated blood in endemic areas
Clinical Features
- Majority of infections: asymptomatic or mild flu-like illness
- Symptomatic disease: fever, jaundice, hemoglobinuria, hemolytic anemia
- Severe/fatal disease in:
- Asplenic individuals (splenectomized)
- Immunocompromised (HIV, organ transplant, rituximab)
- Elderly
- Parasitemia can reach up to 30% in asplenic persons (vs ~1% in mild cases)
- Severe complications: hepatic necrosis, acute tubular necrosis, ARDS, erythrophagocytosis, visceral hemorrhage
Lab Diagnosis - Blood Smear
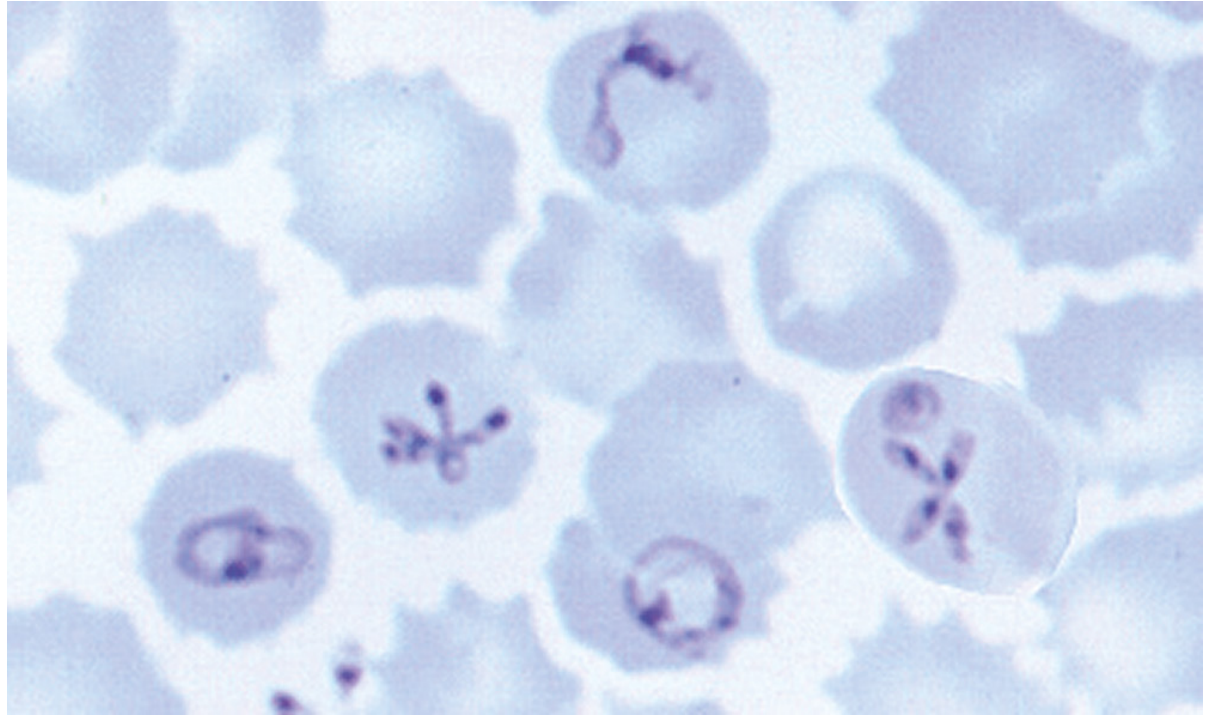
On Giemsa-stained peripheral blood smear, Babesia organisms:
- Superficially resemble P. falciparum ring stages
- Key differences from malaria:
- NO hemozoin (malaria pigment)
- Greater pleomorphism
- Rings may be outside the RBC
- Tetrad form ("Maltese cross" / "cross of Lorraine") - 4 merozoites arranged in a cross, pathognomonic when found (though uncommon)
- Multiple infections per RBC common (like falciparum), but the lack of pigment and extracellular rings distinguish them
Comparison: Babesiosis vs P. falciparum
| Feature | Babesiosis | P. falciparum |
|---|---|---|
| Malaria pigment (hemozoin) | Absent | Present |
| Tetrad (Maltese cross) | Present (pathognomonic) | Absent |
| Gametocytes | Absent | Banana-shaped |
| Extracellular rings | Present | Absent |
| Enlarged infected RBC | No | No (normal/smaller) |
| Vector | Ixodes tick | Anopheles mosquito |
| Hypnozoites | No | No (only vivax/ovale) |
Diagnosis of Babesiosis
- Peripheral blood smear (Giemsa) - as above; Maltese cross pathognomonic but rare
- PCR - most sensitive; useful in low-level parasitemia
- Serology (IFA) - antibody detection; useful for diagnosis and blood bank screening
- Animal inoculation (hamsters) - historical gold standard; no longer routine
Treatment
- Mild-to-moderate: Atovaquone + azithromycin
- Severe: Clindamycin + quinine (IV in very severe cases)
- Exchange transfusion considered for parasitemia >10%, severe hemolysis, or organ failure
Harrison's Principles of Internal Medicine 22E (2025), pp. 1804-1876 | Robbins & Kumar Basic Pathology | Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.