Bells palsy as per harrison with management in details
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
"Bell palsy" AND treatment
Reading File
Loading Image
I now have all the content needed. Here is the complete, detailed answer based on Harrison's Principles of Internal Medicine 22nd Edition (2025).
Bell's Palsy - Harrison's Principles of Internal Medicine (22nd Ed., 2025)
Definition & Epidemiology
Bell's palsy is the most common form of facial paralysis. It is an idiopathic disorder characterized by acute onset unilateral facial nerve (CN VII) palsy.
- Annual incidence: ~25 per 100,000 (approximately 1 in 60 persons over a lifetime)
- Risk factors: pregnancy and diabetes mellitus
Clinical Manifestations
- Onset is fairly abrupt, with maximal weakness reached within 48 hours as a general rule
- Pain behind the ear may precede the paralysis by 1-2 days
- Unilateral loss of taste (ageusia) may occur
- Hyperacusis (sound sensitivity) due to paralysis of the stapedius muscle
- Mild CSF lymphocytosis may be present in some cases
- MRI may reveal swelling and uniform enhancement of the geniculate ganglion and facial nerve, and in some cases, entrapment of the swollen nerve in the temporal bone
Prognosis:
- ~80% of patients recover within a few weeks to months
- EMG after 10 days showing denervation indicates axonal degeneration - expect a long delay (~3 months) before regeneration, which may be incomplete
- Incomplete paralysis in the first week = most favorable prognostic sign
- Recurrence rate: ~7% of cases
Pathophysiology
- Acute Bell's palsy shows inflammation of the facial nerve with mononuclear cells, consistent with an infectious or immune cause
- HSV type 1 DNA has been frequently detected in endoneurial fluid and posterior auricular muscle - reactivation of HSV-1 in the geniculate ganglion is the likely cause in most cases
- Varicella-zoster virus (VZV) reactivation is associated with Bell's palsy in up to one-third of cases (the second most frequent cause)
- Other implicated viruses include SARS-CoV-2
- Bell's palsy can also occur in the setting of HIV seroconversion
Differential Diagnosis
Bell's palsy is a diagnosis of exclusion. The following must be considered:
| Condition | Features |
|---|---|
| Lyme disease | Unilateral or bilateral facial palsy; in endemic areas, ≥10% of facial palsies are due to Borrelia burgdorferi |
| Ramsay Hunt syndrome | Reactivation of herpes zoster in geniculate ganglion; severe facial palsy + vesicular eruption in external auditory canal ± pharynx; CN VIII often affected |
| Sarcoidosis | Often bilateral facial palsy |
| Guillain-Barré syndrome | Often bilateral facial palsy |
| Leprosy | Frequently involves facial nerve |
| Diabetes mellitus | Facial neuropathy |
| Connective tissue diseases | Including Sjögren's syndrome and amyloidosis |
| Melkersson-Rosenthal syndrome | Recurrent facial paralysis + recurrent/permanent facial (labial) edema ± plication of tongue; unknown cause |
| Acoustic neuroma | Facial nerve compression |
| Pontine lesions | Infarcts, MS plaques, tumors; other brainstem signs usually present |
| Tumors | Invading temporal bone (carcinoma, cholesteatoma) |
Supranuclear (UMN) vs. Nuclear/Peripheral (LMN) distinction:
In supranuclear lesions, the forehead is spared (frontalis and orbicularis oculi are less affected) because the upper facial muscles receive bilateral cortical input. In Bell's palsy (peripheral), all ipsilateral facial muscles including the forehead are equally affected. Supranuclear lesions may also show dissociation of emotional vs. voluntary movements and associated limb weakness or aphasia.
Laboratory Evaluation
Clinical diagnosis is sufficient when:
- Typical presentation
- No risk factors or symptoms pointing to other causes
- No cutaneous herpes zoster lesions in the external ear canal
- Normal neurologic exam except for facial nerve
Atypical or uncertain cases may require:
- ESR or CRP
- Fasting glucose / HbA1c (for diabetes)
- Lyme titer
- HIV serologies
- ACE level + chest imaging (for sarcoidosis)
- Lumbar puncture (for Guillain-Barré syndrome)
- MRI with gadolinium
MRI Findings (Figure 452-4)
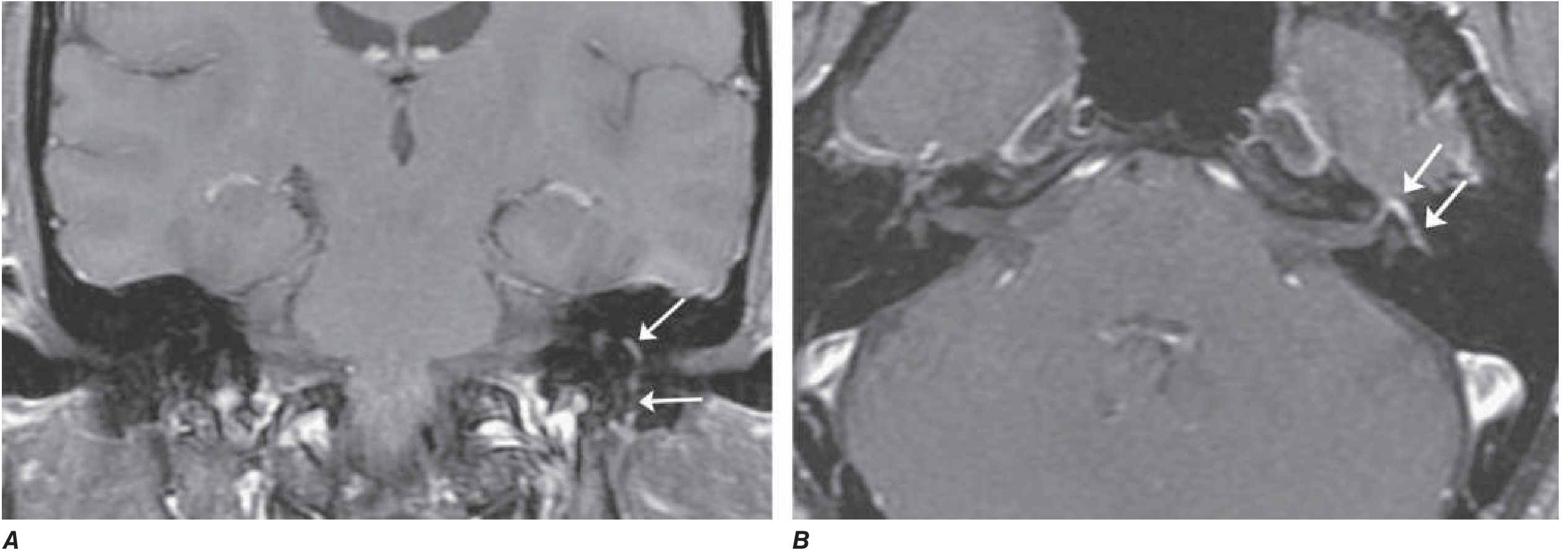
Axial (B) and coronal (A) T1-weighted images after gadolinium with fat suppression demonstrate diffuse smooth linear enhancement of the left facial nerve, involving the genu, tympanic, and mastoid segments within the temporal bone (arrows), without evidence of mass lesion. Although highly suggestive of Bell's palsy, similar findings may be seen with Lyme disease, sarcoidosis, and perineural malignant spread.
Management (Harrison's Treatment Box)
1. Symptomatic / Eye Care Measures
- Paper tape to depress the upper eyelid during sleep - prevents corneal drying and exposure keratopathy
- Artificial tears (lubricating eye drops) throughout the day
- Massage of the weakened muscles
2. Glucocorticoids (First-line treatment)
Prednisone 60-80 mg daily for the first 5 days, then tapered over the next 5 days
- Modestly shortens recovery and improves functional outcome
- Should be started as early as possible (ideally within 72 hours of onset)
3. Antiviral Agents
- Valacyclovir 1000 mg daily for 5-7 days, OR
- Acyclovir 400 mg five times daily for 10 days
Key point from Harrison's: Large, well-controlled randomized trials found no added benefit of antivirals compared to glucocorticoids alone. However, either agent should be used if vesicular lesions are observed in the palate or external auditory canal (suggesting Ramsay Hunt syndrome).
4. Surgical Management
- For patients with permanent paralysis from Bell's palsy, various cosmetic surgical procedures can be used to restore relatively symmetric facial appearance
Summary Table
| Aspect | Detail |
|---|---|
| Incidence | ~25/100,000/year |
| Maximal weakness | Within 48 hours |
| Key symptom | Unilateral facial palsy (all divisions) |
| Associated features | Retroauricular pain, ageusia, hyperacusis |
| Primary cause | HSV-1 reactivation (geniculate ganglion) |
| Recovery | ~80% within weeks-months |
| Steroid regimen | Prednisone 60-80 mg/day x 5 days, taper over next 5 days |
| Antiviral use | Add only if vesicles present (Ramsay Hunt) |
| Eye protection | Paper tape at night + artificial tears |
| Recurrence | ~7% |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 452 - Cranial Nerve Disorders, pp. 3597-3599
Recent evidence note: A 2025 systematic review (PMID 39647183) on physical therapy for idiopathic facial paralysis found emerging support for physiotherapy as an adjunct to medical management - this is not covered in Harrison's treatment box but represents an evolving area. No recent meta-analyses contradict Harrison's core steroid-first approach.
This is a shared conversation. Sign in to Orris to start your own chat.