I have tense swelling at anus around 12 o clock position without bleeding . It occured as pain during defecation 3 days back and subside by time. Yesterday it was very tense but no tenderness. I had a history of fistulous tract wirh pus collection 3 years back .
Reading File
Finding Sources
Finding Sources
Searching PubMed
perianal abscess recurrence fistula
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough clinical assessment based on your presentation and what authoritative surgical textbooks describe.
Clinical Assessment
Your Key Features
| Feature | Significance |
|---|---|
| Tense perianal swelling at 12 o'clock | Typical location for thrombosed external hemorrhoid OR recurrent perianal abscess |
| Pain during defecation 3 days ago, then subsided | Suggests initial acute phase with possible partial spontaneous decompression |
| Tense but not tender yesterday | Important differentiator - classic thrombosed hemorrhoid resolves its tenderness over days 3-5 as the clot organizes |
| No bleeding | Less likely internal hemorrhoid involvement |
| History of fistulous tract + pus collection 3 years ago | This is the most clinically important feature - raises serious concern for recurrent abscess along the old fistula tract |
Two Leading Diagnoses
1. Thrombosed External Hemorrhoid (Most common for this presentation)
An external hemorrhoid becomes thrombosed with acute onset of perianal pain and development of a purplish/bluish nodule - exactly what you describe. The timeline matches:
- Day 0-2: Acute painful phase (pain during defecation)
- Day 3-5: Clot begins to organize, pain diminishes but swelling remains tense - this is where you are now
- Day 5-10: Gradual resolution OR clot may ulcerate and drain spontaneously
The lack of tenderness at day 3+ is consistent with a thrombosed hemorrhoid entering its resolving phase. (Textbook of Family Medicine 9e, p. 573-575)
2. Recurrent Perianal Abscess via Fistula Tract (Must be ruled out given your history)
Your 3-year history of fistula-in-ano with pus collection is a major red flag. From Roberts & Hedges' Clinical Procedures in Emergency Medicine:
"A fistula-in-ano is usually formed after partial resolution of a perianal abscess, and its presence is suggested by recurrence of these abscesses with intermittent drainage."
The textbook also notes: "Recurrence is the most common complication after I&D of a perianal abscess. The most common cause of recurrence is an unrecognized, and therefore untreated, associated fistula."
If the fistula tract was never definitively treated (fistulotomy/fistulectomy), pus can re-accumulate along the same or adjacent tract. A tense, non-tender swelling can be an early/subacute abscess, especially in someone with a pre-existing tract.
Classification of Perirectal Abscesses (for context)
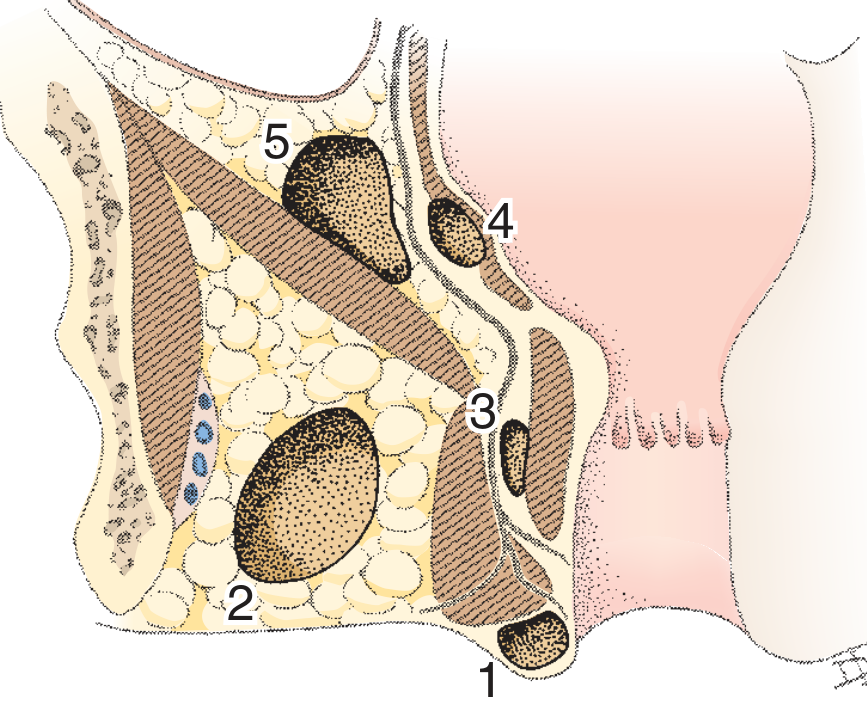
Classification of perirectal abscesses: 1 = Perianal, 2 = Ischiorectal, 3 = Intersphincteric, 4 = High intramuscular, 5 = Pelvirectal - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Given your history, the most likely type would be a perianal (type 1) recurrence.
How to Differentiate
| Feature | Thrombosed Hemorrhoid | Recurrent Abscess |
|---|---|---|
| Color | Purplish-blue | Erythematous (red), skin-colored |
| Tenderness | Initially high, then decreasing | Persistent or increasing |
| Fever/chills | Absent | May be present |
| Surface | Smooth, tense | May show fluctuance later |
| Prior fistula history | Unrelated | Strongly suggestive |
| Location | External, below dentate line | Can be same site as old tract |
What You Should Do - Urgently
You need an in-person surgical/colorectal evaluation. The key reasons:
-
Your fistula history changes everything. Even if this looks like a thrombosed hemorrhoid, an undetected recurrent abscess in someone with a known fistula tract can progress to Fournier's gangrene (necrotizing soft tissue infection) - a life-threatening emergency.
-
MRI or transanal ultrasound may be needed to map any residual or new fistula tract before treatment decisions are made.
-
If this is a thrombosed hemorrhoid within 72 hours of onset, surgical excision (not simple incision) gives the best outcome - lower recurrence, faster resolution. If you are beyond 72 hours and symptoms are improving, conservative management is acceptable:
- Sitz baths 2-3 times/day
- Stool softeners
- Topical anesthetic ointment (e.g., lidocaine 5%)
- Oral analgesics (NSAIDs)
- High-fiber diet and adequate hydration
-
If there is any fluctuance, increasing tension, fever, or return of severe pain, go to an emergency department immediately - abscess drainage cannot be delayed.
Bottom Line
Given the combination of a tense non-tender perianal swelling + prior fistula-in-ano history, this presentation requires colorectal surgical assessment within 24-48 hours to distinguish between a resolving thrombosed hemorrhoid and a recurrent abscess/fistula. Do not manage this purely conservatively at home given your history. The absence of tenderness does not rule out an abscess - deeper or early abscesses can present with minimal tenderness initially.
Disclaimer: This is clinical information for educational purposes. It is not a substitute for an in-person examination. Please see a surgeon or visit an emergency department promptly.
This is a shared conversation. Sign in to Orris to start your own chat.