Shock
Reading File
Finding Sources
Searching PubMed
"shock" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full, detailed answer on Shock.
Shock
Shock is a state of circulatory failure in which inadequate tissue perfusion leads to cellular hypoxia. At the outset the cellular injury is reversible, but prolonged shock leads to irreversible tissue injury and death.
Definition
"Shock is a state in which diminished cardiac output or reduced effective circulating blood volume impairs tissue perfusion and leads to cellular hypoxia."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
"Shock is a progressive disorder that leads to death if the underlying problems are not corrected."
- Robbins & Kumar Basic Pathology
Types of Shock
| Type | Clinical Examples | Core Mechanism |
|---|---|---|
| Cardiogenic | MI, ventricular arrhythmia, cardiac tamponade, pulmonary embolism | Failure of myocardial pump - intrinsic damage, extrinsic compression, or outflow obstruction |
| Hypovolemic | Hemorrhage, severe burns, vomiting, diarrhea, trauma | Inadequate blood or plasma volume leading to low cardiac output |
| Septic / Distributive | Gram-positive/gram-negative bacteremia, fungal sepsis | Activation of cytokine cascades, peripheral vasodilation, endothelial injury, DIC |
| Neurogenic | Spinal cord injury, deep anesthesia | Loss of sympathetic vascular tone causing acute vasodilation |
| Anaphylactic | IgE-mediated hypersensitivity reactions | Systemic vasodilation and increased vascular permeability |
Stages of Shock
Shock evolves through three progressive stages, best characterized in hypovolemic shock but applicable to all forms:
Stage 1 - Nonprogressive (Compensated) Phase
The body activates neurohumoral compensatory mechanisms to maintain perfusion:
- Baroreceptor reflexes detect hypotension
- Catecholamine release (epinephrine, norepinephrine) causes tachycardia and peripheral vasoconstriction
- ADH release conserves water via the kidneys
- RAAS activation (renin-angiotensin-aldosterone) conserves Na+ and water
- Selective vasoconstriction shunts blood from skin/muscle to heart and brain
- Clinical signs: cool, pale, clammy skin; tachycardia; oliguria
Note: In septic shock, early-stage cutaneous vasodilation occurs instead, giving warm, flushed skin.
Stage 2 - Progressive (Decompensated) Phase
Compensatory mechanisms are overwhelmed:
- Persistent oxygen deficit forces cells into anaerobic glycolysis, producing lactic acid
- Metabolic lactic acidosis blunts vasomotor response; arterioles dilate
- Blood pools in the microcirculation - worsening cardiac output
- Endothelial ischemia leads to DIC (disseminated intravascular coagulation)
- Vital organs begin to fail
Stage 3 - Irreversible Phase
- Lysosomal enzyme leakage causes widespread cell death
- Myocardial contractility worsens (partly via increased NO synthesis)
- Ischemic bowel allows intestinal flora to enter circulation (superimposed bacteremic shock)
- Acute tubular necrosis and renal failure develop
- Despite therapy, death follows multiorgan failure
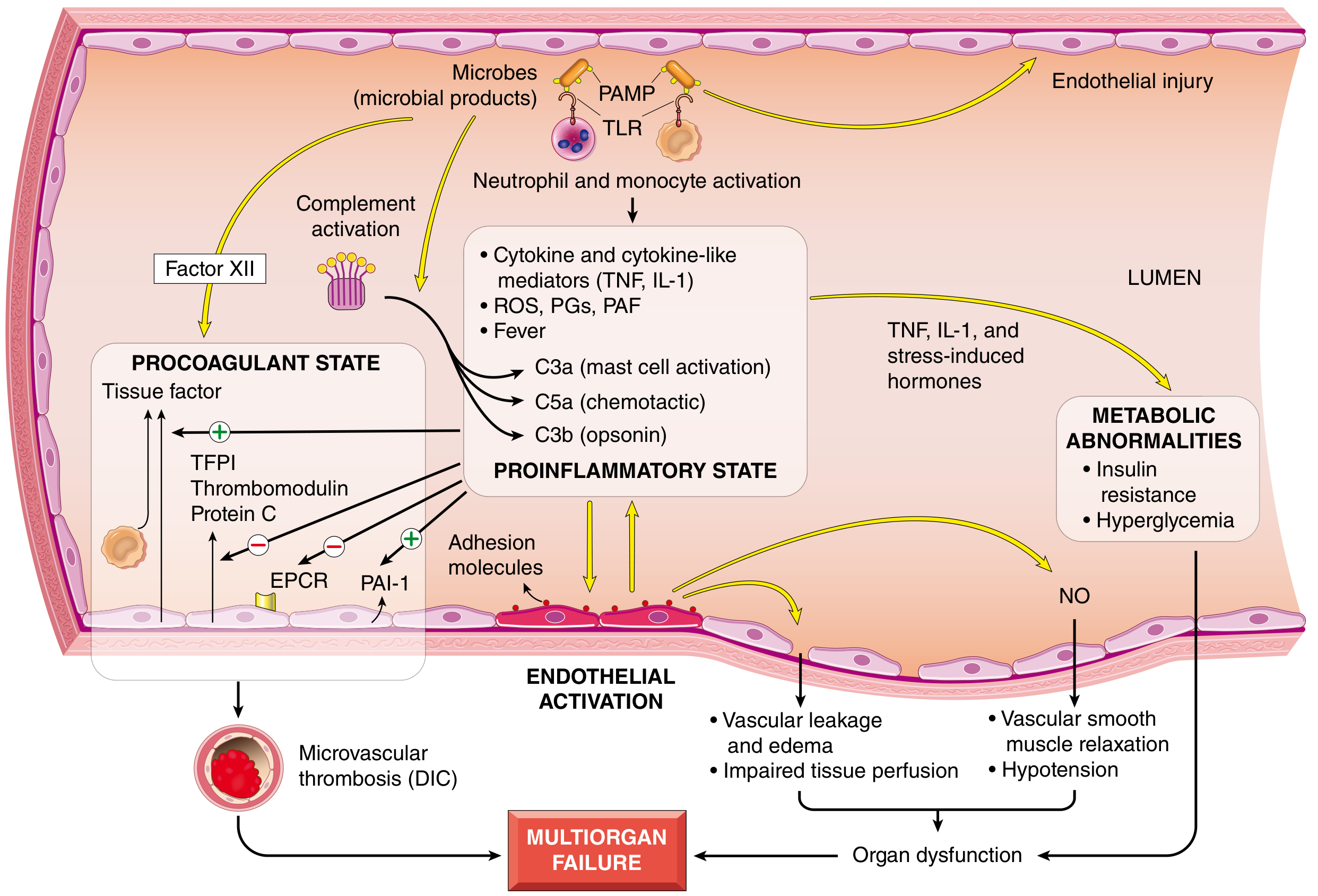
Pathogenesis of Septic Shock (Most Complex Mechanism)
Septic shock accounts for >750,000 US hospital admissions per year with a mortality rate of 20-40%. Most commonly triggered by gram-positive bacteria, then gram-negative bacteria, then fungi.
Microbial Triggers
Microbial products (PAMPs - pathogen-associated molecular patterns) and host-derived damage signals (DAMPs) activate innate immune receptors:
- Toll-like receptors (TLRs) - recognize LPS, peptidoglycans, flagellin
- G-protein-coupled receptors - detect bacterial peptides
- C-type lectin receptors (Dectins) - recognize fungal components
Resulting Cascades
- Proinflammatory cytokines: TNF, IL-1, IL-12, IL-18, IFN-γ, HMGB1 - activate endothelium and amplify inflammation
- Reactive oxygen species (ROS) and lipid mediators: prostaglandins, platelet-activating factor (PAF)
- Complement activation (C3a, C5a, C3b) via microbial components and plasmin
- Coagulation activation: Factor XII directly; altered endothelial function indirectly - leading to DIC
- Nitric oxide (NO) production causes vascular smooth muscle relaxation and hypotension
- Endothelial injury: vascular leakage, edema, impaired perfusion
- Metabolic abnormalities: insulin resistance, hyperglycemia via TNF, IL-1, stress hormones
The host also mounts counter-regulatory immunosuppression (Th1 to Th2 shift, IL-10, lymphocyte apoptosis), causing patients to oscillate between hyperinflammatory and immunosuppressed states.
Morphology (Organ Effects)
The cellular effects of shock are essentially those of hypoxic injury, caused by hypoperfusion and microvascular thrombosis. Organs most affected:
| Organ | Finding |
|---|---|
| Kidneys | Fibrin thrombi in glomeruli; acute tubular necrosis |
| Adrenals | Cortical cell lipid depletion (increased use for steroid synthesis) |
| Lungs | Resistant in simple hypovolemia, but sepsis/trauma causes diffuse alveolar damage ("shock lung" / ARDS) |
| Brain | Neuronal loss (irreversible) |
| Heart | Cardiomyocyte loss (irreversible); contraction band necrosis |
| GI tract | Ischemic enteritis; bacterial translocation |
Except for neuronal and cardiomyocyte loss, tissues can recover completely if the patient survives.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Clinical Features
| Feature | Hypovolemic / Cardiogenic | Septic (early) |
|---|---|---|
| Skin | Cool, clammy, cyanotic | Warm, flushed |
| Pulse | Weak, rapid | Bounding initially |
| BP | Low | Low |
| Mental status | Altered | Altered |
| Urine output | Reduced (oliguria) | Reduced |
| Lactic acid | Elevated | Elevated |
Initial Management (Harrison's Principles, 22e)
The key principle is to initiate treatment simultaneously with diagnosis - do not delay resuscitation while awaiting the full workup.
Access and Monitoring
- Two large-bore peripheral IVs (16-18 gauge) immediately
- Central venous catheter (CVC) for vasopressors, CVP monitoring, ScvO2 assessment if hypotension persists despite fluids
- Arterial line for continuous MAP, pulse pressure variation (volume responsiveness), and repeated lactate/blood gas
- Urinary catheter for hourly urine output tracking
Volume Resuscitation
- Goal: move patient to the non-preload-dependent portion of the Starling curve
- For septic shock: minimum 30 mL/kg IV crystalloid (Surviving Sepsis Campaign recommendation)
- Even some cardiogenic shock patients may benefit from cautious volume - assess first
- Isotonic crystalloids (normal saline, lactated Ringer's) are first-line
Vasopressors and Inotropes
- Indicated when hypotension persists despite adequate volume resuscitation
- Norepinephrine - first-line vasopressor for septic/distributive shock
- Dopamine - alternative (more arrhythmogenic)
- Vasopressin - adjunct for refractory septic shock
- Inotropes (dobutamine) - for cardiogenic shock with low cardiac output
Type-Specific Interventions
| Shock Type | Specific Treatment |
|---|---|
| Septic | Early broad-spectrum antibiotics (within 1 hour), source control |
| Hemorrhagic/Hypovolemic | Hemorrhage control, blood products (1:1:1 ratio - PRBC:FFP:platelets), damage control surgery |
| Cardiogenic | Reperfusion (PCI/thrombolysis for MI), IABP, mechanical support |
| Obstructive | Pericardiocentesis (tamponade), needle decompression/chest tube (tension pneumothorax), anticoagulation (PE) |
| Anaphylactic | Epinephrine IM (first-line), antihistamines, steroids, IV fluids |
Monitoring Goals
- MAP > 65 mmHg
- Urine output > 0.5 mL/kg/hr
- Lactate clearance (target normalization)
- ScvO2 > 70%
Key Summary Points (Robbins)
- Shock = systemic tissue hypoperfusion from reduced CO and/or reduced effective circulating volume
- Three major types: cardiogenic, hypovolemic, septic
- Progresses through compensated, decompensated, and irreversible stages
- Septic shock: dysregulated host response to infection with endothelial activation, vasodilation, edema, DIC, metabolic derangements, organ failure
- Shock of any form leads to hypoxic tissue injury if not corrected
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 134-136
- Robbins & Kumar Basic Pathology, pp. 133-136
- Harrison's Principles of Internal Medicine 22e (2025), Chapter 314
- Sabiston Textbook of Surgery, Chapter on Shock, pp. 563-566
- Goldman-Cecil Medicine, Chapter 94
Recent evidence note: The Surviving Sepsis Campaign 2026 Pediatric Guidelines (PMID 41869844) and a 2024 JAMA meta-analysis on beta-lactam infusion in septic shock (PMID 38864162) support prolonged infusion of beta-lactam antibiotics in adults with sepsis or septic shock for improved pharmacodynamic target attainment - consistent with current Surviving Sepsis Campaign guidance.
This is a shared conversation. Sign in to Orris to start your own chat.