Rupture of tendon physiotherapy assessment and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tendon rupture" AND "physiotherapy" AND "rehabilitation"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive clinical guide on tendon rupture - physiotherapy assessment and management.
Tendon Rupture: Physiotherapy Assessment and Management
1. Overview and Pathophysiology
Tendon ruptures can be complete (full transection) or partial. They most commonly occur in the setting of underlying tendinosis - a degenerative process predisposing the tendon to failure under load. Associated risk factors include:
- Diabetes mellitus, chronic renal failure, rheumatoid arthritis, gout, SLE, hyperparathyroidism
- Corticosteroid injections or systemic steroid use
- Fluoroquinolone antibiotic therapy (e.g., ciprofloxacin)
- Smoking (strongly associated with distal biceps rupture)
- Being a middle-aged male during sporting activity
Up to 20-25% of acute tendon ruptures are initially missed due to retained function through accessory muscles. - ROSEN's Emergency Medicine, 9th Ed.
2. Common Tendon Ruptures by Site
A. Achilles Tendon Rupture
The most frequently encountered tendon rupture in clinical practice.
Mechanism: Sudden forced dorsiflexion, push-off with simultaneous knee extension and calf contraction (e.g., badminton, squash, sprinting). The classic history is a sensation of being "kicked in the heel" with an audible pop.
Assessment:
| Finding | Details |
|---|---|
| Symptom onset | Sudden posterior ankle pain, pop/snap |
| Palpable defect | 2-6 cm proximal to calcaneal insertion |
| Plantar flexion | Weak but may be preserved via tibialis posterior, toe flexors, peroneals (leading to misdiagnosis) |
| Thompson Test (Simmonds Squeeze Test) | Patient prone, knee at 90°, feet hanging off couch - squeeze calf. Absence of passive plantarflexion = positive. Most reliable test. |
| Matles test | Knee flexion from prone - foot falls into neutral/dorsiflexion on affected side |
Imaging: Diagnosis is primarily clinical. Ultrasound or MRI used when diagnostic uncertainty exists. Lateral X-ray may show opacification of Kager's triangle or tendon irregularity. - Campbell's Operative Orthopaedics, 15th Ed 2026
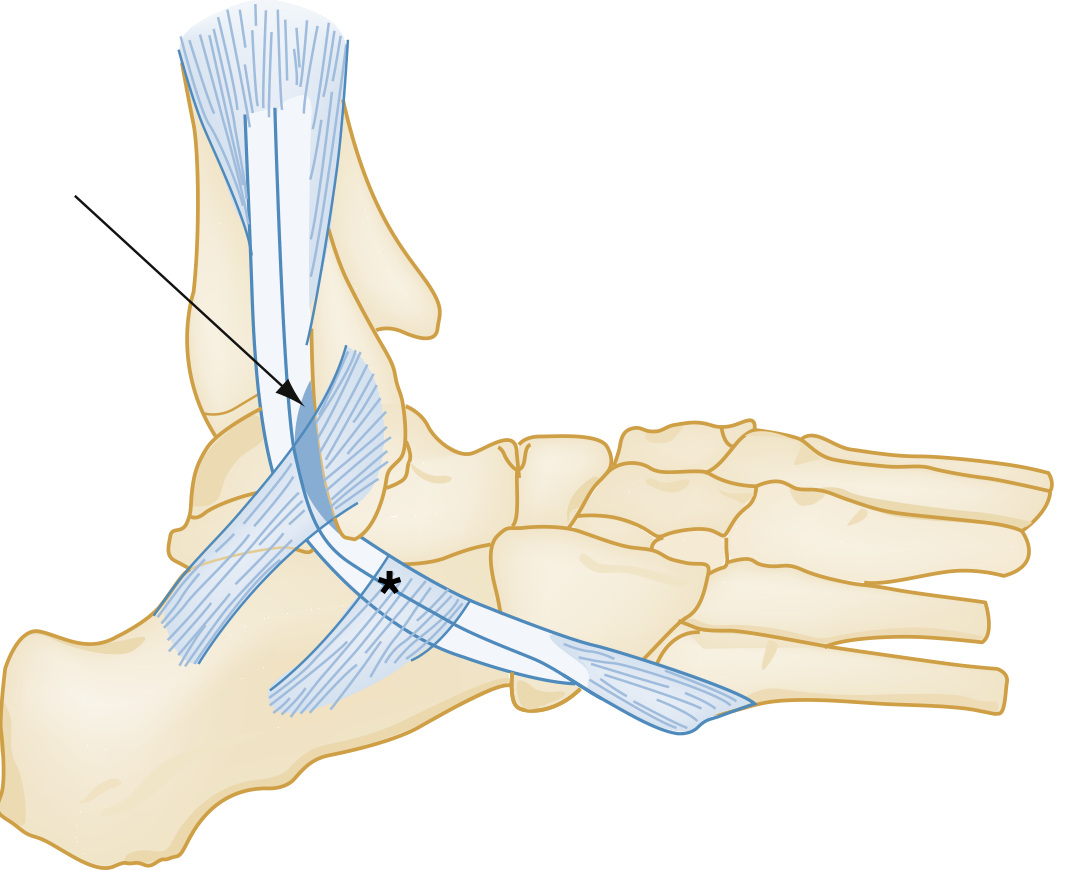
Ankle tendon anatomy - superior (arrow) and inferior peroneal retinaculum (star) in relation to the fibula and peroneal tendons. - ROSEN's Emergency Medicine
B. Quadriceps and Patellar Tendon Rupture
Quadriceps tendon: Age >40, often degenerative background; rupture from forceful eccentric quadriceps contraction or fall on flexed knee.
Patellar tendon: Age <40; history of patellar tendinitis or steroid use increases risk.
Assessment:
| Finding | Quadriceps rupture | Patellar tendon rupture |
|---|---|---|
| Location of defect | Proximal to patella | Distal to patella |
| Patellar position | Patella baja (lowered) | Patella alta (elevated) on lateral X-ray |
| Key sign | Unable to perform straight leg raise | Unable to actively extend knee or maintain extension against gravity |
| Functional loss | Cannot extend knee actively | Same |
Imaging: Point-of-care ultrasound (high-frequency linear transducer) can visualize the rupture. Lateral radiograph shows patella alta in patellar tendon rupture. - Tintinalli's Emergency Medicine

Quadriceps tendon rupture: note the defect above the patella and the prominence of the proximal edge of the patella. - Tintinalli's Emergency Medicine
C. Biceps Tendon Rupture
Proximal (long head): Most common; middle-aged athletes/laborers. Snapping sound + anterior shoulder pain with strenuous activity. Produces "Popeye deformity" - visible muscle belly bunching distally. Flexion remains intact via short head.
Distal (radial tuberosity): Almost exclusively men aged 40-60; dominant arm; inciting event is unexpected extension force on 90°-flexed elbow. Results in weakness of flexion and especially supination.
Assessment:
- Speed's test and Yergason's test: Poor sensitivity/specificity - use in context only
- MRI: Useful when partial rupture is suspected - not urgent in ED
Management note: All patients require orthopedic referral within 72 hours for early anatomic repair consideration. - ROSEN's Emergency Medicine
D. Other Ankle Tendons (Peroneal, Tibialis Posterior, Tibialis Anterior)
| Tendon | Mechanism | Key Clinical Sign | Management |
|---|---|---|---|
| Peroneal longus/brevis | Forced dorsiflexion with inversion | Lateral malleolus pain, weakness of eversion, snapping with eversion | PRICE + physio for tendinopathy; ortho for rupture |
| Tibialis posterior | Forced eversion | Medial ankle pain, flat foot (pes planus), inability to perform single leg heel raise | PRICE + physio; ortho for rupture |
| Tibialis anterior | Laceration > acute rupture | Anterior mass from retraction; compensatory recruitment of EDL/EHL | Ortho referral; PRICE + physio for incomplete |
- ROSEN's Emergency Medicine, Table 49.2
3. Physiotherapy Management by Phase
The core principle is: Protect → Mobilize → Strengthen → Return to Function
Phase 1: Acute/Protective Phase (0-2 weeks)
- Posterior slab/splint in plantar flexion (Achilles) or extension (knee tendons)
- Non-weight bearing with crutches
- Goal: protect healing tissue, control swelling
- Modalities: ice, compression, elevation (PRICE)
- No ankle ROM exercises yet
Phase 2: Early Mobilization (2-4 weeks)
- Aircast/walking boot with 2 cm heel lift (Achilles)
- Protected weight bearing with crutches
- Active plantar flexion and dorsiflexion to neutral; inversion/eversion below neutral
- Modalities to control swelling (ultrasound, ice, elevation)
- Incision mobilization (scar massage, friction, ultrasound) - if scar is tight
- Hip and knee exercises without ankle involvement: leg lifts (sitting, prone, side-lying)
- Non-weight-bearing cardiovascular exercise: single-leg cycling, deep-water running, hydrotherapy
Phase 3: Progressive Loading (4-8 weeks)
- Weight bearing as tolerated by 4-6 weeks
- Remove heel lift from boot at 6-8 weeks
- Graduated resistance exercises - open and closed kinetic chain
- Dorsiflexion stretching (slowly graduated)
- Functional activities introduction
- Proprioceptive training
- Gait retraining
- Hydrotherapy continues
Phase 4: Strengthening and Return to Activity (8-12 weeks)
- Wean off walking boot; return to crutches/cane as needed then wean
- Progressive range of motion, strength, and proprioception
- Eccentric strengthening exercises (especially for Achilles - e.g., heel drops)
- Balance and neuromuscular control work
- Increase dynamic weight-bearing exercise
Phase 5: Sport-Specific and Plyometric Training (>12 weeks)
- Retrain strength, power, and endurance
- Plyometric training (jumping, landing mechanics)
- Sport-specific drills
- Return to sport typically 3-6 months post-operative (AAOS guideline, Moderate strength)
- Campbell's Operative Orthopaedics, 15th Ed 2026 (Table 53.2, AAOS Protocol)
4. AAOS Clinical Practice Guideline Summary (Achilles Tendon Rupture)
| Recommendation | Strength |
|---|---|
| Physical exam with 2+ clinical tests to establish diagnosis | Consensus |
| Early (≤2 weeks) postoperative protected weight bearing limiting dorsiflexion | Moderate |
| Protective device allowing mobilization by 2-4 weeks postoperatively | Moderate |
| Nonoperative treatment as an option | Weak |
| Return to sport within 3-6 months post-operative | Weak |
| Postoperative physiotherapy | Inconclusive (evidence insufficient, not that it lacks benefit) |
- Campbell's Operative Orthopaedics, 15th Ed 2026
5. Conservative vs. Surgical Decision Framework
| Factor | Favor Conservative | Favor Surgical |
|---|---|---|
| Patient age/activity | Older, sedentary | Young, active athlete |
| Rerupture risk tolerance | Accepts higher risk (~6%) | Wants lower risk (~0.6%) |
| Comorbidities | Diabetes, immunocompromised, PVD, BMI >30, smoking | None of these |
| Wound complications | Higher concern | Lower concern |
| Early mobilization | Both approaches benefit from it equally | Both approaches benefit from it equally |
Key point: Regardless of operative vs. non-operative management, early mobilization improves functional recovery without increasing rerupture rates. - ROSEN's Emergency Medicine
For complete quadriceps or patellar tendon tears, surgical repair is the treatment of choice. Incomplete tears with an intact extensor mechanism can be treated conservatively with immobilization and close follow-up. - Tintinalli's Emergency Medicine
6. Outcome Considerations
- 30-50% of patients have functional impairments (pain, reduced strength, decreased ROM) at 1-5 years post-injury regardless of treatment approach
- Patient-reported outcomes are relatively high, suggesting adaptation to residual impairment
- In high-level athletes, only 64-69% return to play after operative treatment
- By 2 years, most athletes who return perform at a level comparable to uninjured controls
- Achilles rerupture after nonoperative treatment necessitates surgical repair
- Campbell's Operative Orthopaedics, 15th Ed 2026
7. Red Flags and Missed Diagnoses
- Retained plantar flexion (via accessory muscles) leads to 20-25% misdiagnosis of complete Achilles rupture as ankle sprain or partial tear
- An intact plantaris may produce a false-negative Thompson test
- Patella alta on X-ray is a key clue to patellar tendon rupture
- Delayed presentations show less palpable gap due to haematoma/oedema - use imaging to confirm
Key References: Campbell's Operative Orthopaedics 15th Ed 2026 | ROSEN's Emergency Medicine 9th Ed | Tintinalli's Emergency Medicine | Bailey and Love's Surgery 28th Ed
This is a shared conversation. Sign in to Orris to start your own chat.