Pathogenesis of cholera
Reading File
Finding Sources
Finding Sources
Searching PubMed
cholera pathogenesis Vibrio cholerae
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the full answer.
Pathogenesis of Cholera
The Organism
Vibrio cholerae is a comma-shaped (curved), flagellated, gram-negative rod that is oxidase-positive and grows best under alkaline conditions (pH 8.0-9.5). Of the >200 O-antigen serogroups, only O1 and O139 cause epidemic cholera. Serogroup O1 is further divided into two biotypes: Classic (responsible for the first six pandemics, now largely extinct) and El Tor (responsible for the current seventh pandemic). V. cholerae O139 resembles El Tor but produces an additional polysaccharide capsule.
- Harrison's Principles of Internal Medicine 22E, p. 1369
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 1247
Step 1 - Ingestion and Gastric Transit
The infectious dose is relatively high, but is markedly reduced in:
- Hypochlorhydric patients
- Those using antacids or proton pump inhibitors
- When gastric acid is buffered by a meal
V. cholerae is acid-sensitive. Organisms that survive the stomach pass into the small intestine, where they must colonize the mucosa to cause disease. - Harrison's, p. 1370
Step 2 - Intestinal Colonization
Colonization depends on two key structures:
-
Toxin-coregulated pilus (TCP) - long filamentous pili that mediate adherence to the intestinal epithelium. TCP is absolutely essential for V. cholerae to survive and multiply in the small intestine. TCP expression is regulated coordinately with cholera toxin production.
-
Flagellar proteins - required for motility and efficient penetration of the intestinal mucus layer to reach the epithelial surface.
A secreted metalloproteinase with hemagglutinin activity is also important for shedding organisms in the stool (completing the transmission cycle).
The organism does NOT invade the mucosa. It remains in the lumen and on the mucosal surface.
- Harrison's, p. 1370
- Robbins & Kumar Basic Pathology, p. 449
- Sherris, p. 1247
Step 3 - Virulence Gene Regulation
Production of cholera toxin, TCP, and other virulence factors is coordinately regulated by the transcriptional activator ToxR. ToxR modulates virulence gene expression in response to environmental signals (temperature, osmolarity, pH) via a cascade of regulatory proteins including ToxT.
Quorum sensing (bacterial population density signaling) also modulates virulence gene expression as the bacterial load builds up in the intestinal lumen.
The genes encoding cholera toxin (ctxAB) are part of the genome of a lysogenic bacteriophage, CTXΦ. The receptor for this phage on the V. cholerae surface is TCP itself. This means TCP serves a dual role: colonization factor AND receptor for the toxin-encoding phage. Horizontal transfer of CTXΦ accounts for the emergence of new toxigenic strains. Many other virulence genes (TCP biosynthesis, accessory colonization factors, regulators) are clustered in the V. cholerae Pathogenicity Island, acquired by horizontal gene transfer.
- Harrison's, p. 1370
Step 4 - Cholera Toxin (CT) Structure
Cholera toxin is an A-B type toxin:
| Subunit | Number | Function |
|---|---|---|
| B subunits | 5 (pentamer) | Bind to GM1-ganglioside receptors on the surface of intestinal epithelial cells |
| A subunit (A1 + A2) | 1 (monomer) | Enzymatically active component; A1 is the toxic moiety |
The B pentamer anchors the toxin to the enterocyte surface via GM1-ganglioside. This delivers the A subunit to its intracellular target.
- Sherris, p. 1247
- Robbins Pathology, p. 449
Step 5 - Molecular Mechanism of Action
Here is the key signaling cascade:
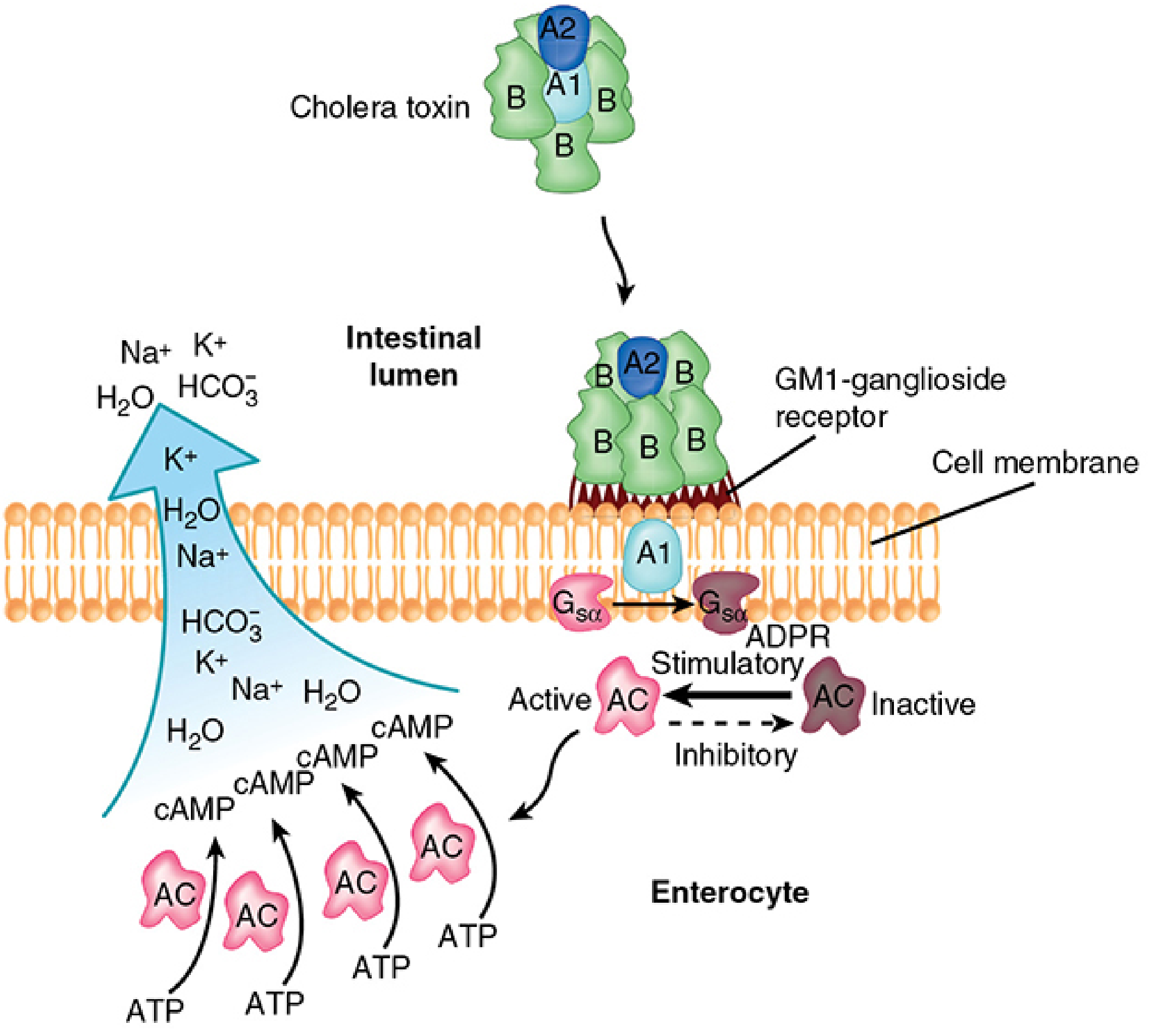
- B subunit binding: The B pentamer binds to GM1-ganglioside on the luminal surface of enterocytes.
- A subunit internalization: The disulfide bond between A1 and A2 is reduced; the A1 fragment is released and translocated into the cytosol (via the endoplasmic reticulum).
- ADP-ribosylation of Gsα: The A1 subunit catalyzes ADP-ribosylation of Gsα (the stimulatory G protein that regulates adenylate cyclase). This modification locks Gsα in its active state, preventing it from hydrolyzing GTP back to GDP - the normal "off switch."
- Persistent adenylate cyclase activation: ADP-ribosylated Gsα constitutively activates adenylate cyclase, which continuously converts ATP → cyclic AMP (cAMP).
- cAMP accumulation: Intracellular cAMP rises to very high levels, activating protein kinase A and the cystic fibrosis transmembrane conductance regulator (CFTR).
- Harrison's, p. 1370
- Sherris, p. 1247-1248
- Robbins & Kumar Basic Pathology, p. 449
Step 6 - Net Effect on Ion Transport (The Diarrhea)
The massive rise in cAMP has two simultaneous effects on intestinal epithelial cells:
| Cell Type | Normal Action | Effect of High cAMP |
|---|---|---|
| Villus cells | Absorb Na+ (and water) | Absorption INHIBITED |
| Crypt cells | Normally minimal secretion | Cl- secretion ACTIVATED (via CFTR) |
- Cl- pours into the intestinal lumen.
- Na+, K+, and HCO3- follow the electrochemical gradient.
- Water follows passively to maintain osmolality.
- The result is massive isotonic fluid accumulation in the intestinal lumen - secretory diarrhea.
When the volume exceeds the resorptive capacity of the colon and the rest of the gut, profuse watery diarrhea results - up to 1 liter per hour in severe cases.
Cholera toxin also enhances intestinal secretion secondarily via prostaglandins and neural/histamine receptors, amplifying the secretory signal.
- Harrison's, p. 1370
- Robbins & Kumar Basic Pathology, p. 449
Key Histopathological Point
Despite the catastrophic fluid loss, mucosal biopsy specimens show only minimal morphological alterations. There is:
- No mucosal invasion
- No significant inflammation
- No fever (in most cases)
- No ulceration or tissue destruction
This is purely a toxin-mediated secretory process. V. cholerae acts entirely from the intestinal lumen.
- Robbins & Kumar Basic Pathology, p. 449
- Sherris, p. 762
Summary Flowchart
Ingestion of V. cholerae (contaminated water/food)
↓
Survival through stomach (aided by achlorhydria, food buffering)
↓
Flagellar motility → penetrates mucus → reaches small intestinal epithelium
↓
TCP (toxin-coregulated pilus) → adherence/colonization
↓
ToxR/ToxT regulatory cascade → virulence gene activation
↓
Cholera toxin secreted into intestinal lumen
↓
B pentamer → GM1-ganglioside receptor binding
↓
A1 subunit enters cytosol → ADP-ribosylates Gsα
↓
Gsα locked in ON state → adenylate cyclase permanently active
↓
Massive intracellular cAMP accumulation → CFTR activation
↓
↓ Villus Na+ absorption + ↑ Crypt Cl- secretion → Na+, K+, HCO3-, H2O into lumen
↓
Profuse isotonic "rice-water" diarrhea (up to 1 L/hr)
↓
Dehydration → hypovolemic shock → metabolic acidosis (HCO3- loss) → death
Why ORS Works
The hexose-Na+ co-transport system (SGLT1) in villus cells remains intact even when cholera toxin is active. Oral rehydration solution (ORS) exploits this by pairing glucose with Na+, allowing Na+ (and water) absorption to continue via this toxin-independent pathway, compensating for the secretory losses.
- Harrison's, p. 1370
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 173
- Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter on GI infections
- Sherris & Ryan's Medical Microbiology, 8th Ed., Chapter 32
- Goldman-Cecil Medicine, Chapter 278
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full, detailed answer.
Parasites Infecting the GIT - Classification & Hookworm Infections
Classification of Parasites Infecting the GIT
GIT parasites are broadly divided into:
A. Protozoa
| Group | Organism | Disease |
|---|---|---|
| Amoeba | Entamoeba histolytica | Amoebiasis, amoebic dysentery |
| Flagellates | Giardia lamblia | Giardiasis |
| Flagellates | Trichomonas hominis | Diarrhea |
| Coccidia | Cryptosporidium parvum | Cryptosporidiosis |
| Coccidia | Cyclospora cayetanensis | Cyclosporiasis |
| Coccidia | Isospora belli | Isosporiasis |
| Microsporidia | Enterocytozoon bieneusi | Diarrhea (immunocompromised) |
| Ciliates | Balantidium coli | Balantidiasis |
B. Helminths
1. Nematodes (Roundworms)
| Organism | Common Name |
|---|---|
| Ascaris lumbricoides | Roundworm |
| Necator americanus / Ancylostoma duodenale | Hookworm |
| Strongyloides stercoralis | Threadworm |
| Trichuris trichiura | Whipworm |
| Enterobius vermicularis | Pinworm / Threadworm |
| Trichinella spiralis | Trichinellosis |
2. Trematodes (Flukes)
| Organism | Common Name |
|---|---|
| Fasciolopsis buski | Intestinal fluke |
| Fasciola hepatica | Liver fluke |
| Schistosoma mansoni / japonicum | Blood fluke (GI involvement) |
3. Cestodes (Tapeworms)
| Organism | Common Name |
|---|---|
| Taenia saginata | Beef tapeworm |
| Taenia solium | Pork tapeworm |
| Hymenolepis nana | Dwarf tapeworm |
| Diphyllobothrium latum | Fish tapeworm |
The Clinical Case Explained
The presented case - Fever, Abdominal Pain, Iron Deficiency Anaemia, Rash on Leg, Diarrhoea with stool microscopy showing segmented ovum - is classic for Hookworm Infection.
The segmented (cleaved, with visible blastomeres) oval egg on stool microscopy is the hallmark diagnostic finding. This distinguishes it from Ascaris (unsegmented, rough mamillated coat) and Trichuris (barrel-shaped with polar plugs).
Hookworm Infections - Full Discussion
The Pathogens
Three species cause human hookworm infection:
- Necator americanus - predominant worldwide (tropics, subtropics); cutting plates; ~10,000 eggs/day/female; survives 2-5 years
- Ancylostoma duodenale - North Africa, Middle East, northern India; buccal teeth; ~28,000 eggs/day/female; survives ~1 year
- Ancylostoma ceylanicum - mainly Southeast Asia; less common
Zoonotic species (A. caninum, A. braziliense) cause cutaneous larva migrans but do NOT complete their life cycle in humans.
- Harrison's Principles of Internal Medicine 22E, p. 2020
- Goldman-Cecil Medicine, p. 3477
Life Cycle
Eggs passed in feces onto warm, moist soil (23-33°C)
↓ (1 week)
Rhabditiform (non-infective) larvae hatch
↓
Filariform (infective, L3) larvae develop in soil
↓
SKIN PENETRATION (usually feet/legs)
↓
Enter venous circulation → Heart → Lungs
↓
Penetrate alveolar walls → ascend bronchial tree → Larynx
↓
SWALLOWED → reach small intestine
↓
Mature to adult worms (takes 5-9 weeks; prepatent period ~6-8 weeks)
↓
Adults attach to small bowel mucosa
A. duodenale → buccal TEETH
N. americanus → CUTTING PLATES
↓
Secrete enzymes → invade submucosa → ingest blood + villous tissue
↓
Female produces eggs → passed in feces → cycle repeats
Key alternative route: A. duodenale larvae can also be ingested orally and develop directly into adult worms in the intestine (no lung migration). This is also how Wakana syndrome occurs.
- Harrison's 22E, p. 2022
- Goldman-Cecil, p. 3477
Pathogenesis
1. At the Skin
- Filariform larvae penetrate intact skin, producing a hypersensitivity "ground itch" reaction
- Pruritic, erythematous, maculopapular rash - most common between the toes/ankles
2. Larval Migration (Loeffler-like Syndrome)
- Larvae pass through the lungs, causing mild transient pneumonitis
- Dry cough, wheezing, low-grade fever - less severe than in Ascaris
3. In the Intestine - The Key Pathology
Adult worms cause disease by:
- Attaching to small bowel mucosa using cutting teeth (Ancylostoma) or cutting plates (Necator)
- Secreting enzymes that allow invasion of submucosal tissues
- Ingesting blood and villous tissue
- Hemoglobinases within the worm's digestive canal degrade host hemoglobin for nutrition
Blood loss per worm per day:
- A. duodenale: 0.15-0.26 mL/day (higher blood sucker)
- N. americanus: 0.03-0.10 mL/day
Additional blood loss occurs when worms migrate to new attachment sites, leaving bleeding points at old sites. Given adults may survive 2-14 years, cumulative blood loss in heavy infections is substantial.
Result: Iron deficiency anaemia + (in severe infections) hypoproteinaemia/hypoalbuminaemia
The host mounts both humoral and immediate hypersensitivity responses, but these do not effectively control the infection. Peripheral and gut eosinophilia is a hallmark.
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 1848
- Goldman-Cecil, p. 3477-3478
- Harrison's 22E, p. 2026
Clinical Features
Stage 1 - Skin Penetration
- "Ground itch" - pruritic, erythematous papular rash at penetration site (feet, ankles, between toes)
- More common with N. americanus
Cutaneous larva migrans (CLM) - caused by zoonotic hookworms (A. caninum, A. braziliense), which penetrate skin but cannot complete life cycle; produce characteristic serpiginous, intensely pruritic, erythematous tracks advancing by mm-cm per day

Stage 2 - Pulmonary (Larval Migration)
- Mild transient pneumonitis: dry cough, sore throat, wheezing, low-grade fever
- Less severe and less frequent than in Ascaris
Stage 3 - Gastrointestinal
- Epigastric pain, abdominal bloating, abnormal peristalsis
- Eosinophilia
- In early intestinal phase: abdominal pain + diarrhoea
Stage 4 - Chronic Infection (Most Significant)
- Iron deficiency anaemia (hypochromic, microcytic) - the hallmark
- Weakness, fatigue, palpitations, dyspnoea, dizziness, lassitude, headache
- In heavy infections: hypoproteinaemia, hypoalbuminaemia, anasarca
- In children: growth retardation, cognitive impairment, cardiac failure, kwashiorkor
- Diarrhoea with occult blood; occasionally frank melena in children
Most light infections are asymptomatic. Disease requires heavy worm burden + prolonged infection + inadequate dietary iron.
- Harrison's 22E, p. 2026
- Goldman-Cecil, p. 3478
- Sherris, p. 1848
Laboratory Diagnosis
1. Stool Microscopy (Gold Standard)
- Characteristic oval eggs, 40 × 60 μm, thin-walled, with segmented/cleaved contents (visible blastomeres - this is the "segmented ovum" in the case)
- Eggs of N. americanus and A. duodenale are morphologically indistinguishable by light microscopy; species identification requires PCR (research tool only)
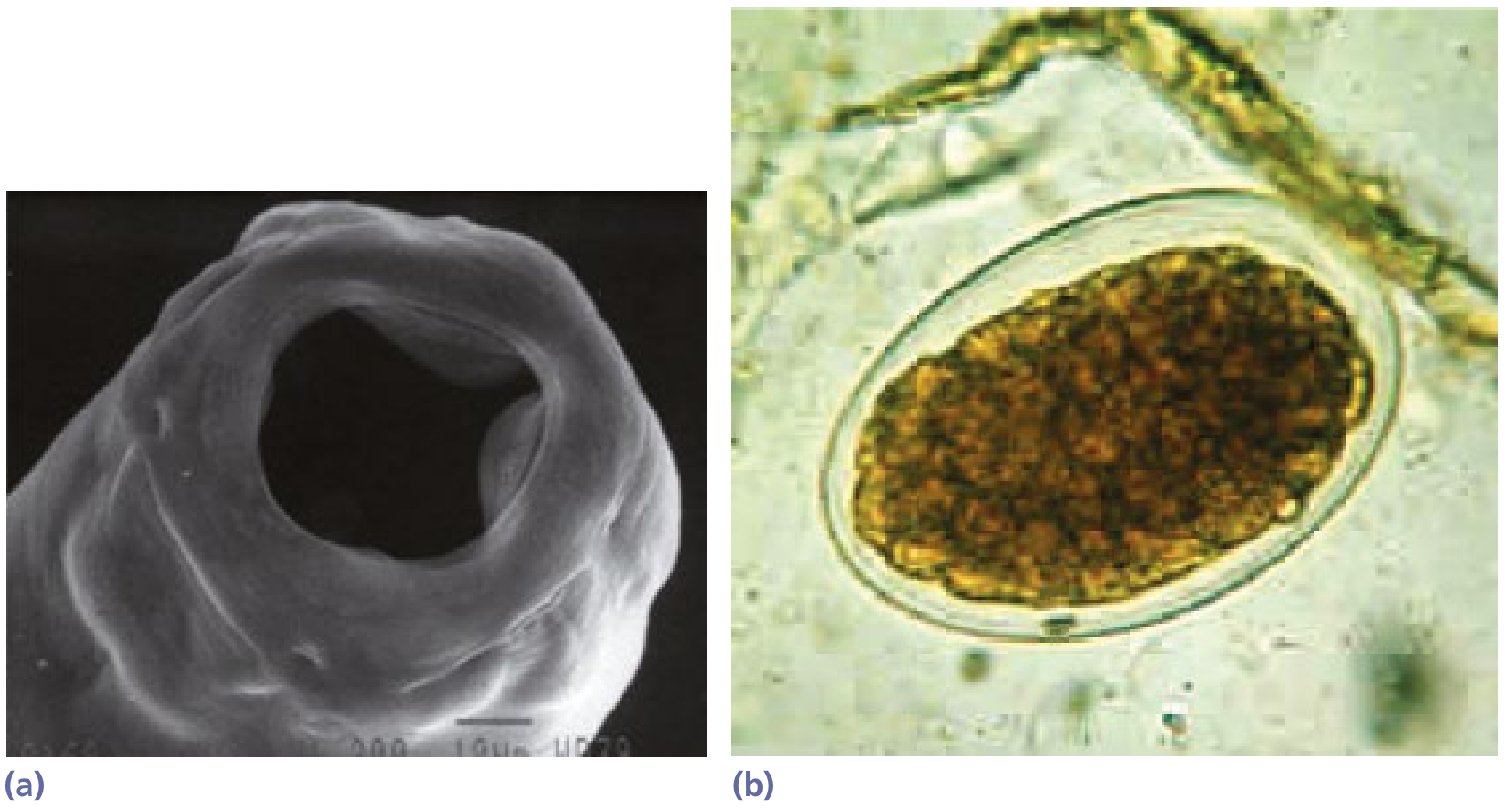
- Important: If stool is not fresh, eggs may hatch to release rhabditiform larvae, which must be differentiated from Strongyloides larvae (S. stercoralis has a short buccal canal; hookworm has a longer buccal canal)
- Stool concentration techniques may be needed for light infections
- Quantitative egg count (Kato-Katz technique) estimates worm burden
2. Blood Tests
- Hypochromic microcytic anaemia (low Hb, low MCV, low MCH)
- Eosinophilia (peripheral blood)
- Hypoalbuminaemia in heavy infections
- Low serum iron, low ferritin, high TIBC
3. PCR
-
Species-specific diagnosis, currently only a research tool
-
Harrison's 22E, p. 2027-2028
-
Sherris, p. 1849
Treatment
Anthelmintic Therapy
| Drug | Dose | Notes |
|---|---|---|
| Albendazole | 400 mg daily × 3 days | First-line (WHO recommended) |
| Mebendazole | 500 mg daily × 3 days OR 100 mg twice daily × 3 days | Alternative |
| Pyrantel pamoate | 11 mg/kg × 3 days (max 1 g/day) | Alternative |
| Tribendimidine | 400 mg once | Alternative |
Note: Growing concern that benzimidazoles (albendazole, mebendazole) are becoming less effective due to emerging resistance. - Harrison's 22E, p. 2037
For Cutaneous Larva Migrans:
- Ivermectin 200 μg/kg daily × 1-2 days (preferred)
- Alternative: Albendazole 400 mg daily × 3 days
Management of Anaemia
- Mild-moderate anaemia: Oral iron supplementation alone is often sufficient
- Severe anaemia with protein loss and malabsorption: Nutritional support + oral iron + deworming
- Very severe anaemia: Blood transfusion may be required
Prevention
-
Improved sanitation and proper disposal of human waste
-
Wearing shoes - key preventive measure (blocks skin penetration)
-
Mass drug administration (albendazole/mebendazole) to at-risk populations in endemic areas
-
Harrison's 22E, p. 2036-2037
-
Goldman-Cecil, Table 327-1
-
Sherris, p. 1849
Key summary for the case: The patient has fever + abdominal pain + iron deficiency anaemia + rash on leg (ground itch / cutaneous migration) + diarrhoea with segmented oval eggs on stool microscopy - all pointing directly to hookworm infection (Necator americanus / Ancylostoma duodenale). Treat with albendazole 400 mg daily × 3 days + oral iron supplementation.
This is a shared conversation. Sign in to Orris to start your own chat.