All the possible questions that can be asked in visual pathway anatomy and physiology in optha
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is a complete, exam-oriented breakdown of every possible question that can be asked on Visual Pathway Anatomy & Physiology in Ophthalmology. The content is drawn from Gray's Anatomy for Students, Goldman-Cecil Medicine, Kanski's Clinical Ophthalmology, Adams & Victor's Neurology, Neuroscience: Exploring the Brain, Localization in Clinical Neurology, and Guyton & Hall.
Visual Pathway - All Possible Exam Questions
The Retinofugal Projection (Base of the pathway)
SECTION 1: ANATOMY OF THE RETINA (Pre-optic nerve)
Q1. What are the layers of the retina in order from vitreous to choroid?
10 layers: Internal limiting membrane → Nerve fiber layer → Ganglion cell layer → Inner plexiform layer → Inner nuclear layer → Outer plexiform layer → Outer nuclear layer → External limiting membrane → Photoreceptor layer (rods & cones) → Retinal pigment epithelium.
Q2. What is the fovea? What is its significance?
The fovea is the central zone of the macula, consisting of ~100,000 slender cones with no rods ("rod-free zone"). It provides maximum visual acuity (central vision). Ganglion cells subserving foveal cones send axons directly to the temporal optic disc as the papillomacular bundle.
Q3. What is the papillomacular bundle?
A dense concentration of axons from foveal ganglion cells that travel directly to the temporal aspect of the optic disc. It is particularly vulnerable in toxic optic neuropathies (e.g., methanol, ethambutol) producing central scotomas.
Q4. What is the blind spot? Why does it exist?
The optic disc (optic nerve head) has no photoreceptors - it is the site where ganglion cell axons coalesce to exit the eye. This creates a physiological scotoma in the nasal visual field of each eye, ~15 degrees temporal to the fovea.
Q5. What is the blood supply of the retina?
- Inner 2/3: Central retinal artery (branch of ophthalmic artery, enters nerve sheath ~1 cm behind globe)
- Outer 1/3 (photoreceptors): Choroidal circulation via posterior ciliary arteries
- ~10% of people: Macular supply via a cilioretinal artery (branch of ciliary system)
- Venous drainage: Central retinal vein
Q6. What are rods and cones? How do they differ?
| Feature | Rods | Cones |
|---|---|---|
| Number | ~120 million | ~6-7 million |
| Location | Peripheral retina | Concentrated at fovea |
| Function | Scotopic (dim light) vision | Photopic (bright light), color, acuity |
| Photopigment | Rhodopsin | 3 types (red/green/blue opsins) |
| Convergence | High (many → 1 ganglion) | Low (1:1 at fovea) |
Q7. What is the mechanism of phototransduction?
Light → Isomerization of 11-cis retinal to all-trans retinal → Activation of opsin → Activation of transducin (G-protein) → Activation of phosphodiesterase → Hydrolysis of cGMP → Closure of Na⁺ channels → Hyperpolarization of photoreceptor → Reduced glutamate release → Signal to bipolar cells.
Q8. What are the cell types in the retina and their roles?
- Photoreceptors (rods, cones): phototransduction
- Bipolar cells: relay to ganglion cells
- Ganglion cells: project to brain (form optic nerve)
- Horizontal cells: lateral inhibition in outer retina
- Amacrine cells: lateral inhibition in inner retina
- Müller cells: principal glial support cells
SECTION 2: OPTIC NERVE
Q9. Describe the segments of the optic nerve.
Four segments:
- Intraocular (optic disc): 1 mm, unmyelinated
- Intraorbital: 25-30 mm, myelinated, surrounded by meninges (dura, arachnoid, pia), covered by oligodendrocytes - making it a CNS structure
- Intracanalicular: 4-10 mm, passes through optic canal in lesser wing of sphenoid
- Intracranial: 10 mm, from optic canal to chiasm
Q10. Why is the optic nerve considered part of the CNS (not a peripheral nerve)?
During embryonic development, optic nerve axons acquire myelin from oligodendrocytes (not Schwann cells) and are covered by cranial meninges. It is embryologically an outgrowth of the diencephalon. This is why multiple sclerosis (a CNS demyelinating disease) can cause optic neuritis, and why the nerve does not regenerate like a peripheral nerve.
Q11. What is the clinical significance of the meningeal sheath of the optic nerve?
The subarachnoid space around the optic nerve is continuous with the intracranial subarachnoid space. Therefore, raised intracranial pressure is transmitted to the nerve sheath, causing compression of the central retinal vein → papilledema.
Q12. What is the blood supply of the optic nerve?
- Intraocular portion: Posterior ciliary arteries (short posterior) and central retinal artery branches
- Intraorbital portion: Ophthalmic artery via pial plexus
- Intracanalicular: Ophthalmic artery
- Intracranial: Internal carotid artery branches
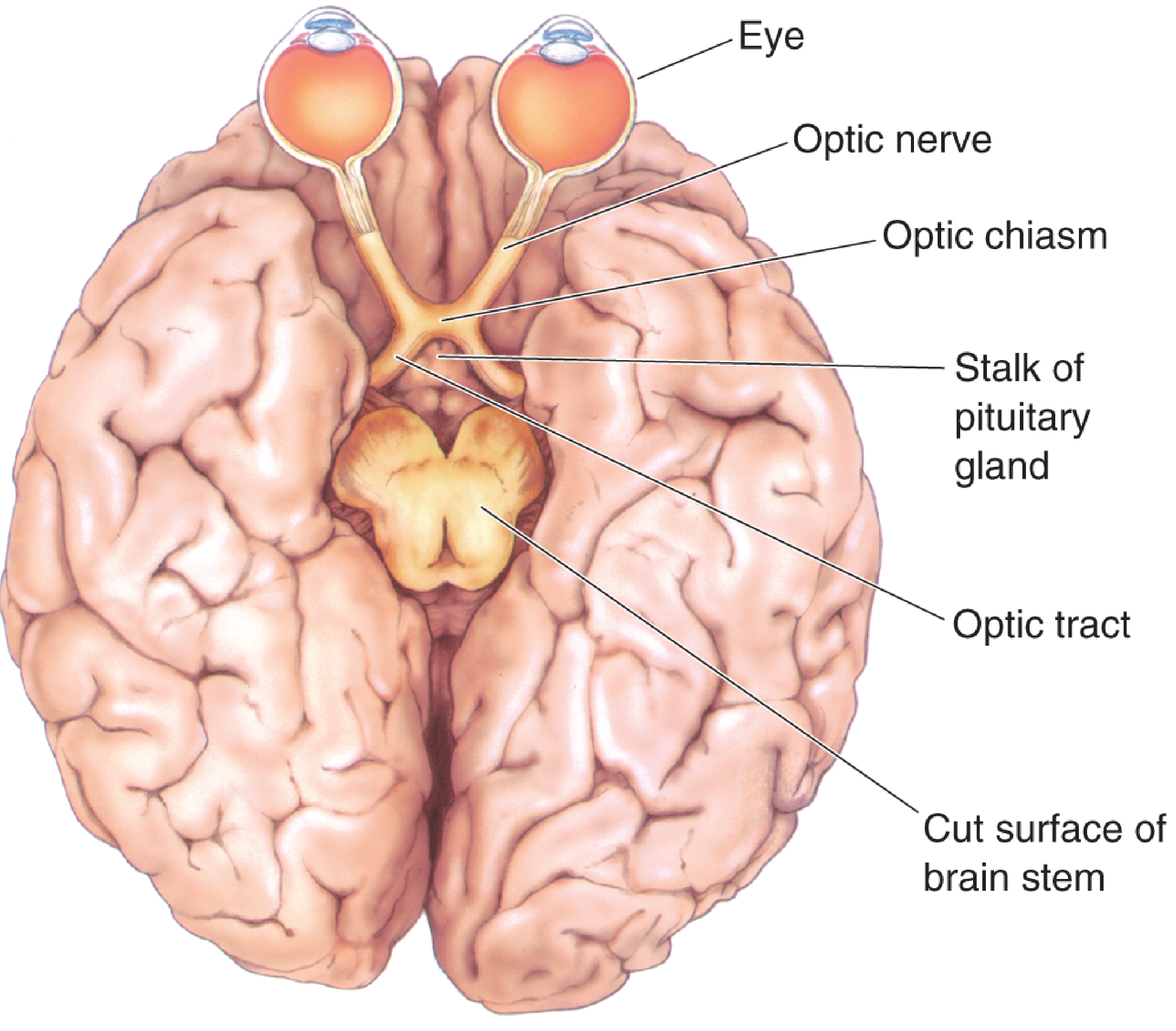
SECTION 3: OPTIC CHIASM
Q13. Where is the optic chiasm located?
Anterior to the infundibular stalk (pituitary stalk), just above the pituitary gland (sella turcica), at the base of the diencephalon. It lies above the diaphragma sellae.
Q14. What fibers decussate at the optic chiasm? What fibers do NOT cross?
- Cross (decussate): Nasal retinal fibers (which carry information from the temporal visual field)
- Do NOT cross (stay ipsilateral): Temporal retinal fibers (which carry information from the nasal visual field)
- This is a partial decussation, unlike the complete crossing of the olfactory or complete non-crossing seen elsewhere.
Q15. Why do nasal fibers cross at the chiasm?
So that all visual information from the left visual hemifield (received by the nasal retina of the right eye + temporal retina of the left eye) travels together in the right optic tract to the right cerebral hemisphere. This allows unified processing of each visual hemifield in the contralateral hemisphere.
Q16. What is the mnemonic for chiasmal fiber arrangement?
"Nasal fibers cross, Temporal fibers travel on the same side."
- N = Nasal = crosses
- T = Temporal = stays (ipsilateral tract)
Q17. What visual field defect results from a lesion at the optic chiasm?
Bitemporal hemianopia - loss of both temporal visual fields. This is the classic defect because the crossing nasal fibers (representing temporal fields) are damaged. Classic cause: pituitary adenoma compressing the chiasm from below.
Q18. What are the named fibers at the chiasm?
- Wilbrand's knee: Nasal fibers from the inferior retina of one eye loop briefly into the contralateral optic nerve before joining the contralateral optic tract. (Note: existence is debated - may be an artefactual finding)
- Junctional scotoma: A lesion at the junction of optic nerve and chiasm → monocular central scotoma (ipsilateral) + superior temporal defect contralaterally (due to Wilbrand's knee involvement)
SECTION 4: OPTIC TRACT
Q19. Describe the course of the optic tracts.
From the chiasm, the optic tracts pass posterolaterally, coursing around the cerebral peduncles of the midbrain, under the pia along the lateral surfaces of the diencephalon, to reach the lateral geniculate nucleus (LGN) of the thalamus.
Q20. What is the fiber composition of each optic tract?
Each optic tract carries:
- Temporal retinal fibers from the ipsilateral eye
- Nasal retinal fibers from the contralateral eye
- Therefore, the right optic tract carries information from the left visual hemifield (from both eyes)
Q21. What visual field defect results from complete optic tract lesion?
Contralateral homonymous hemianopia - loss of the opposite visual hemifield in both eyes. E.g., left optic tract lesion → right homonymous hemianopia. Defect is often incongruous (asymmetric in both eyes) because macular fibers are not yet fully segregated.
Q22. What is the difference between congruous and incongruous visual field defects?
- Congruous: Defect has identical shape in both eyes → posterior lesion (optic radiation/cortex)
- Incongruous: Defect shape differs between the two eyes → anterior lesion (optic tract, or less organized part of the pathway) Rule: The more posterior the lesion, the more congruous the defect.
Q23. What non-visual fibers travel in the optic tract?
Pupillary afferent fibers branch off just before the LGN to reach the pretectal nucleus in the dorsal midbrain (for the pupillary light reflex). These do NOT synapse in the LGN.
SECTION 5: LATERAL GENICULATE NUCLEUS (LGN)
Q24. Where is the LGN and what is its function?
The LGN is the visual relay nucleus in the posterior thalamus (part of the metathalamus). It is the primary relay station between the retina and visual cortex. Optic tract fibers synapse here on LGN neurons whose axons form the optic radiations.
Q25. Describe the layers of the LGN and their significance.
The LGN has 6 layers (numbered 1-6 from ventral to dorsal):
- Layers 1 and 2: Magnocellular (M) layers - receive input from large (M-type) ganglion cells; process motion, depth, low spatial frequency, luminance contrast
- Layers 3-6: Parvocellular (P) layers - receive input from small (P-type) ganglion cells; process color, fine detail, high spatial frequency
- Layers 1, 4, 6: Input from contralateral eye
- Layers 2, 3, 5: Input from ipsilateral eye (Also: Koniocellular layers between the main layers carry color information from bistratified ganglion cells)
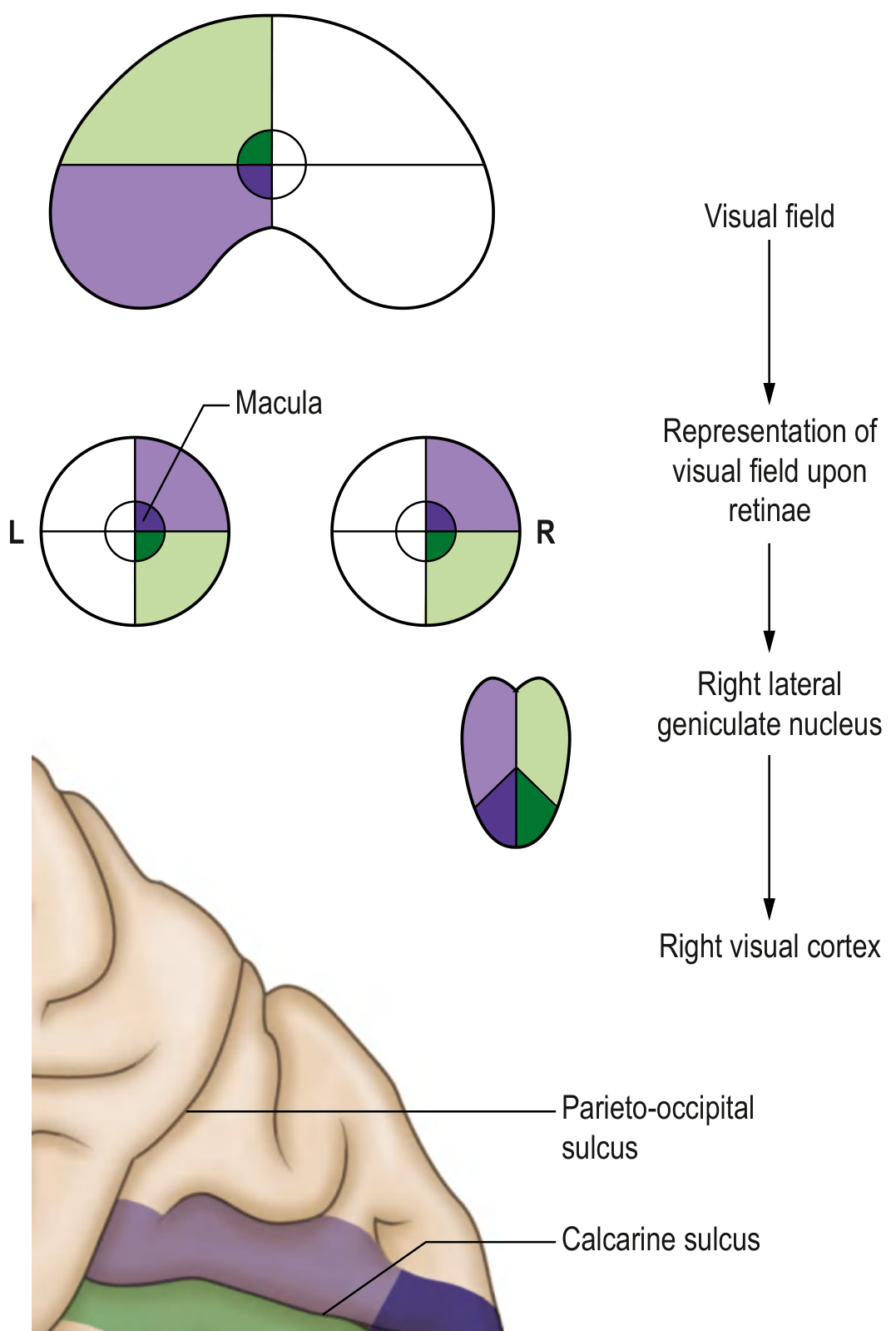
Q26. What is the orientation of the visual map in the LGN?
The visual field is rotated 90 degrees in the LGN compared to the retina: images from the inferior visual field project to the medial half, superior visual field to the lateral half.
Q27. What is the blood supply of the LGN?
The LGN has a dual supply creating a characteristic "notched" sparing pattern in ischemic lesions:
- Anterior choroidal artery (branch of ICA): supplies anterior hilum - upper and lower temporal visual field
- Lateral choroidal artery (posterior choroidal, PCA branch): supplies rest Anterior choroidal artery occlusion can cause a characteristic "wedge-shaped" or "sector" visual field defect sparing horizontal sector (opposite of a typical homonymous hemianopia).
SECTION 6: OPTIC RADIATIONS (Geniculocalcarine Tract)
Q28. Describe the course of the optic radiations.
Axons from LGN neurons form the geniculocalcarine tract (optic radiations), which fans out in two main projections:
- Superior (dorsal) fibers: Travel through the parietal lobe white matter → carry information from the inferior visual field → terminate on the inferior bank of the calcarine fissure (cuneus)
- Inferior (ventral) fibers - Meyer's loop: Initially pass anteriorly and laterally into the temporal lobe before turning posteriorly → carry information from the superior visual field → terminate on the superior bank of the calcarine fissure (lingual gyrus)
Q29. What is Meyer's loop (loop of Meyer)?
The inferior optic radiation fibers that course anteriorly into the temporal lobe around the tip of the inferior horn of the lateral ventricle before turning posteriorly to reach the striate cortex. Named after Adolf Meyer.
Q30. What is the clinical significance of Meyer's loop?
Temporal lobe lesions (e.g., temporal lobectomy for epilepsy, temporal lobe tumors) damage Meyer's loop → contralateral superior quadrantanopia ("pie-in-the-sky" defect) - loss of the upper outer quadrant of vision.
Q31. What is "pie-in-the-sky" vs "pie-on-the-floor" defect?
- Pie-in-the-sky (superior quadrantanopia): Meyer's loop lesion in temporal lobe
- Pie-on-the-floor (inferior quadrantanopia): Parietal lobe lesion affecting superior optic radiation fibers
Q32. What structures does the optic radiation pass through or near?
The optic radiations travel in the retrolenticular and sublenticular portions of the posterior limb of the internal capsule, then through the white matter of the temporal and parietal lobes to reach the occipital lobe.
SECTION 7: PRIMARY VISUAL CORTEX (V1, Striate Cortex, Area 17)
Q33. Where is the primary visual cortex?
In the occipital lobe, along the superior and inferior banks of the calcarine fissure (calcarine sulcus), predominantly on the medial surface of the occipital lobe. It extends slightly onto the posterior surface near the occipital pole.
Q34. Why is it called "striate cortex"?
Because of a visible white stripe - the stria of Gennari (line of Gennari) - visible to the naked eye within the cortex. This corresponds to a thick band of myelinated axons (thalamocortical fibers) in layer IV of the cortex. This gives V1 its distinctive appearance and its alternate name: striate cortex.
Q35. What is macular sparing and why does it occur?
Occipital lobe lesions (e.g., from posterior cerebral artery stroke) often spare central/macular vision despite producing homonymous hemianopia. Proposed reasons:
- The macula has a disproportionately large representation at the occipital pole which has dual blood supply (from PCA and MCA)
- The macular representation in V1 is bilateral (both hemispheres represent the macula)
Q36. What is the retinotopic map in V1?
- Macula (central vision): Projects to the most posterior part of V1 near the occipital pole (magnification factor is large - macula occupies ~50-60% of V1 despite being <3% of retinal area)
- Peripheral retina: Projects to anterior portions of V1
- Upper visual field: Projects to inferior bank of calcarine fissure (lingual gyrus)
- Lower visual field: Projects to superior bank of calcarine fissure (cuneus)
- Left hemifield: Right V1
Q37. What are the layers of V1 (striate cortex)?
V1 has 6 cortical layers. Key features:
- Layer IVc (divided into IVcα and IVcβ): Primary input from LGN (thalamocortical fibers terminate here)
- IVcα: Input from magnocellular layers (M-pathway)
- IVcβ: Input from parvocellular layers (P-pathway)
- Layer II/III: Contains cytochrome oxidase blobs (process color)
- Layer V: Projects to superior colliculus
- Layer VI: Projects back to LGN (feedback)
Q38. What are ocular dominance columns?
Alternating columns in V1 where neurons respond preferentially to one eye vs the other, arranged as stripes in layer IV. Critical period during development establishes these; deprivation amblyopia occurs if input is blocked during this period.
SECTION 8: VISUAL ASSOCIATION AREAS (V2-V5 and beyond)
Q39. What are the two main streams of visual processing beyond V1?
- Dorsal stream (WHERE/HOW pathway): V1 → V2 → V5 (MT) → parietal cortex - processes spatial location, motion, depth, visuomotor guidance
- Ventral stream (WHAT pathway): V1 → V2 → V4 → inferior temporal cortex - processes form, color, object recognition, face recognition
Q40. What is V5 (MT area)?
The middle temporal area, specialized for motion processing. Lesion → akinetopsia (inability to perceive motion; moving objects appear as a series of still frames).
Q41. What is V4?
Specialized for color processing (part of ventral stream). Lesion → achromatopsia (loss of color vision, despite intact brightness perception).
SECTION 9: VISUAL FIELD DEFECTS - THE MASTER CHART
Q42. Summarize all visual field defects by lesion site:
| Level | Lesion Site | Visual Field Defect |
|---|---|---|
| 1 | Optic nerve (complete) | Complete monocular blindness (ipsilateral) |
| 2 | Optic nerve (partial) | Monocular field defect (central scotoma, arcuate, altitudinal) |
| 3 | Optic chiasm (central) | Bitemporal hemianopia |
| 4 | Optic chiasm (lateral) | Binasal hemianopia (rare; from bilateral carotid aneurysms) |
| 5 | Optic tract | Contralateral homonymous hemianopia (incongruous) |
| 6 | LGN (anterior choroidal a.) | Sector/wedge-shaped homonymous defect |
| 7 | Meyer's loop (temporal lobe) | Contralateral superior quadrantanopia ("pie in sky") |
| 8 | Parietal optic radiation | Contralateral inferior quadrantanopia ("pie on floor") |
| 9 | Complete optic radiation | Contralateral homonymous hemianopia (congruous) |
| 10 | Occipital cortex (PCA stroke) | Contralateral homonymous hemianopia WITH macular sparing |
| 11 | Occipital pole (tip) | Contralateral central homonymous scotoma |
| 12 | Bilateral V1 | Cortical blindness (Anton syndrome - patient denies blindness) |
SECTION 10: PUPILLARY LIGHT REFLEX PATHWAY
Q43. Describe the complete afferent pathway of the pupillary light reflex.
Light → Retinal photoreceptors → Ganglion cells (melanopsin-containing ipRGCs also contribute) → Optic nerve → Optic chiasm → Optic tracts → Branch off before LGN → Pretectal olivary nucleus (dorsal midbrain) → Posterior commissure → Both Edinger-Westphal (EW) nuclei (bilateral projection = consensual reflex)
Q44. Describe the efferent pathway of the pupillary light reflex.
EW nucleus → Preganglionic parasympathetic fibers travel with CN III (oculomotor nerve) → Synapse in ciliary ganglion (in orbit) → Postganglionic short ciliary nerves → Sphincter pupillae muscle → Pupil constriction (miosis)
Q45. Why does light in one eye cause constriction in both eyes (consensual reflex)?
Because the pretectal nucleus projects bilaterally to both Edinger-Westphal nuclei via the posterior commissure. Thus one eye's light input produces bilateral pupillary constriction (direct in illuminated eye, consensual in fellow eye).
Q46. What is the Relative Afferent Pupillary Defect (RAPD / Marcus Gunn Pupil)?
In the swinging flashlight test, when light is swung from the normal eye to the affected eye, the affected eye's pupils paradoxically dilate (because the afferent signal from the affected optic nerve is weaker, so the relative withdrawal of light signal from the normal eye outweighs the direct stimulus). This indicates unilateral optic nerve disease. It is the most objective bedside test for optic nerve dysfunction.
Q47. What conditions cause RAPD?
Optic neuritis, optic nerve compression, ischemic optic neuropathy, severe unilateral retinal disease (e.g., CRVO, retinal detachment), optic tract lesion (contralateral, smaller RAPD due to nasal fiber predominance).
Q48. Why does optic tract lesion cause a contralateral RAPD (not ipsilateral)?
Because more nasal fibers (60%) than temporal fibers (40%) cross in the chiasm. A lesion of one optic tract destroys the temporal fibers from the ipsilateral eye + nasal fibers from the contralateral eye. The nasal fiber predominance means the contralateral eye has a weaker afferent signal → contralateral RAPD.
Q49. What is the near (accommodation-convergence) reflex?
Triad: Accommodation (ciliary muscle contraction → lens rounding), convergence (medial recti contraction), miosis (pupil constriction). Pathway goes through the visual cortex (not pretectal nucleus), which is why the Argyll Robertson pupil (syphilis) shows light-near dissociation (near reflex intact, light reflex lost).
SECTION 11: NON-VISUAL PROJECTIONS OF RETINAL GANGLION CELLS
Q50. What are the non-LGN projections of the retinofugal pathway?
- Pretectal nucleus: Pupillary light reflex (branches before LGN)
- Superior colliculus: Reflex eye movements, visual orienting responses, saccade control
- Suprachiasmatic nucleus (SCN) of hypothalamus: Circadian rhythm entrainment (via melanopsin-containing ipRGCs)
- Accessory optic nuclei: Optokinetic reflexes, smooth pursuit eye movements
- Nucleus of the optic tract: Optokinetic nystagmus
Q51. What is melanopsin and what are intrinsically photosensitive retinal ganglion cells (ipRGCs)?
A subset of retinal ganglion cells (~1-2%) that contain melanopsin, a photopigment with peak sensitivity at ~480 nm (blue light). They are intrinsically light-sensitive (do not require rods/cones). Functions include: circadian photoentrainment (project to SCN), pupillary light reflex, regulating sleep/wake cycle. These are preserved in patients with significant photoreceptor degeneration (e.g., advanced retinitis pigmentosa) - explaining why such patients can still entrain to light cycles.
SECTION 12: PHYSIOLOGY OF VISION
Q52. What are the three types of cone photopigments and what is the basis of color vision?
- L-cones (red-sensitive): Peak ~560 nm
- M-cones (green-sensitive): Peak ~530 nm
- S-cones (blue-sensitive): Peak ~420 nm Color perception arises from differential stimulation of these three cone types (trichromatic theory). Color opponent processing (red-green, blue-yellow, luminance channels) occurs in the retina, LGN, and cortex.
Q53. What is the dark adaptation curve and what does it signify?
After exposure to bright light, visual sensitivity increases progressively in the dark over ~30 minutes. The curve shows two phases:
- First 5-7 minutes: Cone adaptation (reaches ~100-fold sensitivity increase)
- Break/kink in curve (Kohlrausch kink): Transition to rod adaptation
- 7-30 minutes: Rod adaptation (ultimate sensitivity ~10,000 × cones) Clinical test: Goldmann-Weekers dark adaptometry. Abnormal in: vitamin A deficiency, retinitis pigmentosa, choroideremia.
Q54. What is the visual acuity and how is it determined anatomically?
Visual acuity is highest at the fovea because:
- Highest cone density and smallest cone size
- Near 1:1 ratio of cones to ganglion cells (no convergence = maximum resolution)
- Optical quality is best along the visual axis Normal: 6/6 (20/20) - can resolve 1 arc-minute separation.
Q55. What is contrast sensitivity? How does it differ from visual acuity?
Contrast sensitivity measures the ability to detect gratings of varying spatial frequency at varying contrast levels. It is impaired earlier than Snellen acuity in many diseases (e.g., optic neuritis, glaucoma). Measured by Pelli-Robson chart or spatial frequency gratings.
Q56. What is the critical flicker fusion (CFF) frequency?
The rate of flickering light above which the flicker is perceived as a steady light. Reduced in optic nerve disease. ~15-20 Hz for rods, ~60 Hz for cones. Measured as a functional test of the visual pathway.
SECTION 13: HIGHER CORTICAL VISUAL DISORDERS
Q57. What is cortical blindness? What is Anton syndrome?
Cortical blindness: Bilateral destruction of V1 → complete loss of visual perception despite intact eyes and optic pathways. Pupils react normally to light (light reflex preserved, as it does not use V1).
Anton syndrome: Cortical blindness + anosognosia (patient denies being blind, confabulates visual experiences). Seen after bilateral posterior cerebral artery strokes.
Q58. What is Balint syndrome?
Bilateral parieto-occipital lesions causing the triad:
- Simultanagnosia: Cannot perceive more than one object at a time
- Optic ataxia: Cannot accurately reach for visually guided targets
- Ocular apraxia (psychic gaze paralysis): Cannot voluntarily direct gaze to a new target
Q59. What is visual agnosia?
Inability to recognize objects by sight despite intact vision, intact memory, and intact object recognition by other senses. Subtypes: aperceptive (cannot form percept) vs associative (can form percept but cannot match to memory). Ventral stream lesion.
Q60. What is prosopagnosia?
Inability to recognize familiar faces. Associated with bilateral fusiform gyrus lesions (inferior temporal-occipital cortex - "fusiform face area").
SECTION 14: OPTIC NERVE LESION PATTERNS (High-yield for OSCE/Theory)
Q61. What are the patterns of optic nerve visual field loss and their causes?
| Defect | Location of Damage | Cause |
|---|---|---|
| Central scotoma | Papillomacular bundle | Optic neuritis, toxic/nutritional optic neuropathy |
| Cecocentral scotoma | Papillomacular bundle + blind spot | Toxic/nutritional optic neuropathy |
| Altitudinal defect (superior/inferior half) | Optic nerve (nerve fiber bundles) | Ischemic optic neuropathy (AION), glaucoma |
| Arcuate scotoma | Arcuate nerve fiber bundles | Glaucoma, AION |
| Nasal step | Nasal fiber bundles | Glaucoma |
| Concentric contraction | Diffuse nerve damage | Retinitis pigmentosa, advanced glaucoma, papilledema |
KEY DIAGRAMS TO KNOW
- Complete visual pathway diagram from retina to occipital cortex with fiber origins labeled
- Visual field defects chart (the "standard" diagram showing all 12 lesion sites)
- Pupillary light reflex arc (afferent + efferent limbs)
- LGN laminar organization (6 layers, ipsi/contra, M/P segregation)
- Retinal fiber arrangement at the optic disc (superior, inferior, papillomacular bundle)
- Meyer's loop course through the temporal lobe
HIGH-YIELD ONE-LINERS (for MCQs)
- Nasal fibers cross at chiasm; temporal stay ipsilateral
- Chiasm lesion = bitemporal hemianopia (pituitary adenoma)
- Meyer's loop = temporal lobe = superior quadrantanopia ("pie in sky")
- Parietal radiation = inferior quadrantanopia ("pie on floor")
- Occipital cortex lesion = homonymous hemianopia WITH macular sparing
- Cortical blindness = intact pupil reflex (reflex bypasses cortex)
- RAPD = swinging flashlight test = optic nerve disease
- Argyll Robertson pupil = syphilis = light-near dissociation
- Striate cortex = V1 = Area 17 = calcarine fissure = line of Gennari
- LGN layers 1,4,6 = contralateral eye; 2,3,5 = ipsilateral eye
- M-cells (layers 1,2) = motion/depth; P-cells (3-6) = color/detail
- ipRGCs + melanopsin = circadian rhythm + direct pupil reflex
- Fovea = rod-free, highest acuity, max cone density
Sources: Gray's Anatomy for Students; Goldman-Cecil Medicine, 27th ed.; Neuroscience: Exploring the Brain, 5th ed.; Adams & Victor's Principles of Neurology, 12th ed.; Kanski's Clinical Ophthalmology, 10th ed.; Localization in Clinical Neurology, 8th ed.; Guyton & Hall Medical Physiology, 14th ed.
This is a shared conversation. Sign in to Orris to start your own chat.