I want to learn basic anatomy and clinical anatomy for ent so teach me anatomy of pharynx from relevant anatomy and ent books
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Here is a complete, structured lesson on the anatomy of the pharynx drawn from Gray's Anatomy for Students, Scott-Brown's Otorhinolaryngology Head & Neck Surgery, and Cummings Otolaryngology.
Anatomy of the Pharynx
1. Overview and Definition
The pharynx is a musculofascial half-cylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck. It serves as a common pathway for air and food.
- Superiorly: attached to the base of the skull (basisphenoid and basal occipital bone)
- Inferiorly: continuous with the top of the esophagus at the level of vertebra C6
- Anteriorly: attached to the margins of the nasal cavities, oral cavity, and larynx
- Posteriorly: separated from the vertebral column by the retropharyngeal space (loose connective tissue)
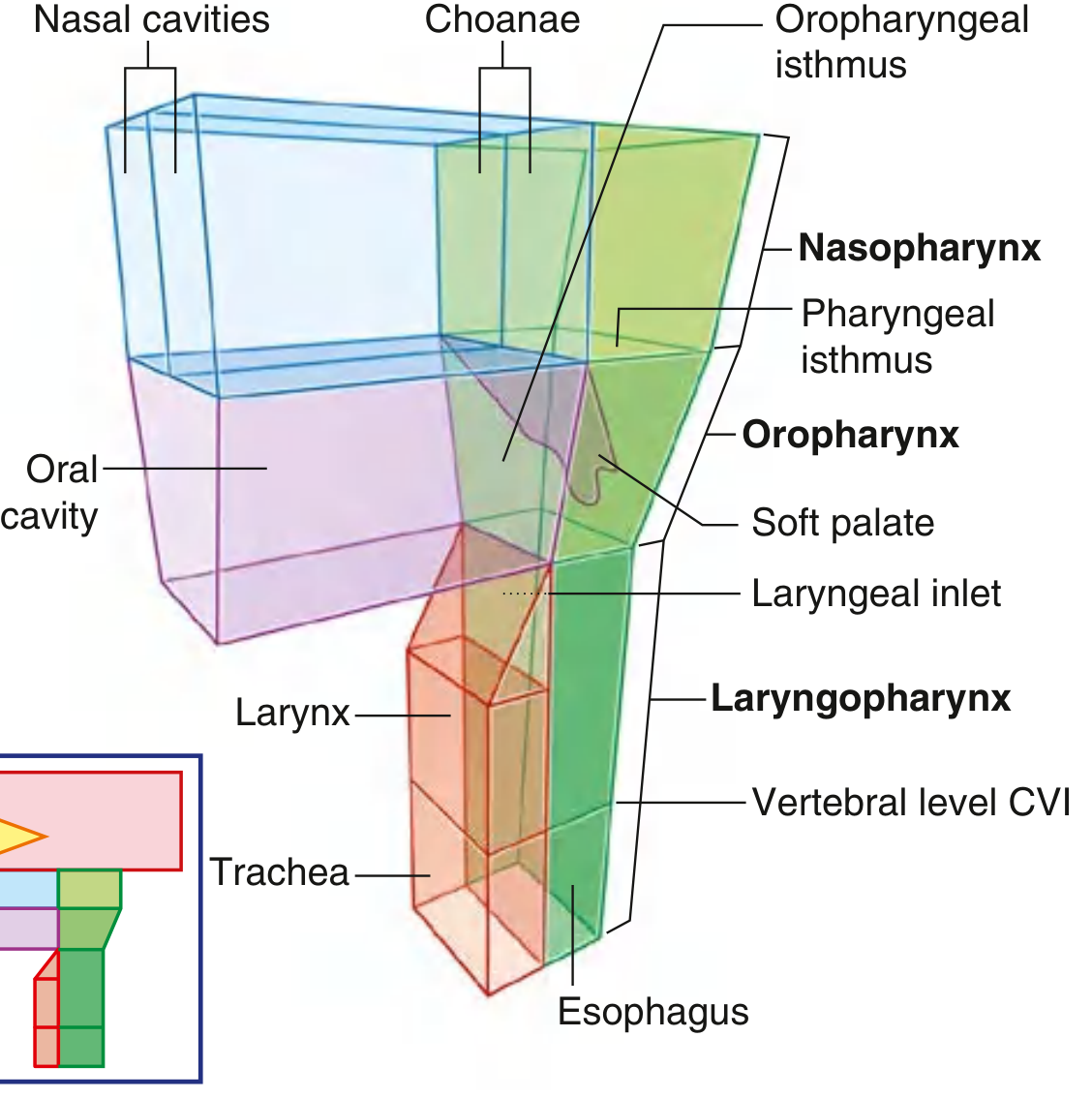
2. Subdivisions
The pharynx is divided into three parts based on anterior relationships:
| Division | Also Called | Boundaries |
|---|---|---|
| Nasopharynx | Epipharynx | Behind choanae, above the soft palate |
| Oropharynx | Mesopharynx | Behind oral cavity, from soft palate to hyoid bone |
| Laryngopharynx | Hypopharynx | Behind larynx, from hyoid to C6 (esophageal inlet) |
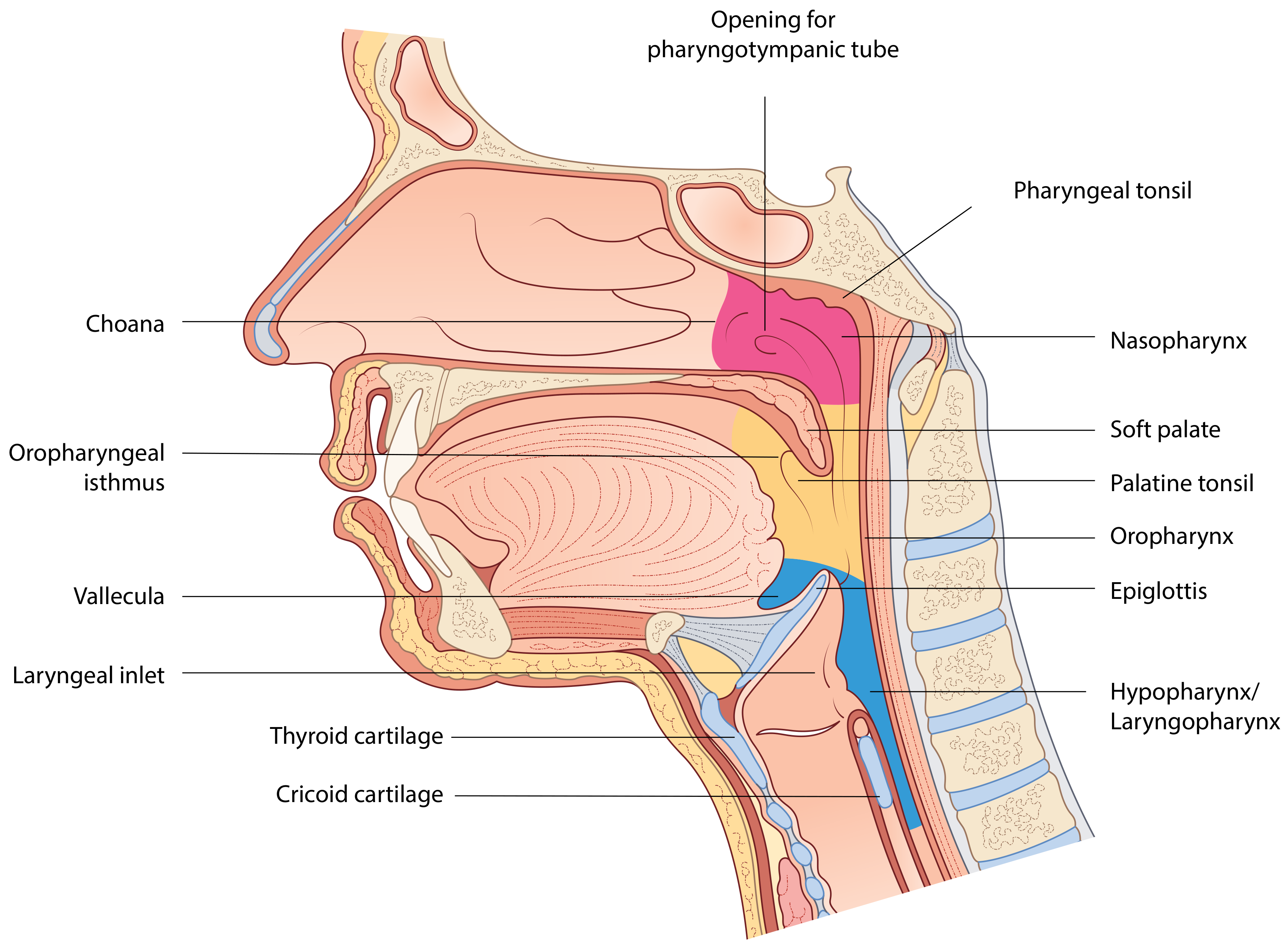
3. Nasopharynx
Basic Anatomy
- Located above the soft palate, behind the choanae (posterior nasal apertures)
- Has a roof, two lateral walls, a posterior wall, and a floor
- The roof and posterior wall are contiguous due to the sloping base of the sphenoid and occipital bones - collectively called the basisphenoid
- Always patent (walls are rigid bony/cartilaginous structures) - unlike the oropharynx and hypopharynx which open and close with swallowing
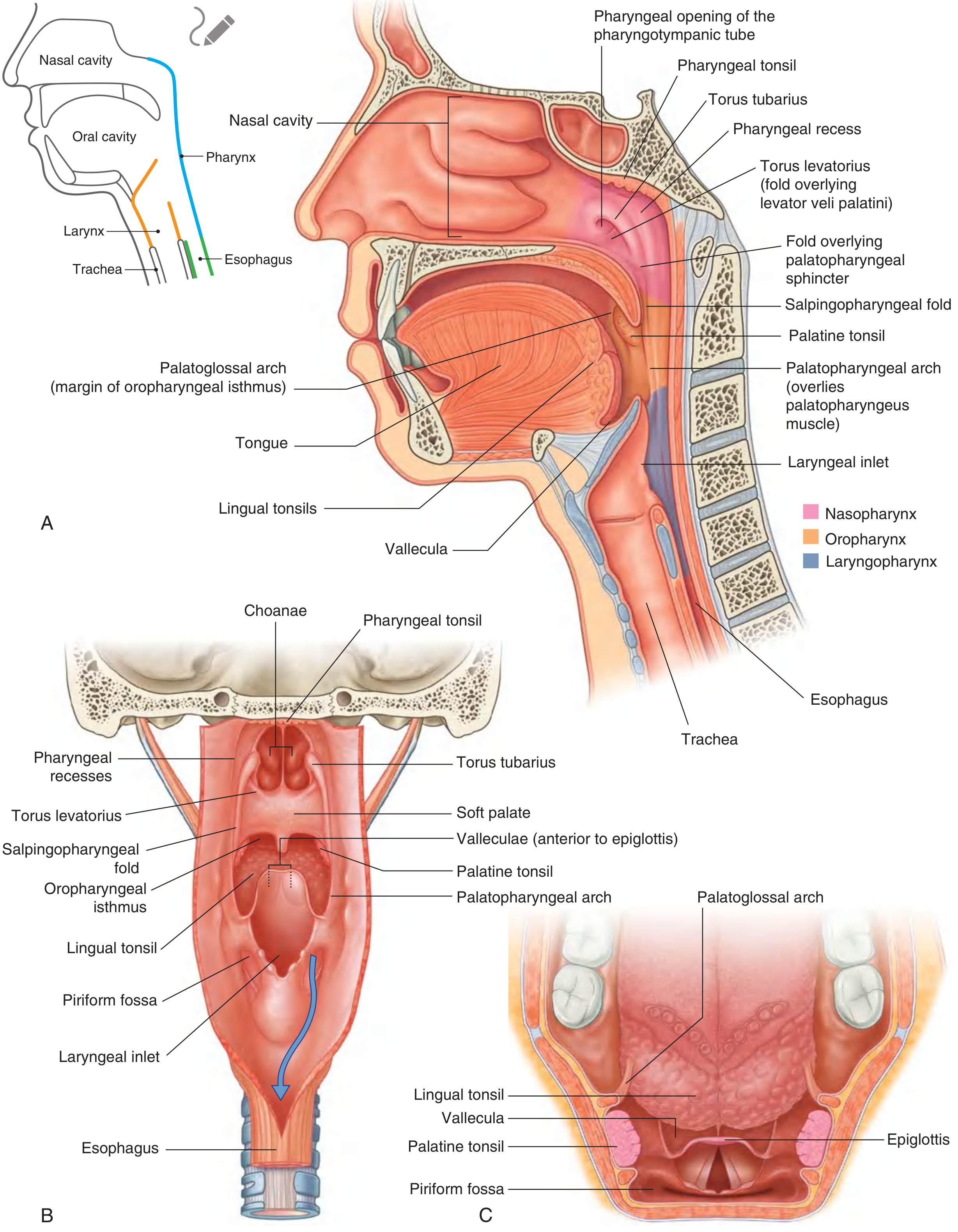
Key Features of the Lateral Wall
- Pharyngotympanic (Eustachian/Auditory) tube opening - posterior to and slightly above the level of the hard palate
- Torus tubarius - a mucosal elevation formed by the cartilaginous end of the tube projecting into the nasopharynx
- Pharyngeal recess (Fossa of Rosenmüller) - a recess posterior to the torus tubarius; clinically important as the most common site of nasopharyngeal carcinoma
- Torus levatorius - a mucosal fold overlying the levator veli palatini muscle, inferior to the torus tubarius
- Salpingopharyngeal fold - a mucosal fold that descends from the lower end of the torus tubarius
Floor
- The floor is the upper surface of the soft palate
- The pharyngeal isthmus lies posterior to the soft palate - this is the communication between the nasopharynx and oropharynx
- Closure of the isthmus during swallowing is achieved by elevation of the soft palate + contraction of the palatopharyngeal sphincter (part of the superior constrictor)
Pharyngeal Tonsil (Adenoids)
- Lymphoid tissue in the mucosa of the roof and posterior walls
- Maximal in childhood; contributes to upper respiratory tract defense
- No clear plane of cleavage (unlike palatine tonsils) - makes adenoidectomy less precise
- When enlarged = adenoids - can occlude the nasopharynx, forcing mouth breathing
Mucosa
- Ciliated pseudostratified columnar (respiratory) epithelium - unique to this part of the pharynx
4. Oropharynx
Basic Anatomy (Clinical Boundaries from Scott-Brown's)
- Superiorly: horizontal line at the level of the hard palate (or free border of soft palate)
- Inferiorly: horizontal line through the floor of the valleculae (hyoid bone level)
- Anteriorly: vertical plane of the palatoglossal folds, including the posterior 1/3 of the tongue
Subsites (UICC/AJCC Classification)
Anterior subsites:
- Base of tongue (posterior to vallate papillae / posterior 1/3)
- Vallecula (between the tongue and epiglottis)
Lateral subsites:
- Palatine tonsils
- Tonsillar fossae and tonsillar (faucial) pillars
- Glossotonsillar sulci
Superior subsites:
- Inferior surface of the soft palate and uvula
Posterior wall
Key Structures
The Soft Palate:
- Suspended from the posterior border of the hard palate; a mobile flap that opens and closes on swallowing
- Contains five muscles all attached to the palatine aponeurosis
- The uvula (musculus uvulae) hangs from its free inferior border into the oropharyngeal isthmus
Faucial Pillars (Tonsillar Pillars):
- Anterior pillar = palatoglossal arch (contains palatoglossus muscle) - forms the anterior boundary of the oropharyngeal isthmus
- Posterior pillar = palatopharyngeal arch (contains palatopharyngeus muscle)
- The palatine tonsil sits in the tonsillar fossa between these two arches
Valleculae:
- Paired shallow depressions anterior to the epiglottis
- The median glossoepiglottic fold divides them in the midline
- Flanked laterally by the lateral glossoepiglottic (pharyngoepiglottic) folds
- Common site for foreign bodies (e.g., fish bones)
Mucosa
- Non-keratinized stratified squamous epithelium (same as rest of pharynx below the transitional zone)
5. Laryngopharynx (Hypopharynx)
Basic Anatomy (Clinical Boundaries from Scott-Brown's)
- Extends from the superior margin of the epiglottis (level of the cranial border of the hyoid bone) to the lower margin of the cricoid cartilage at C6, where the pharynx becomes the esophagus
- The laryngeal inlet (aditus) is the missing anterior segment - the communication between the larynx and pharynx, bounded superiorly by the epiglottis, laterally by the aryepiglottic folds, and inferiorly by the arytenoids and cricoid cartilage
Subsites
- Piriform recesses (fossae/sinuses) - bilateral
- Posterior pharyngeal wall
- Postcricoid area (pharyngo-esophageal junction)
Piriform Recess - Clinically Most Important
- Bilateral channels lateral to the laryngeal inlet between the larynx medially and the thyroid cartilage/thyrohyoid membrane laterally
- Medial boundary: quadrangular membrane of the larynx
- Lateral boundary: thyrohyoid membrane (superiorly), thyroid cartilage lamina (inferiorly)
- Broader superiorly, narrower inferiorly - funnel-shaped
- Function: directs food and liquid around the laryngeal inlet into the esophagus
- Clinical: foreign bodies commonly lodge here; tumors can silently expand asymptomatically until neck nodes appear
Postcricoid Area
- Extends from the arytenoid cartilages to the inferior border of the cricoid cartilage
- Forms the anterior wall of the hypopharynx
- Lateral margins merge with the medial wall of the piriform recesses
Mucosa
- Predominantly stratified squamous epithelium with goblet cells
6. Pharyngeal Wall - Layers (from Scott-Brown's)
From deep to superficial, five layers:
- Mucous membrane - respiratory in nasopharynx; squamous below
- Submucosa (fibrous layer, also called pharyngobasilar fascia at its inner aspect)
- Pharyngobasilar fascia - inner fascial layer, thicker, lines the deep surface
- Muscular layer - constrictors + longitudinal muscles
- Buccopharyngeal fascia - outer thin layer, part of the pretracheal fascia
7. Muscles of the Pharynx
A. Constrictor Muscles (Circular - form most of the wall)
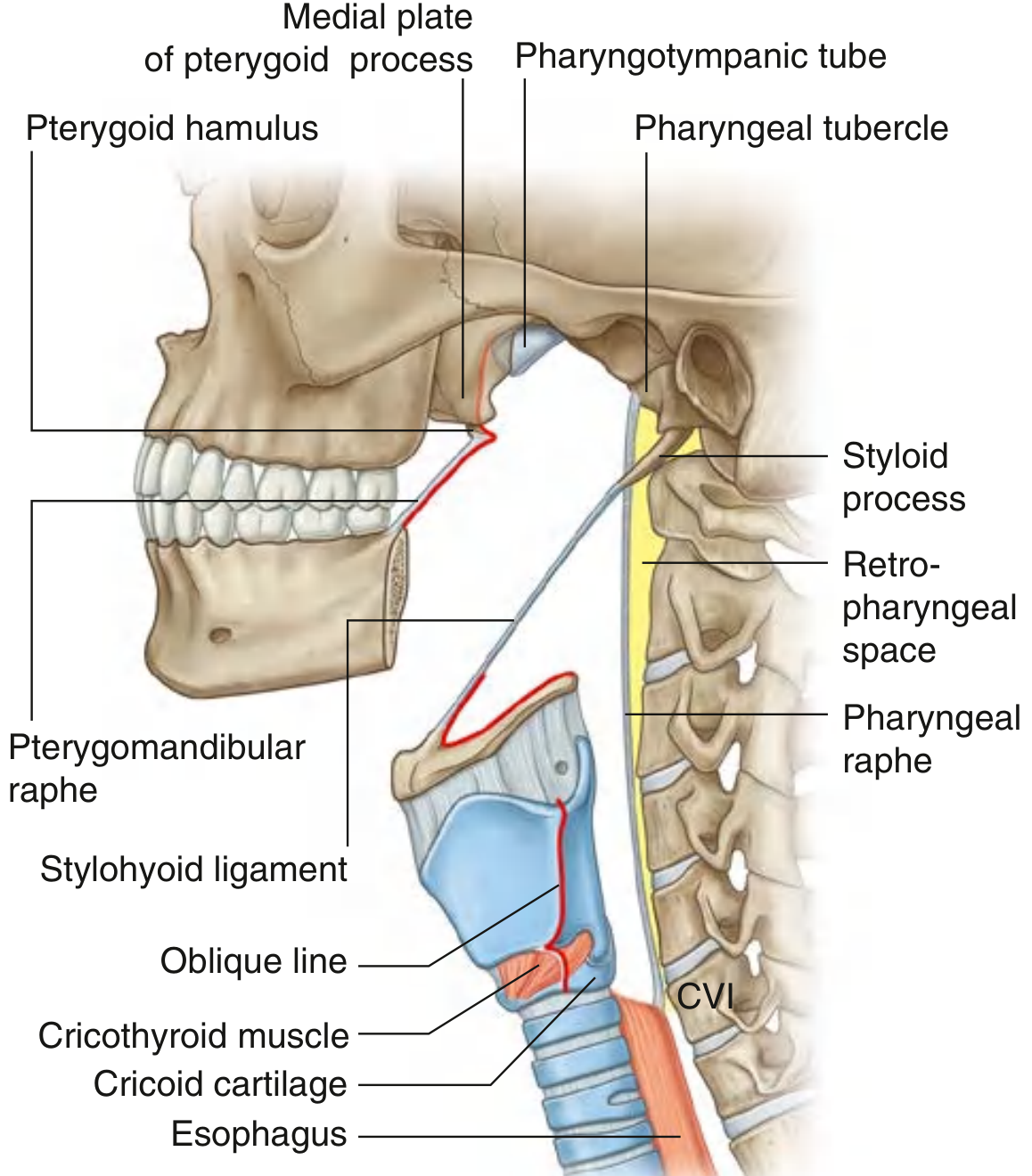
The three constrictors overlap like stacked flower pots - inferior overlapping middle, which overlaps superior. They all insert posteriorly into the pharyngeal raphe (a midline fibrous cord descending from the pharyngeal tubercle on the basioccipital bone to C6).
| Muscle | Anterior Attachment | Innervation | Function |
|---|---|---|---|
| Superior constrictor | Pterygomandibular raphe + pterygoid hamulus + mandible | Vagus [X] via pharyngeal plexus | Constricts upper pharynx; palatopharyngeal sphincter |
| Middle constrictor | Greater horn of hyoid + stylohyoid ligament + lesser horn | Vagus [X] via pharyngeal plexus | Constricts mid-pharynx |
| Inferior constrictor | Oblique line of thyroid cartilage + cricoid cartilage | Vagus [X] via pharyngeal plexus | Constricts lower pharynx; upper esophageal sphincter |
Killian's Dehiscence (Killian's Triangle):
The inferior constrictor has two parts - thyropharyngeus (from thyroid) and cricopharyngeus (from cricoid, acts as upper esophageal sphincter). The triangular gap between them is Killian's dehiscence - a site of muscular weakness in the posterior pharyngeal wall. A Zenker's (pharyngeal) diverticulum occurs when mucosa herniates through this gap.
B. Longitudinal Muscles (Elevate the pharynx)
| Muscle | Origin | Insertion | Innervation | Function |
|---|---|---|---|---|
| Stylopharyngeus | Medial base of styloid process | Pharyngeal wall | Glossopharyngeal [IX] (unique!) | Elevates pharynx |
| Salpingopharyngeus | Inferior end of pharyngotympanic tube | Pharyngeal wall | Vagus [X] | Elevates pharynx |
| Palatopharyngeus | Upper surface of palatine aponeurosis | Pharyngeal wall | Vagus [X] | Elevates pharynx; closes oropharyngeal isthmus |
Key point: Stylopharyngeus is the only pharyngeal muscle supplied by CN IX - all others are vagus [X].
8. Waldeyer's Tonsillar Ring
A circumpharyngeal ring of mucosa-associated lymphoid tissue (MALT) at the entry to the aerodigestive tract. Its role is immune sampling and maturation.
| Component | Location |
|---|---|
| Pharyngeal tonsil (Adenoids) | Roof and posterior wall of nasopharynx |
| Tubal tonsils | Near pharyngotympanic tube openings |
| Palatine tonsils | Tonsillar fossae of oropharynx (between pillars) |
| Lingual tonsils | Posterior 1/3 of tongue (base of tongue) |
Palatine Tonsil - Special Features (ENT High-Yield):
- Bounded by palatoglossal and palatopharyngeal arches
- Encapsulated - unlike all others in Waldeyer's ring - this provides the surgical dissection plane during tonsillectomy
- The floor of the tonsillar bed is the superior constrictor
- Surface has multiple crypts and an intratonsillar cleft
- Blood supply: tonsillar branch of the facial artery (main supply; enters inferior pole through superior constrictor) + ascending palatine, ascending pharyngeal, lingual, descending palatine arteries
- Venous drainage: pharyngeal venous plexus + external palatine (paratonsillar) vein - this vein is commonly injured in tonsillectomy and causes post-operative bleeding
- Lymphatics drain to: jugulodigastric (tonsillar) lymph node (level II) - the first node to enlarge in tonsillitis
- Nerve supply: tonsillar plexus (branches of glossopharyngeal [IX] + lesser palatine nerve from maxillary [V2])
- Because CN IX also innervates the tympanic cavity via the tympanic nerve, tonsil pathology can cause referred otalgia
9. Blood Supply
Arteries (all ultimately from external carotid artery)
Upper pharynx:
- Ascending pharyngeal artery (direct branch of external carotid)
- Ascending palatine and tonsillar branches of facial artery
- Branches of maxillary and lingual arteries
Lower pharynx:
- Pharyngeal branches of the inferior thyroid artery (from thyrocervical trunk of subclavian artery)
Veins
- Form a pharyngeal venous plexus on the outer wall
- Drains superiorly into the pterygoid plexus (infratemporal fossa)
- Drains inferiorly into the facial vein and internal jugular vein
Lymphatics
- Deep cervical nodes
- Retropharyngeal nodes (between nasopharynx and vertebral column) - important in nasopharyngeal carcinoma
- Paratracheal and infrahyoid nodes
- Palatine tonsil drains to jugulodigastric nodes (level IIA)
10. Nerve Supply
Motor Innervation
All pharyngeal muscles are supplied by Vagus [X] via the pharyngeal plexus, EXCEPT:
- Stylopharyngeus → Glossopharyngeal [IX]
The Pharyngeal Plexus
Formed by:
- Pharyngeal branch of the vagus [X] (major motor nerve)
- Branches from the external laryngeal nerve (branch of superior laryngeal nerve of vagus)
- Pharyngeal branches of glossopharyngeal [IX]
The plexus lies in the outer (buccopharyngeal) fascia of the pharyngeal wall.
Sensory Innervation (by region)
| Region | Sensory Nerve |
|---|---|
| Nasopharynx | Pharyngeal branch of Maxillary nerve [V2] (through palatovaginal canal) |
| Oropharynx | Glossopharyngeal [IX] via pharyngeal plexus (afferent limb of gag reflex) |
| Base of tongue / Vallecula | Internal laryngeal nerve (branch of superior laryngeal of Vagus [X]) |
| Laryngopharynx | Vagus [X] via internal branch of superior laryngeal nerve |
Gag reflex: Afferent = CN IX (sensory from oropharynx); Efferent = CN X (motor to pharyngeal muscles)
11. Radiological Anatomy (from Cummings Otolaryngology)
On fluoroscopic / CT imaging of the pharynx:
- Torus tubarius, Fossa of Rosenmüller, uvula are identified on CT of nasopharynx
- Piriform sinuses - asymmetry is normal; complete lack of filling is suspicious for tumor
- Postcricoid line - formed by barium pooling between the posterior larynx and posterior hypopharyngeal wall; disruption = tumor invasion
- Cricopharyngeus muscle - lies anterior to C6 vertebra; appears as an indentation on the posterior hypopharyngeal wall
- Normal CT cross-sectional diameter of cervical esophagus: AP ≤ 16 mm, lateral ≤ 24 mm
12. Swallowing Mechanics - Clinical Anatomy
During swallowing:
- Soft palate elevates → closes pharyngeal isthmus → seals nasopharynx from oropharynx (prevents nasal regurgitation)
- Oropharyngeal isthmus opens → food enters pharynx
- Laryngeal inlet closes (epiglottis tilts, aryepiglottic folds adduct)
- Food is directed through the piriform recesses around the larynx into the esophagus
- You cannot breathe and swallow simultaneously - the airway is closed at two points (pharyngeal isthmus and larynx)
13. Summary of Key Clinical Correlations
| ENT Condition | Anatomical Basis |
|---|---|
| Adenoid hypertrophy | Enlargement of pharyngeal tonsil in nasopharynx roof → nasal obstruction + mouth breathing |
| Otitis media with effusion | Dysfunction of pharyngotympanic tube opening in nasopharyngeal lateral wall |
| Nasopharyngeal carcinoma | Arises most often in the Fossa of Rosenmüller |
| Peritonsillar abscess (Quinsy) | Pus in loose areolar tissue between tonsillar capsule and superior constrictor |
| Tonsillectomy bleeding | External palatine (paratonsillar) vein near lateral tonsil surface |
| Referred otalgia from tonsil | Shared CN IX supply to tonsil and tympanic cavity (via tympanic nerve) |
| Zenker's diverticulum | Mucosa herniates through Killian's dehiscence (gap between thyropharyngeus and cricopharyngeus) |
| Foreign body in piriform fossa | Narrow funnel shape traps sharp objects; endoscopy required |
| HPV oropharyngeal cancer | Base of tongue and palatine tonsils (Waldeyer's ring) - most common sites |
Sources:
- Gray's Anatomy for Students, pp. 1180-1191 (pharynx, muscles, vessels, nerves)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp. 781-786 (nasopharynx, oropharynx, hypopharynx, pharyngeal wall, Waldeyer's ring)
- Cummings Otolaryngology Head and Neck Surgery, p. 1876 (radiological anatomy, cross-sectional CT)
Everything on nose
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Here is a complete, structured lesson on the anatomy of the nose drawn from Scott-Brown's Otorhinolaryngology, K.J. Lee's Essential Otolaryngology, Cummings Otolaryngology, and Gray's Anatomy for Students.
Complete Anatomy of the Nose
1. Embryology
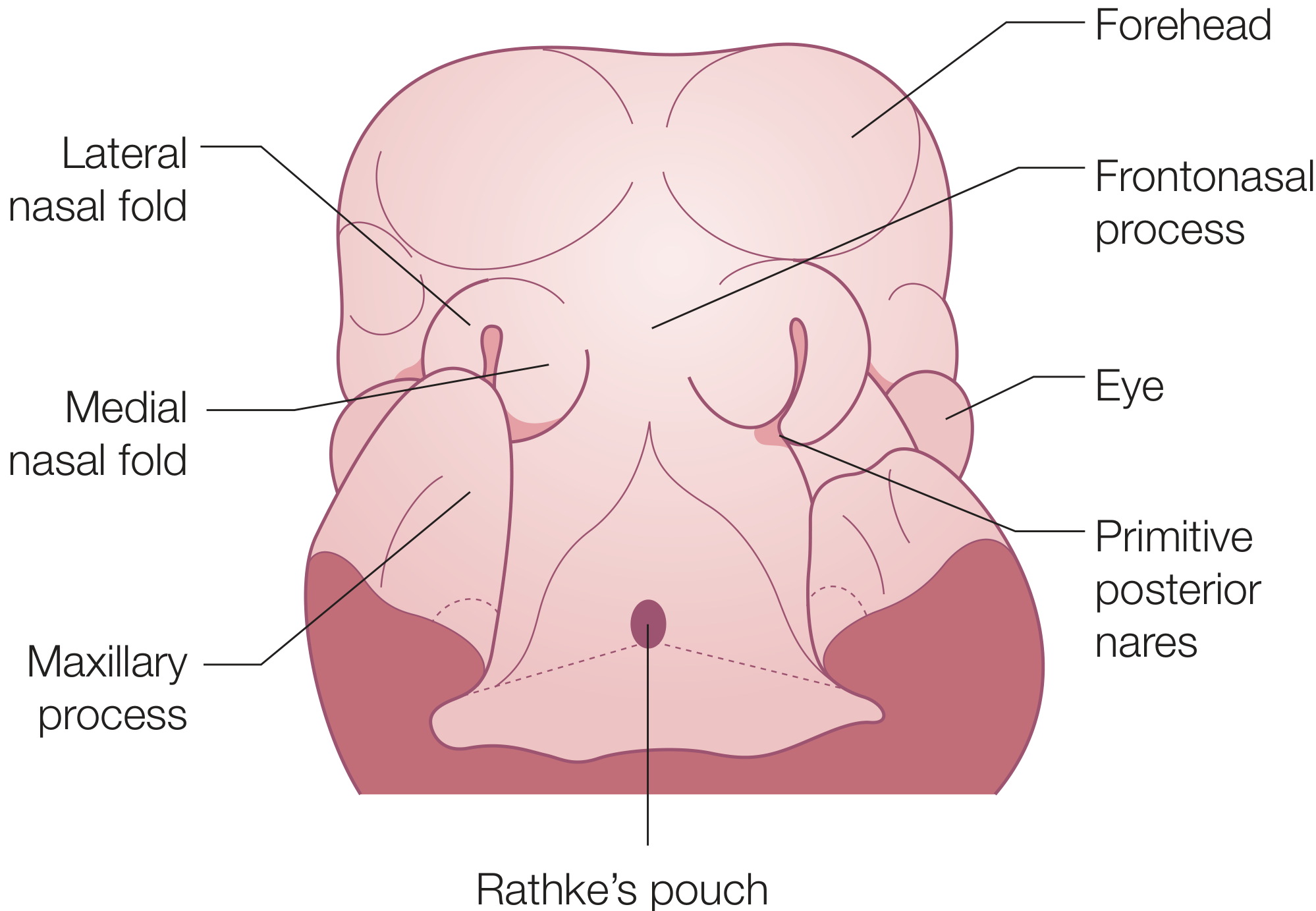
Development begins in the 4th week of gestation:
- Neural crest cells proliferate and form nasal placodes
- Nasal placodes sink to form the nasal pits (primitive anterior nares)
- The bucconasal membrane normally breaks down to form the choanae - failure = choanal atresia
Processes and what they form:
| Process | Structure Formed |
|---|---|
| Frontal + maxillary processes | Lateral 2/3 of upper lip, superior alveolar ridges, palatal shelves |
| Medial nasal prominences + maxillary process | Philtrum, medial crus of lower lateral cartilages |
| Lateral nasal prominences | Nasal bones, upper lateral cartilages, lateral crus of lower lateral cartilages |
| Frontonasal process (posterior midline) | Nasal septum |
Turbinate embryology (from K.J. Lee):
- Turbinate precursors appear in the 8th week of gestation
- Maxilloturbinal (from maxillary process) → inferior turbinate
- Ethmoturbinals (from ethmoid, 5 arise but only 4 persist):
- 1st ethmoturbinal: ascending portion → agger nasi; descending portion → uncinate process (regresses)
- 2nd ethmoturbinal → middle turbinate
- 3rd ethmoturbinal → superior turbinate
- 4th + 5th → supreme turbinate (when present)
- Primary furrows form between ethmoturbinals giving rise to the meati
2. External Nose
A. Landmarks (K.J. Lee)
| Landmark | Description |
|---|---|
| Nasion | Nasofrontal suture (bony depression at root of nose) |
| Radix | Nasal root; centered at nasion |
| Rhinion | Bony-cartilaginous junction along dorsum |
| Supratip break | Junction between dorsum and lobule, just above tip-defining point |
| Tip-defining points | Two points of maximum light reflection on nasal tip (corresponding to domes of lower lateral cartilages) |
| Infratip break | Lobule-columella junction |
| Nasal sill | Nostril rim between columella and alar-facial attachment |
| Columella | Bridge of skin between the two nostrils |
B. Subcutaneous Layers (K.J. Lee mnemonic: "SF DeeP")
- S - Superficial fatty layer (connected to dermis)
- F - Fibromuscular layer (nasal SMAS - superficial musculoaponeurotic system)
- D - Deep fatty layer (contains neurovascular system)
- P - Periosteum/Perichondrium
The optimal surgical plane for rhinoplasty dissection is between D and P - it is avascular and heals with minimal fibrosis.
C. Nasal Osteology
- Two nasal bones fuse in midline forming a pyramidal shape
- Nasal bones are thicker superiorly than inferiorly
- Attachments: Superior = nasal process of frontal bone; Lateral = frontal process of maxilla
- Pyriform aperture (bony opening to nasal cavity):
- Superior = caudal margin of nasal bones
- Inferior = alveolar process of maxilla
- Lateral = frontal process of maxilla
- Medial = nasal septum
D. Nasal Cartilages
| Cartilage | Key Points |
|---|---|
| Upper lateral cartilage (ULC) | Attached superiorly to nasal bones; articulates inferiorly with cephalic margin of LLC (scroll area); medially continuous with quadrangular cartilage |
| Lower lateral cartilage (LLC) | Gives shape to nasal tip; composed of medial and lateral crura |
| Sesamoid cartilages | Between lateral crura and pyriform aperture |
| Quadrangular (septal) cartilage | Forms the cartilaginous septum; continuous with ULC at dorsum |
Keystone area = convergence of caudal nasal bone, perpendicular plate of ethmoid, cephalic margin of ULC, and cartilaginous septum - failure to preserve = nasal collapse.
E. Nasal Tip Support
Major supports:
- Medial and lateral crura of LLC
- Attachment of medial crura to caudal edge of quadrangular cartilage
- Attachment of ULC to LLC at the scroll area
Minor supports:
- Skin-soft tissue envelope
- Sesamoid complex
- Interdomal ligament
- Anterior nasal spine
- Cartilaginous septal dorsum
- Membranous nasal septum
F. Nasal Muscles
| Group | Muscles | Action |
|---|---|---|
| Elevators | Procerus, levator labii superioris alaeque nasi, anomalous nasi | Shortens nose, dilates nostrils |
| Depressors | Depressor septi, alar nasalis | Lengthens nose, dilates nostrils |
| Compressors | Compressor narium minor, transverse nasalis | Lengthens nose, constricts nostrils |
3. Nasal Cavity
The nasal cavity extends from the external nares anteriorly to the posterior choanae (opening into the nasopharynx). It is divided into two passages by the nasal septum. Each side has:
- A floor, roof, medial wall (septum), and lateral wall
A. Floor
- Anterior 3/4: palatine process of maxilla
- Posterior 1/4: horizontal process of palatine bone
- ~12 mm behind the anterior nasal floor lies the incisive canal containing the nasopalatine nerve and greater palatine artery
B. Roof
- Formed by the skull base; slopes downward from anterior to posterior
- This slope is surgically important - during endoscopic sinus surgery, the skull base descends as you proceed posteriorly toward the sphenoid sinus
C. Nasal Vestibule
- The entrance of the nasal cavity
- Lined by hair-bearing keratinized squamous epithelium with sebaceous and sweat glands (vibrissae)
- Boundaries:
- Medial = nasal septum
- Superior and lateral = LLC
- Inferior = alveolar process of maxilla
- Posterior = Limen nasi (formed by the caudal margin of the ULC) - this is where skin transitions to respiratory mucosa
D. Epithelium of the Nasal Cavity (3 types)
| Zone | Epithelium |
|---|---|
| Nasal vestibule | Squamous (keratinized) |
| Superior septum, superior turbinate, upper middle turbinate | Olfactory epithelium (pseudostratified, with olfactory receptor neurons) |
| Remainder of nasal cavity | Respiratory epithelium (pseudostratified ciliated columnar with goblet cells) |
4. Nasal Septum
The nasal septum has three components:
A. Bony Septum
| Bone | Location |
|---|---|
| Perpendicular plate of ethmoid | Upper 1/3 of septum; continuous superiorly with cribriform plate and crista galli |
| Vomer | Posterior and inferior septum; its two alae articulate with the sphenoid rostrum forming vomerovaginal canals (containing pharyngeal branches of maxillary artery) |
| Maxillary crest | Inferior midline ridge of maxilla |
| Palatine bone | Posterior part of inferior nasal crest |
B. Cartilaginous Septum
- The quadrilateral (quadrangular) cartilage - the most important component
- Bound to nasal bones, perpendicular plate of ethmoid, and vomer by collagenous fibers
- Continuous with the ULC superiorly at the nasal dorsum
- The septal tail (sphenoidal process) extends posteriorly between vomer and perpendicular plate - a harvest site for cartilage in revision rhinoplasty
- Inferior attachment sits in the maxillary nasal crest bound by looser tissue (pseudoarthrosis) - allows mobility, reducing fracture risk with trauma
C. Membranous Septum
- Connective tissue between the caudal portion of the septal cartilage and the columella
- Site of the hemitransfixion/transfixion incision in septoplasty
Vomeronasal Organ (Jacobsen's organ)
- Auxiliary olfactory organ for pheromone perception in animals
- In humans: largely regresses in utero; identified as a groove in the anterior-inferior nasal septum
5. Lateral Nasal Wall
A. Bones of the Lateral Wall (anterior to posterior)
- Frontal process of maxilla
- Lacrimal bone
- Medial maxillary wall (inferior) / Lamina papyracea (LP) of ethmoid (superior)
- Perpendicular plate of palatine bone
- Medial pterygoid plate of sphenoid (latter two form the sphenopalatine foramen)
B. Turbinates (Conchae)
Shelves of bone covered in erectile mucosa that warm, humidify, and filter air while regulating airflow resistance. Three constant turbinates: inferior, middle, superior (and occasionally a supreme).
- Middle and superior turbinates = ethmoid bone extensions
- Inferior turbinate = independent osseous structure (embryologically distinct)
The Nasal Cycle:
Turbinates continuously dilate and constrict alternately every 0.5-3 hours under sympathetic control - a normal physiological phenomenon. Total nasal resistance remains constant as one side congests and the other decongests.
C. Meati and Sinus Drainage
| Meatus | Turbinate Above It | What Drains Into It |
|---|---|---|
| Inferior meatus | Inferior turbinate | Nasolacrimal duct (Hasner's valve, ~1 cm posterior to head of inferior turbinate) |
| Middle meatus | Middle turbinate | Frontal, anterior ethmoid, and maxillary sinuses (via hiatus semilunaris) |
| Superior meatus | Superior turbinate | Posterior ethmoid sinuses |
| Sphenoethmoidal recess | Above/posterior to superior turbinate | Sphenoid sinus |
D. Middle Turbinate - Detailed (ENT High-Yield)
The middle turbinate (MT) has three attachment points in three different planes:
| Portion | Orientation | Attachment | Significance |
|---|---|---|---|
| Anterior | Sagittal | Junction of cribriform plate and lateral lamella | Delimits fovea ethmoidalis from cribriform plate |
| Middle (Basal/Ground lamella) | Coronal (vertical) | Lateral attachment to lamina papyracea | Divides anterior from posterior ethmoid |
| Posterior (Horizontal attachment) | Axial (horizontal) | Crista ethmoidalis of palatine bone, just anterior to sphenopalatine foramen | Risk of bleeding when MT is resected |
MT Variations:
- Concha bullosa - pneumatized middle turbinate; present in ~1/3 of the population; can narrow ethmoid infundibulum
- Paradoxical MT - lateral surface of MT is convex (reversed curve)
E. Key Endoscopic Landmarks
Lamellae of the lateral nasal wall (anterior to posterior):
- First lamella = Uncinate process (UP)
- Second lamella = Ethmoid bulla (EB)
- Third lamella = Basal lamella of middle turbinate (key division between ant. and post. ethmoid)
- Fourth lamella = Basal lamella of superior turbinate
- Fifth lamella = Basal lamella of supreme turbinate (when present)
Agger nasi = most anterior ethmoid cell; anterior to the frontal recess; identified as a mound above the axilla of the MT on endoscopy.
Uncinate Process (UP):
- Crescent-shaped bone of ethmoid origin; shields the natural maxillary ostium
- Vertical portion attaches to the lacrimal line (frontal process of maxilla / lacrimal bone junction)
- Horizontal portion attaches to inferior turbinate
- The superior attachment of the UP determines frontal sinus drainage:
- Attaches to LP → frontal sinus drains medial to UP, directly into middle meatus (80% - most common)
- Attaches to fovea ethmoidalis or MT → frontal sinus drains into ethmoid infundibulum
F. Osteomeatal Complex (OMC)
The OMC is the functional unit of anterior sinus drainage:
- Posterior boundary: Basal lamella of MT
- Medial: MT
- Lateral: Lamina papyracea
- Superior: Fovea ethmoidalis
It is the key site in the pathophysiology of acute rhinosinusitis - obstruction here affects frontal, anterior ethmoid, and maxillary sinus drainage simultaneously.
G. Key Structures
Hiatus semilunaris:
- 2D crescentic opening into the ethmoid infundibulum
- Bounded anteriorly by UP, posteriorly by the ethmoid bulla
Ethmoid Infundibulum:
- 3D trough: UP (medial) + LP (lateral) + ethmoid bulla (posterosuperior)
- Opens inferiorly at the maxillary sinus natural ostium
Lacrimal Drainage Pathway:
Upper/lower punctum → Canaliculi → Common canaliculus → Valve of Rosenmüller → Lacrimal sac → Nasolacrimal duct → Valve of Hasner → Inferior meatus
6. Nasal Valves
| Valve | Boundaries | Notes |
|---|---|---|
| Internal nasal valve | Nasal septum + caudal edge of ULC + anterior face of inferior turbinate | Normally 10-15° angle; narrowest cross-sectional area; site of greatest airflow resistance; does NOT change during inspiration |
| External nasal valve | Nasal ala laterally + nasal septum + columella medially | Situated caudal to internal valve; normally dilates during inspiration (active dilator: dilator naris anterior) |
7. Blood Supply
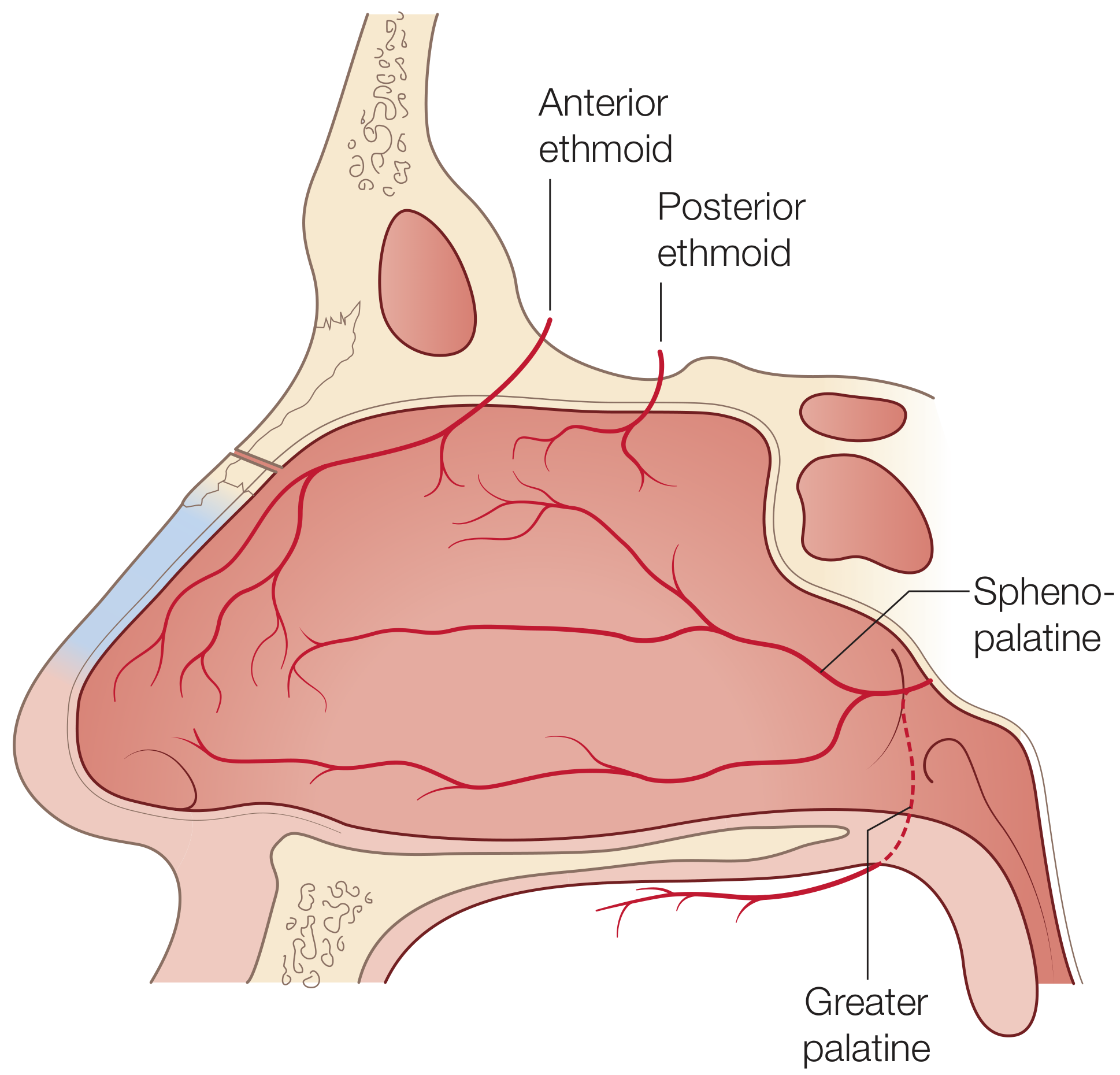
Nasal Septum
Blood supply comes from both the internal and external carotid systems:
External carotid system (via internal maxillary artery):
- Sphenopalatine artery → posterior septal artery → posteroinferior septum
- The posterior septal artery is the basis of the nasoseptal mucosal flap (workhorse flap for endoscopic skull base reconstruction)
- Greater palatine artery → enters via incisive canal → anteroinferior septum
- Septal branch of superior labial artery (from facial artery) → caudal septum and columella
Internal carotid system (via ophthalmic artery):
- Anterior ethmoid artery → anterosuperior septum
- Posterior ethmoid artery → posterosuperior septum
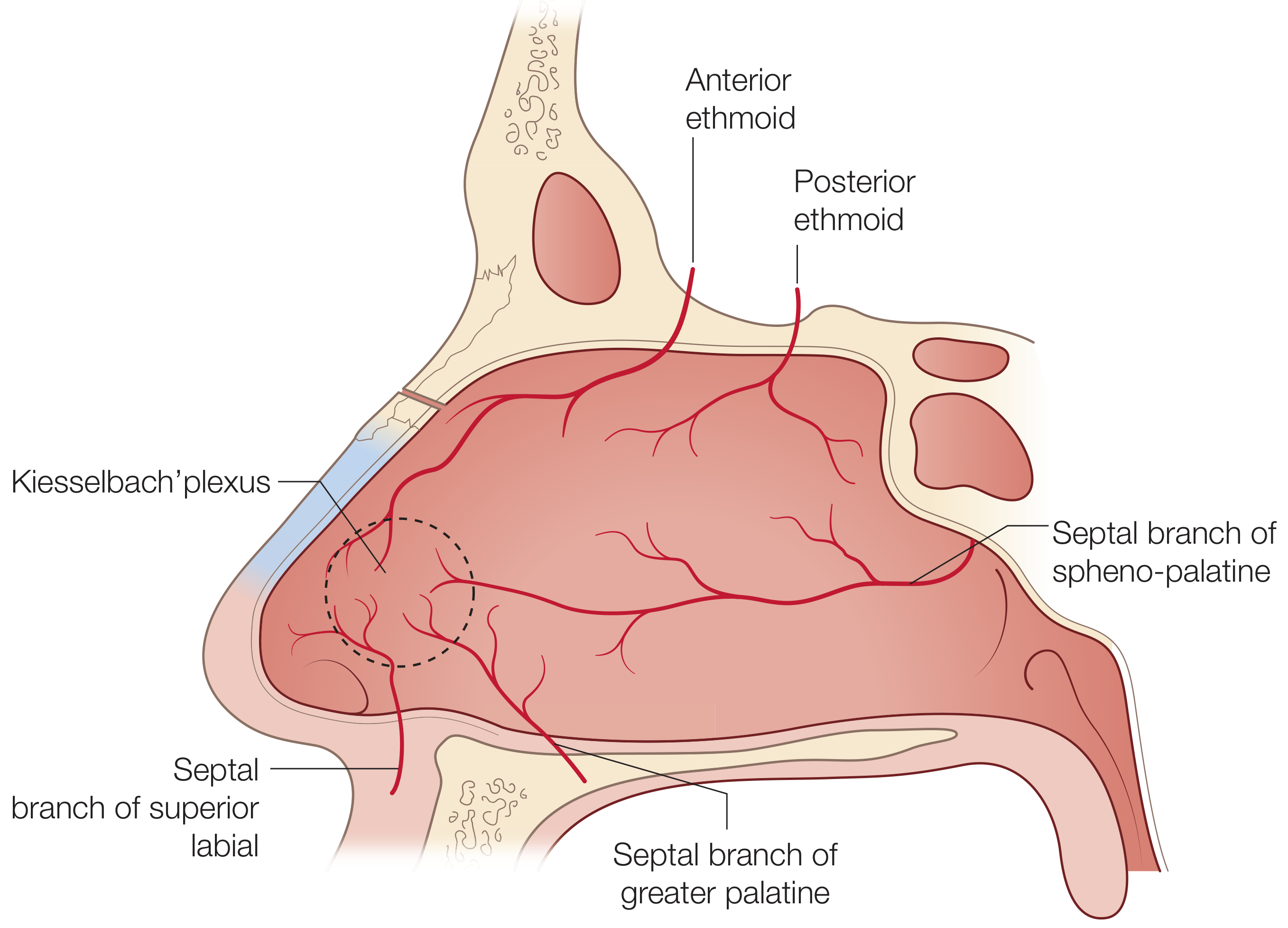
Little's Area (Kiesselbach's Plexus):
The anterior nasal septum is where the anterior ethmoid artery, posterior septal artery (from sphenopalatine), and the septal branch of the superior labial artery anastomose into a rich vascular bed of long capillary loops. This is:
- The most common site of epistaxis (90% of nosebleeds)
- Vulnerable to turbulent airflow, dry air, and digital trauma
Lateral Nasal Wall
- Sphenopalatine artery (dominant supply) - enters through sphenopalatine foramen, just inferior to horizontal attachment of MT; the crista ethmoidalis is the endoscopic landmark to find this vessel
- Anterior and posterior ethmoid arteries (from ophthalmic / ICA) - supply superior lateral wall
- Greater palatine artery - inferior lateral wall near palate
- Facial artery branch - small contribution to anterior lateral wall
Anterior ethmoid artery traverses three compartments:
- Orbit (within the orbital fat)
- Anterior cranial fossa (above cribriform plate)
- Nasal cavity (where it may be dehiscent and visible during ESS)
Veins
- Drain via sphenopalatine vessels into the pterygoid plexus posteriorly
- Drain into facial veins anteriorly
- Superiorly, ethmoidal veins communicate with the superior ophthalmic system
- May have direct connections through the foramen cecum into the superior sagittal sinus (route of intracranial spread of infection)
8. Nerve Supply
Sensory Innervation
| Region | Nerve |
|---|---|
| Anterior nasal cavity (anterior septum and lateral wall) | Anterior ethmoid nerve (from V1/ophthalmic via nasociliary nerve) |
| Superior nasal cavity | Posterior ethmoid nerve (from V1) |
| Posteroinferior lateral wall and turbinates | Posterolateral nasal branches of V2 (maxillary nerve) via sphenopalatine foramen |
| Septum (posterior and inferior) | Nasopalatine nerve (from V2 via sphenopalatine ganglion, runs through incisive canal) |
| Olfaction | Olfactory nerve (CN I) - axons of olfactory receptor neurons pierce cribriform plate to reach olfactory bulb |
Autonomic Innervation (the Vidian nerve pathway)
The Vidian nerve (nerve of the pterygoid canal) carries:
- Greater superficial petrosal nerve (parasympathetic, from CN VII) - presynaptic fibers
- Deep petrosal nerve (sympathetic, from the superior cervical ganglion on the ICA)
These synapse in the sphenopalatine (pterygopalatine) ganglion → postsynaptic fibers distributed to the nasal mucosa.
| Autonomic Division | Function | Pathway |
|---|---|---|
| Parasympathetic | Regulates nasal secretions | Via vidian nerve → sphenopalatine ganglion → nasal mucosa |
| Sympathetic | Regulates vascular tone and turbinate congestion | Via vidian nerve → pass through (not synapse in) sphenopalatine ganglion → nasal mucosa |
Vidian neurectomy can be performed for intractable vasomotor rhinitis to reduce hypersecretion.
9. Key Clinical Correlations
| ENT Condition | Anatomical Basis |
|---|---|
| Choanal atresia | Failure of bucconasal membrane to break down; bony (90%) or membranous (10%); presents as neonatal respiratory distress (neonates are obligate nasal breathers) |
| Anterior epistaxis | Kiesselbach's plexus at Little's area on anterior septum; managed with silver nitrate cautery |
| Posterior epistaxis | Sphenopalatine artery / posterior septal artery; severe, requires endoscopic sphenopalatine artery ligation |
| CSF rhinorrhea | Cribriform plate fracture (roof of nasal cavity); continuity of olfactory filaments and meninges breached |
| Acute rhinosinusitis | OMC obstruction → blocked drainage of maxillary, anterior ethmoid, and frontal sinuses |
| Concha bullosa | Pneumatized middle turbinate; narrows ethmoid infundibulum → predisposes to sinusitis |
| Deviated nasal septum | Trauma or growth displacement of septal cartilage from maxillary crest; treated by septoplasty |
| Nasal valve collapse | Internal nasal valve (10-15° angle) narrowed by thickened ULC or septal deviation → nasal obstruction |
| Dacryocystorhinostomy (DCR) | Creates connection between lacrimal sac and inferior meatus; bypasses blocked nasolacrimal duct |
| Orbital injury in ESS | Lamina papyracea forms the lateral boundary of the ethmoid labyrinth; penetration → orbital hematoma |
| Anosmia after skull base fracture | Shearing of olfactory filaments at cribriform plate; or damage to olfactory epithelium (superior septum + superior/upper middle turbinate) |
| Sphenopalatine artery ligation | Crista ethmoidalis (crest of palatine bone) is the key endoscopic landmark just anterior to the sphenopalatine foramen |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, pp. 1009-1016 (external nose embryology, nasal cavity, nasal septum, blood supply)
- K.J. Lee's Essential Otolaryngology, pp. 509-513 (embryology, external anatomy, nasal cartilages, turbinates, OMC, osteomeatal complex)
- Scott-Brown's Otorhinolaryngology, pp. 1014-1016 (nasal septum, Kiesselbach's plexus, turbinate cycle)
- Cummings Otolaryngology Head and Neck Surgery, p. 189 (imaging of nasal cavity, anatomic variants)
Ear
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Here is the complete anatomy of the ear, drawn from Shambaugh Surgery of the Ear, K.J. Lee's Essential Otolaryngology, Cummings Otolaryngology, and Scott-Brown's Otorhinolaryngology.
Complete Anatomy of the Ear
The ear is divided into three anatomical parts: the external ear, middle ear, and inner ear.
Part 1: The External Ear
A. The Auricle (Pinna)
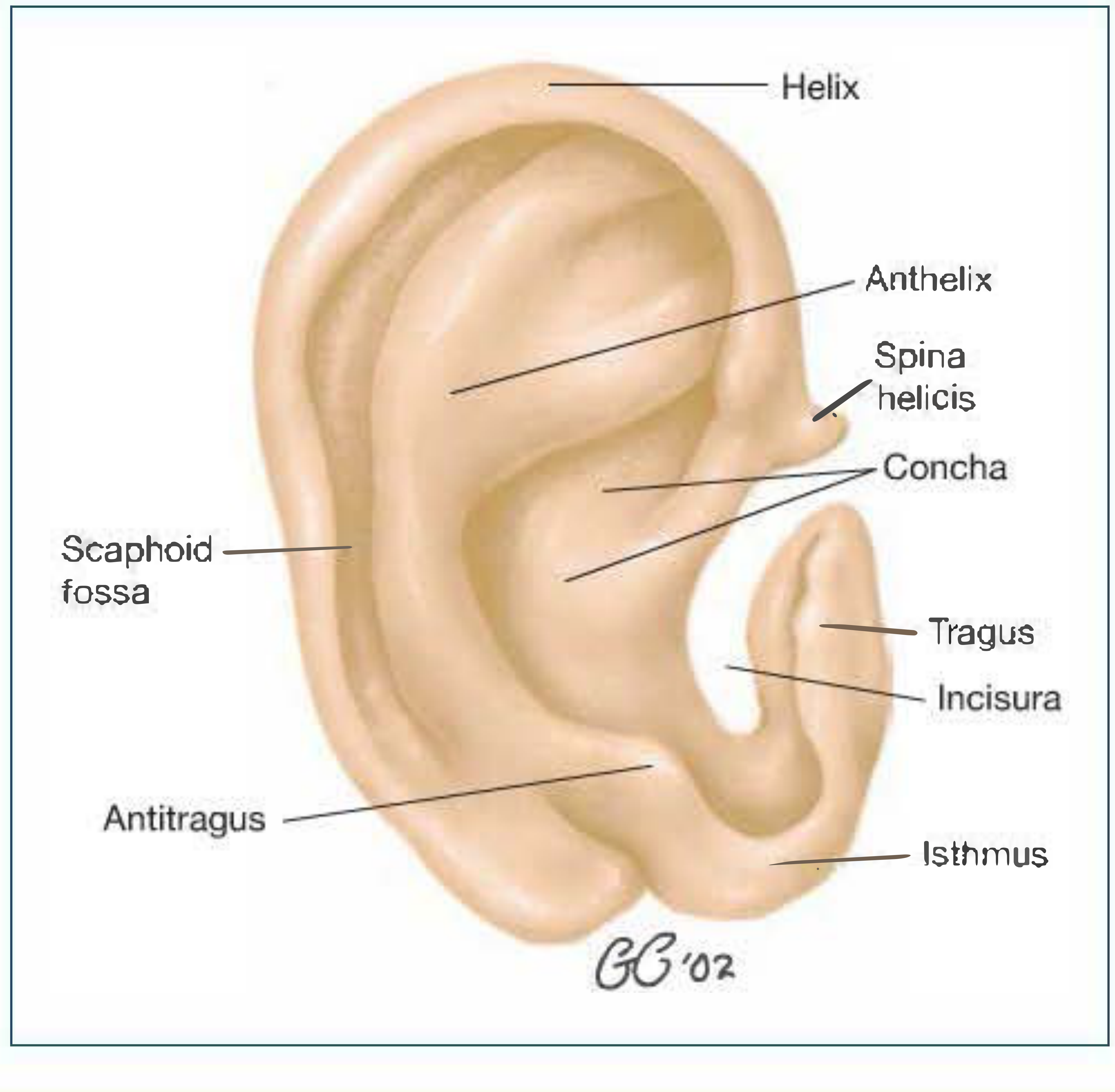
The auricle is a cartilaginous and skin-covered structure that collects and funnels sound. Its key landmarks are:
| Landmark | Description |
|---|---|
| Helix | Outer curved rim of the auricle |
| Antihelix | Inner curved ridge parallel to the helix; bifurcates superiorly into two crura |
| Scaphoid fossa | Groove between helix and antihelix |
| Triangular fossa | Space between the two crura of the antihelix |
| Concha | Deep central bowl of the auricle; leads to EAC |
| Tragus | Small anterior cartilaginous projection over the canal opening |
| Antitragus | Small projection opposite the tragus |
| Incisura | Notch between tragus and antitragus |
| Lobule | Inferior fleshy, cartilage-free portion |
The auricle has a single continuous cartilaginous framework (elastic fibrocartilage) except the lobule and a small area behind the lobe (where the ear is attached to the head).
Blood supply: Posterior auricular artery (branch of external carotid) and superficial temporal artery - both branches of the external carotid artery.
Nerve supply of the auricle and EAC (Shambaugh):
- Auriculotemporal nerve (branch of V3 / mandibular) - anterior auricle and EAC
- Greater auricular nerve (C3 - cervical plexus) - lower lateral face, lobule, lower auricle
- Lesser occipital nerve (C2, C3) - posterior scalp and upper auricle
- Arnold's nerve (auricular branch of vagus, CN X) - posterior EAC and floor of EAC
- Stimulation → cough reflex (Arnold's reflex / ear-cough reflex)
- Facial nerve (CN VII) twigs - small contribution
Because the EAC has vagal innervation via Arnold's nerve, inserting a cotton bud or syringing the ear can trigger coughing, or rarely fainting (vasovagal). This is also why referred otalgia can arise from the larynx, pharynx, and esophagus.
B. External Auditory Canal (EAC)
Dimensions: ~2.4-2.5 cm long; the isthmus (narrowest point) lies just medial to the bony-cartilaginous junction.
Two parts:
| Feature | Cartilaginous (Lateral 1/3) | Bony (Medial 2/3) |
|---|---|---|
| Length | ~8 mm | ~16 mm |
| Framework | Elastic cartilage (continuation of auricular cartilage) | Tympanic bone (floor + walls) + squamous bone (roof) |
| Skin | Thick; contains hair follicles, sebaceous glands, cerumen (apocrine) glands | Very thin; NO adnexal structures, NO hair |
| Direction | Inward, downward, forward | Slightly upward and backward toward TM |
Key features:
- Fissures of Santorini - two or three vertical perforations in the anterior cartilaginous canal wall; allow passage of infection / tumor to the parotid gland
- Incisura terminalis - superior gap in the cartilaginous canal; used for the endaural incision in ear surgery
- Isthmus - narrowest point, ~5 mm from the TM; the anterior recess (wedge between TM and anterior canal wall) is deep to the isthmus and difficult to access surgically
- Tympanic sulcus - bony groove at the medial end where the TM annulus sits; absent superiorly (notch of Rivinus)
- Suture lines in the bony canal:
- Tympanosquamous suture - anterior wall
- Tympanomastoid suture - posterior wall
- These form the "vascular strip" landmarks in surgery
To straighten the EAC for otoscopy:
- Adults: Pull pinna upward and backward
- Neonates/infants: Pull pinna downward and backward (the bony EAC is undeveloped; TM is more horizontal)
Epithelial migration (self-cleaning):
The skin of the bony EAC has a unique centrifugal migration pattern - keratinocytes migrate from the umbo outward toward the cartilaginous canal where debris is shed. This prevents wax accumulation. Failure of this mechanism → cerumen impaction and EAC cholesteatoma.
Part 2: The Middle Ear
A. Tympanic Membrane (TM)

The TM is a four-layered, cone-shaped, concave membrane that forms the lateral wall of the middle ear:
Layers (from lateral to medial):
- Squamous epithelium (skin, continuous with EAC)
- Radiate fibrous layer (outer fibrous layer - inserts onto manubrium of malleus)
- Circular fibrous layer (inner; arranged circumferentially at periphery)
- Mucosal layer (continuous with middle ear mucosa)
Key dimensions (K.J. Lee):
- Average total area: 70-80 mm²
- Average vibrating surface: 55 mm² (effective area for sound transduction)
- Lies at a 45° angle to the long axis of the petrous pyramid in adults
Parts of the TM:
| Part | Description |
|---|---|
| Pars tensa | Lower, larger portion; contains all four layers; ~10 mm diameter; most of TM |
| Pars flaccida (Shrapnell's membrane) | Superior portion; lacks the middle fibrous layers; attached to bony rim of notch of Rivinus superiorly |
Dividing landmark: The anterior and posterior mallear folds extend from the notch of Rivinus to the lateral process of the malleus, dividing the TM into pars flaccida (above) and pars tensa (below).
Key points visible on otoscopy:
- Umbo - most medial/depressed point; where the tip of the malleus manubrium attaches
- Mallear stria (light stripe) - line of manubrium visible through TM
- Lateral process of malleus - anterosuperior knuckle-like projection
- Cone of light - anteroinferior light reflex (right ear: 5 o'clock; left ear: 7 o'clock)
- Annulus - fibrocartilaginous ring anchoring TM to tympanic sulcus
Through the translucent pars tensa you can see: long process of incus, incudostapedial joint, round window niche, chorda tympani, promontory.
B. Tympanic Cavity (Middle Ear)
The middle ear is an air-filled space within the temporal bone. It is divided into three levels:
| Compartment | Location | Contents |
|---|---|---|
| Epitympanum (Attic) | Above the level of the TM annulus | Head of malleus, body and short process of incus; communicates with mastoid via aditus ad antrum |
| Mesotympanum | Level of the TM | Ossicular chain, promontory, oval window, round window, chorda tympani, tensor tympani |
| Hypotympanum | Below the level of the TM annulus | Variable; floor determined by jugular bulb height |
Six walls of the tympanic cavity:
| Wall | Also called | Key Structures |
|---|---|---|
| Lateral wall | Membranous wall | Tympanic membrane (mainly); scutum (bony lateral epitympanic wall) |
| Medial wall | Labyrinthine wall | Promontory (basal cochlear turn); oval window (fenestra vestibuli); round window (fenestra cochleae); facial nerve canal (horizontal segment); lateral semicircular canal prominence |
| Anterior wall | Carotid wall | Internal carotid artery; Eustachian tube opening; semicanal for tensor tympani (above Eustachian tube) |
| Posterior wall | Mastoid wall | Aditus ad antrum (leads to mastoid); pyramidal eminence (stapedius tendon exits here); sinus tympani (posterior recesses); facial nerve (vertical segment) |
| Superior wall | Tegmental wall | Tegmen tympani (thin bony plate separating middle ear from middle cranial fossa/brain) |
| Inferior wall | Jugular wall | Jugular bulb (covered by thin bone; can be dehiscent - seen as blue mass behind TM) |
Key Medial Wall Structures in Detail:
- Promontory - formed by the basal turn of cochlea; covered by the tympanic plexus (formed by Jacobson's nerve = tympanic branch of CN IX, + branches from carotid plexus)
- Jacobson's nerve "points" toward the cochleariform process - a surgical landmark for locating the facial nerve
- Oval window (fenestra vestibuli) - superior to promontory; occupied by the footplate of the stapes (average 1.41 mm × 2.99 mm); sealed by the annular ligament
- Round window (fenestra cochleae) - inferior to promontory; sealed by the round window membrane (secondary tympanic membrane); leads to scala tympani; separated from oval window by the subiculum
- Facial nerve (horizontal segment) - runs in a bony canal (fallopian canal) just superior to the oval window; makes first genu (sharp bend) anteriorly above the cochleariform process, then runs posteriorly
- Lateral semicircular canal - prominent bulge on medial wall of epitympanum; most commonly injured/violated landmark in mastoid surgery
- Cochleariform process - spoon-shaped bony prominence where tensor tympani tendon bends to insert on malleus; key surgical landmark for the first genu of the facial nerve
- Ponticulus - bony ridge from oval window to sinus tympani (defines superior extent of sinus tympani)
- Subiculum - bony ridge from round window to sinus tympani (defines inferior extent of sinus tympani)
Epitympanum (Attic) - Surgical Importance:
- Contains: head of malleus + body and short process of incus (in the fossa incudis)
- Fossa incudis (houses short process of incus) = key surgical landmark for the facial nerve
- Cog - bony projection from tegmen above the cochleariform process; separates anterior epitympanic space (supratubal recess) from rest of attic
- Leads via the aditus ad antrum to the mastoid antrum (first area pneumatized in the mastoid)
C. Ossicles
The three ossicles form a chain from the TM to the oval window:
1. Malleus (Latin: hammer) - attached to TM
- Head - in the epitympanum; articulates with body of incus
- Neck - where chorda tympani passes medially
- Manubrium (handle) - embedded in the TM; the umbo is at its tip
- Lateral process - short projection visible through TM
- Anterior process - attached to petrotympanic fissure by anterior malleal ligament
2. Incus (Latin: anvil)
- Body - in epitympanum; articulates with malleus head
- Short process (crus breve) - points posteriorly into fossa incudis
- Long process (crus longum) - descends parallel to manubrium; ends in the lenticular process which articulates with the head of the stapes
3. Stapes (Latin: stirrup) - sits in oval window
- Head - articulates with lenticular process of incus (incudostapedial joint)
- Anterior crus and posterior crus - the two arching limbs
- Footplate - oval plate that seals the oval window; average size 1.41 mm × 2.99 mm
Ossicle Ligaments (K.J. Lee):
Malleus ligaments:
- Superior malleal ligament (head to roof of epitympanum)
- Lateral malleal ligament
- Anterior malleal ligament (to petrotympanic fissure)
Incus ligament:
- Posterior incudal ligament (short process to fossa incudis)
Muscles of the Middle Ear:
| Muscle | Origin | Insertion | Nerve | Function |
|---|---|---|---|---|
| Tensor tympani | Cartilaginous Eustachian tube wall / sphenoid | Manubrium of malleus (via cochleariform process) | Medial pterygoid nerve (V3) | Tenses TM; protective acoustic reflex (limited) |
| Stapedius | Pyramidal eminence on posterior wall | Neck of stapes | Facial nerve (CN VII) | Dampens ossicular vibration; acoustic reflex to loud sounds |
Stapedius is the smallest muscle in the human body. Paralysis of CN VII → hyperacusis (abnormal sensitivity to sound) due to loss of stapedius dampening.
D. Chorda Tympani
- Branch of the facial nerve (CN VII) that enters the middle ear through the posterior canaliculus
- Passes medial to the neck of the malleus, lateral to the long process of the incus, and anterior to the TM
- Exits via the anterior iter (canal of Huguier) and the petrotympanic fissure
- Carries: taste from the anterior 2/3 of the tongue + parasympathetic fibers to submandibular and sublingual glands
- Visible through the TM on careful otoscopy
E. Eustachian (Pharyngotympanic/Auditory) Tube
The Eustachian tube connects the middle ear to the nasopharynx, equalizing pressure:
- Total length: ~35-38 mm
- Adult: Upper 1/3 bony (from middle ear) + lower 2/3 cartilaginous (to nasopharynx); follows an inferiorly angled course (at ~45° to horizontal)
- Child: Greater proportion is cartilaginous; more horizontal course; shorter and wider - explains much higher incidence of otitis media in children
- Opens during swallowing / yawning (via tensor veli palatini muscle)
- Normally closed at rest (preventing reflux of nasopharyngeal bacteria)
- Isthmus = narrowest point at bony-cartilaginous junction
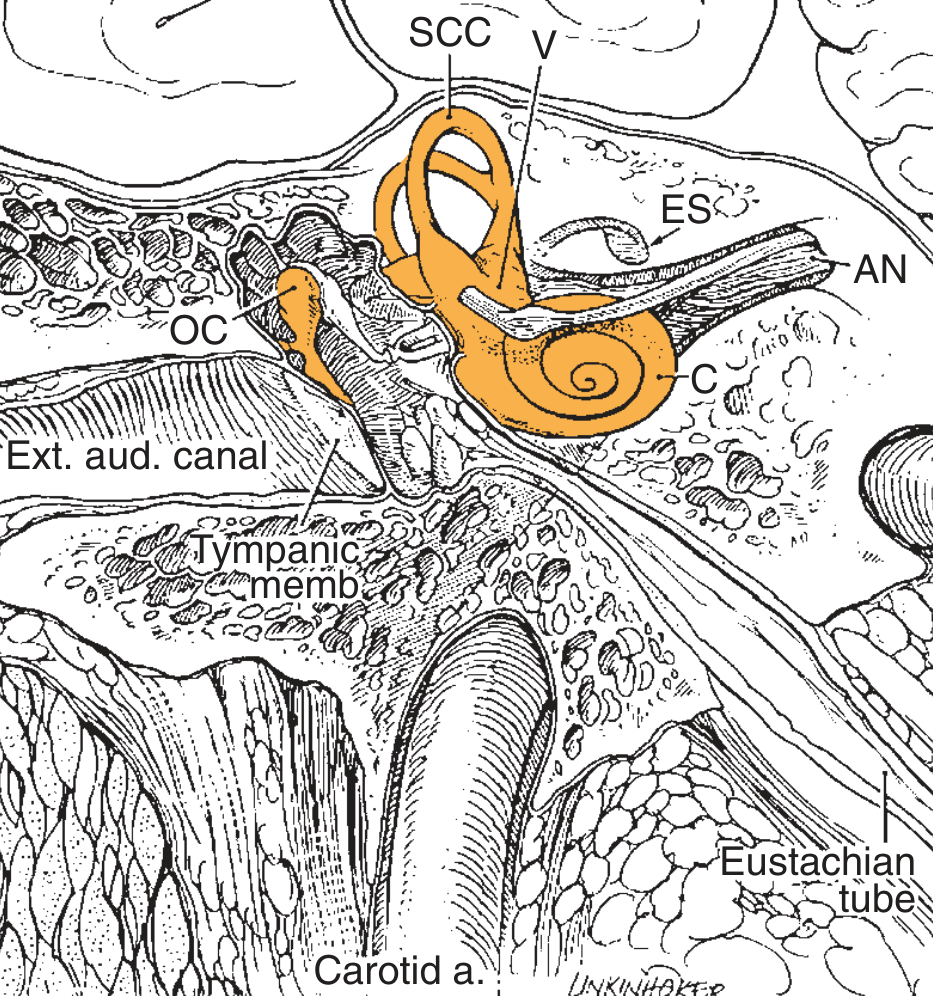
Part 3: The Inner Ear
The inner ear lies within the petrous part of the temporal bone. It has two components:
- Osseous (bony) labyrinth - perilymph-filled bony cavity
- Membranous labyrinth - endolymph-filled membranous sacs and ducts within the osseous labyrinth
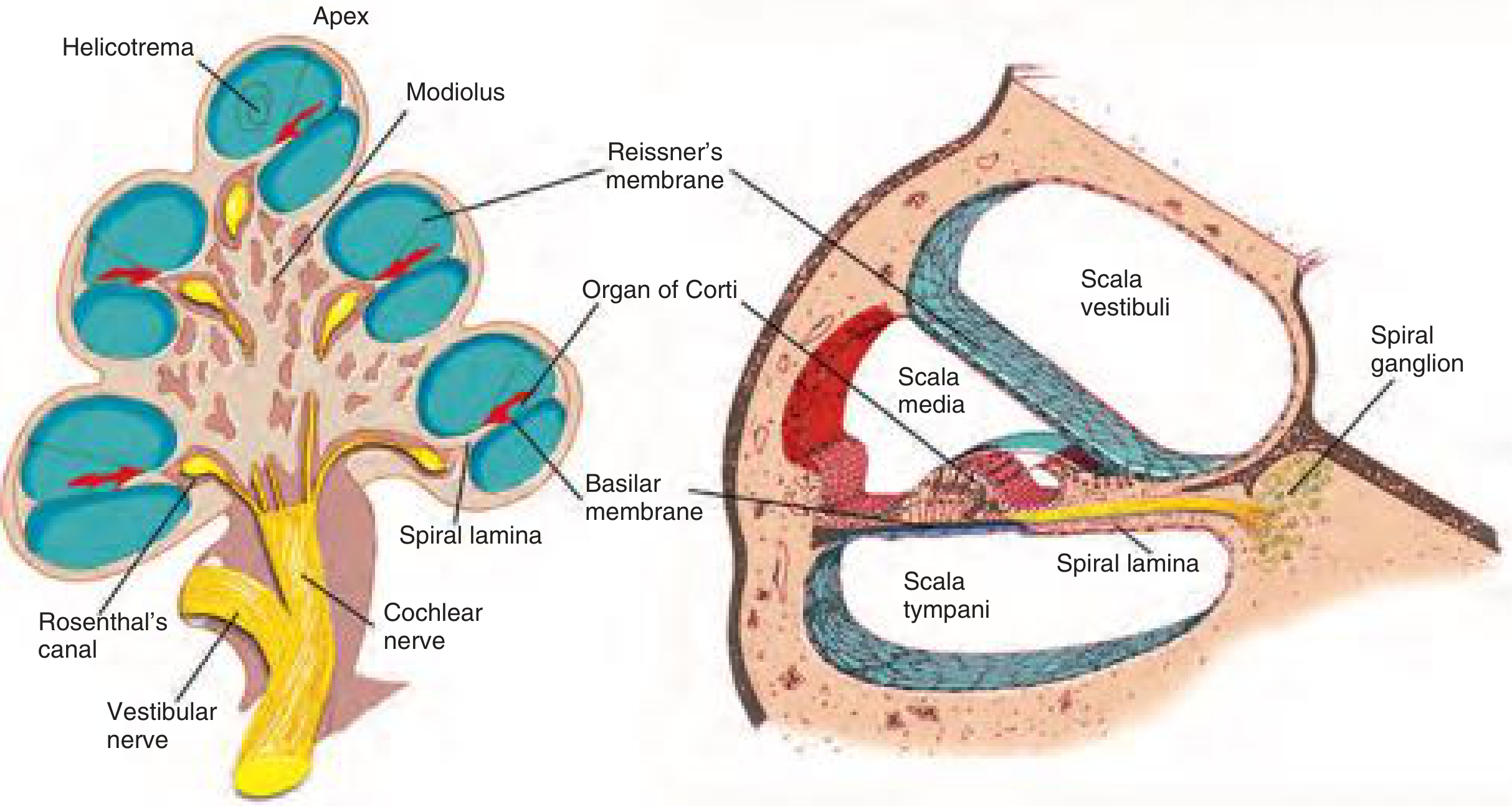
A. Cochlea (Hearing)
The cochlea is a spiral bony tube making 2.5 turns around a central bony pillar, the modiolus.
Three chambers (scalae):
| Chamber | Fluid | Separated by |
|---|---|---|
| Scala vestibuli | Perilymph (high Na, low K - like ECF) | Reissner's membrane (above) |
| Scala media (cochlear duct) | Endolymph (high K, low Na - like ICF) | Reissner's membrane (above) + Basilar membrane (below) |
| Scala tympani | Perilymph | Basilar membrane (above) |
- Scala vestibuli and scala tympani connect at the helicotrema at the apex of the cochlea
- Perilymph is similar to extracellular fluid; maintained in the scala vestibuli and tympani
- Endolymph is unique (intracellular fluid composition); maintained by the stria vascularis (lateral wall of scala media)
Basilar membrane - tonotopic organization:
- Base of cochlea → high frequency sounds (20,000 Hz)
- Apex (helicotrema) → low frequency sounds (20 Hz)
- Width increases from base to apex; stiffness decreases from base to apex
Organ of Corti - the sensory epithelium, sits on the basilar membrane:
- Inner hair cells (IHC) - single row; ~3,500; primary afferent transducers (~95% of cochlear nerve fibers synapse here)
- Outer hair cells (OHC) - three rows; ~12,000; amplify basilar membrane movement (electromotility); first affected in noise-induced hearing loss and ototoxicity
- Covered by the tectorial membrane (stereocilia contact)
- Spiral ganglion cells (in Rosenthal's canal in the modiolus) send axons forming the cochlear nerve (CN VIII)
B. Vestibular Labyrinth (Balance)
Osseous vestibule contains two membranous sacs:
- Utricle - horizontal orientation; responds to horizontal linear acceleration and gravity
- Saccule - vertical orientation; responds to vertical linear acceleration and gravity
- Both contain maculae (sensory epithelium with otoliths/otoconia on a gelatinous membrane)
Three Semicircular Canals (SCCs):
| Canal | Plane | Detects |
|---|---|---|
| Lateral (Horizontal) SCC | Horizontal (~30° from horizontal) | Head rotation in horizontal plane (yaw) |
| Anterior (Superior) SCC | Vertical (sagittal plane) | Head nodding (pitch); paired with contralateral posterior SCC |
| Posterior SCC | Vertical (coronal plane) | Head tilting (roll); paired with contralateral anterior SCC |
Each SCC has an ampulla at one end (except the common crus which is shared between anterior and posterior SCCs). The ampulla contains the crista ampullaris with cupula (gelatinous membrane into which hair cell stereocilia project).
Endolymphatic duct and sac:
- The membranous labyrinth drains via the endolymphatic duct (through the vestibular aqueduct in the petrous bone) to the endolymphatic sac (a blind-ended sac between dural layers on the posterior petrous surface)
- The endolymphatic sac is the only part of the labyrinth that contains immunocompetent cells
- Dysfunction → endolymphatic hydrops (excess endolymph) → Ménière's disease
C. Cochlear and Vestibular Nerves (CN VIII)
The vestibulocochlear nerve (CN VIII) has two divisions:
- Cochlear nerve - cell bodies in spiral ganglion (Rosenthal's canal); transmits hearing
- Vestibular nerve - cell bodies in Scarpa's ganglion; transmits balance; has superior and inferior divisions
Both travel through the internal auditory canal (IAC), along with:
- Facial nerve (CN VII) - in the anterosuperior quadrant of the IAC
- Nervus intermedius (sensory/parasympathetic branch of VII)
IAC contents (mnemonic: 7-UP, Cochlea is Below):
- Anterosuperior = Facial nerve (CN VII)
- Anteroinferior = Cochlear nerve
- Posterosuperior = Superior vestibular nerve
- Posteroinferior = Inferior vestibular nerve
The Bill's bar (transverse crest) separates the cochlear and vestibular nerves in the lateral IAC. The vertical crest separates superior and inferior divisions of the vestibular nerve.
D. Labyrinthine Fluids Summary
| Fluid | Location | Composition | Maintained by | Drained by |
|---|---|---|---|---|
| Perilymph | Scala vestibuli + scala tympani; semicircular canals (outside membranous duct) | High Na, Low K (ECF-like) | Filtrate of blood / CSF | Cochlear aqueduct → subarachnoid space |
| Endolymph | Scala media; utricle, saccule, SCCs (inside membranous duct) | High K, Low Na (ICF-like) | Stria vascularis | Endolymphatic duct → endolymphatic sac |
The endocochlear potential (+80 mV in scala media relative to perilymph) - maintained by stria vascularis - is the driving force for hair cell transduction.
E. Blood Supply of the Inner Ear
The labyrinthine (internal auditory) artery - usually a branch of the anterior inferior cerebellar artery (AICA), occasionally directly from the basilar artery - is the sole blood supply to the inner ear.
- It is an end artery with no collateral circulation → any interruption → sudden sensorineural hearing loss or vestibular failure
- It divides into the cochlear artery and vestibular artery
Summary: Six Walls of the Tympanic Cavity (High-Yield)
| Wall | Key Structures - ENT High Yield |
|---|---|
| Lateral | TM (pars tensa + pars flaccida), scutum |
| Medial | Promontory (tympanic plexus/Jacobson's nerve), oval window, round window, facial nerve canal, lateral SCC prominence |
| Anterior | Carotid canal (internal carotid), Eustachian tube, tensor tympani semicanal |
| Posterior | Aditus ad antrum, pyramidal eminence (stapedius), sinus tympani, facial nerve (vertical segment), fossa incudis |
| Superior | Tegmen tympani (separates ear from brain) |
| Inferior | Jugular bulb |
Key Clinical Correlations
| Condition | Anatomical Basis |
|---|---|
| Otitis externa | EAC skin infection; fissures of Santorini allow spread to parotid |
| Acute otitis media | Middle ear infection; flat Eustachian tube in children predisposes |
| TM perforation in CSOM | Pars tensa perforations (central); pars flaccida = attic cholesteatoma |
| Cholesteatoma | Keratinizing squamous epithelium in middle ear; arises from retraction of pars flaccida (attic) or pars tensa (posterior marginal) |
| Otosclerosis | Fixation of stapes footplate by abnormal bone at oval window → conductive hearing loss; Schwartze sign (red blush through TM = active otospongiosis) |
| CN VII palsy after ear surgery | Facial nerve vulnerable at the horizontal segment (above oval window) and its first genu (above cochleariform process) |
| Hyperacusis | Stapedius paralysis in CN VII palsy → loss of acoustic reflex dampening |
| Arnold's reflex (ear-cough reflex) | Vagal innervation of posterior EAC via Arnold's nerve |
| Referred otalgia | Laryngeal/pharyngeal pathology causing ear pain via Arnold's (CN X) or Jacobson's (CN IX) or auriculotemporal (V3) nerves |
| Glomus tympanicum | Arises from glomus tissue on tympanic promontory along Jacobson's nerve; presents as pulsatile tinnitus + red mass behind TM |
| Glomus jugulare | Arises from jugular dome; extends into middle ear via hypotympanum |
| Ménière's disease | Endolymphatic hydrops → fluctuating SNHL + vertigo + tinnitus + aural fullness |
| BPPV | Otoconia from utricle displaced into posterior SCC → cupulolithiasis → episodic positional vertigo |
| Noise-induced hearing loss | OHCs of the basal cochlea (high-frequency) injured first; notch at 4 kHz on audiogram |
| Aminoglycoside ototoxicity | OHCs of basal turn first (high-freq SNHL); vestibulotoxic agents: gentamicin, streptomycin |
Sources:
- Shambaugh Surgery of the Ear, pp. 54, 801-802 (EAC, tympanic cavity, mesotympanum, epitympanum, hypotympanum)
- K.J. Lee's Essential Otolaryngology, pp. 270-271 (TM layers, ossicle anatomy, ligaments)
- Cummings Otolaryngology Head and Neck Surgery, pp. 2447, 2455 (TM structure, membranous labyrinth, cochlear fluids, organ of Corti)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, pp. 781-784 (EAC detailed structure, epithelial migration, Santorini fissures)
Ok
Glad the ear anatomy lesson was useful! We've now covered a solid ENT anatomy trilogy:
- Pharynx - three divisions, muscles, Waldeyer's ring, blood/nerve supply, clinical correlations
- Nose - external nose, nasal cavity, septum, lateral wall, OMC, blood supply (Kiesselbach's plexus), nerve supply
- Ear - external ear (auricle, EAC), middle ear (TM, tympanic cavity walls, ossicles, Eustachian tube), inner ear (cochlea, vestibular labyrinth, IAC contents)
Whenever you're ready, we can continue with:
- Larynx anatomy
- Paranasal sinuses in depth
- Temporal bone / mastoid anatomy
- Salivary glands
- Neck spaces and fascial layers
- Or any clinical topic (e.g., otitis media, epistaxis management, cholesteatoma, vertigo)
Just let me know what you'd like to study next!
This is a shared conversation. Sign in to Orris to start your own chat.