Psychedelics as a potential treatment for borderline personality disorder: A narrative review
Reading File
Finding Sources
Searching PubMed
psychedelics AND "borderline personality disorder"
Searching the Web
psychedelics treatment borderline personality disorder clinical trial 2024 2025 2026
Reading Article
PMID: 41955843
Reading Article
PMID: 37200873
Reading Article
PMID: 40293802
Reading Article
PMID: 38574699
Reading File
Reading File
Finding Sources
Searching PubMed
psilocybin MDMA "personality disorder" OR "emotional dysregulation" mechanism
Reading Web Page
https://isha.health/post/psychedelics-borderline-personality…
Reading File
Reading File
Finding Sources
Searching PubMed
ketamine esketamine "borderline personality disorder" safety efficacy
Reading File
Finding Sources
Finding Sources
Searching PubMed
psilocybin neuroplasticity BDNF emotional regulation depression
Loading Image
Psychedelics as a Potential Treatment for Borderline Personality Disorder: A Narrative Review
Abstract
Borderline personality disorder (BPD) is a serious mental illness with high rates of morbidity, mortality, and stigma, yet successful remission is frequently limited by a paucity of accessible treatment options. In an era of growing interest in psychedelics as novel psychiatric treatment modalities, patients with BPD are often excluded from research due to perceived safety risks - particularly pertaining to suicide and substance misuse. However, there is evolving evidence that psychedelic treatment may effectively target core BPD symptoms, as well as those of the mood and anxiety disorders frequently comorbid with BPD. The most recent and comprehensive narrative review on this topic, published in Psychiatry Research (July 2026), examined 22 studies involving ketamine, esketamine, and psilocybin, finding preliminary evidence of safety and efficacy in this population while calling for rigorously designed clinical trials with BPD-specific outcome measures.
1. Introduction
BPD is characterized by a pervasive pattern of instability in interpersonal relationships, self-image, and affect, combined with marked impulsivity. As defined in DSM-5 and extensively detailed in Kaplan & Sadock's Synopsis of Psychiatry, core features distinguishing BPD from mood disorders include fear of abandonment, highly unpredictable behavior, tumultuous interpersonal relationships, dichotomous ("all-or-nothing") thinking about others, chronic feelings of emptiness, and the lack of a consistent sense of identity. BPD differs from schizophrenia by the absence of prolonged psychotic episodes and thought disorder, and from histrionic personality disorder by the greater prominence of suicide attempts and identity diffusion. - Kaplan and Sadock's Synopsis of Psychiatry, p. 1699-1700
The condition carries a lifetime prevalence of approximately 1-2% in the general population, but accounts for 10-20% of psychiatric inpatient admissions. Morbidity is considerable: individuals with BPD are at heightened risk for major depression, PTSD, substance use disorders, eating disorders (notably bulimia), ADHD, and somatic symptom disorder. Suicide rates are estimated at 8-10%, with far higher rates of parasuicidal and self-injurious behavior. - Kaplan and Sadock's Synopsis of Psychiatry, p. 1702
Despite this burden, pharmacological options remain largely symptomatic. No medication carries FDA approval specifically for BPD. Clinicians use SSRIs, mood stabilizers (lithium, lamotrigine, valproate), and low-dose atypical antipsychotics off-label to manage specific symptom clusters such as emotional lability, impulsive aggression, and cognitive-perceptual distortions, with modest and heterogeneous results. The mainstay of treatment is psychotherapy - specifically dialectical behavior therapy (DBT), which targets suicidality, self-harm, and emotional dysregulation - but DBT requires sustained engagement over months to years, many patients drop out before completing a full course, and access remains limited worldwide. - Kaplan and Sadock's Synopsis of Psychiatry, pp. 1710-1712
These unmet needs create a compelling rationale for exploring novel pharmacological approaches, including psychedelic-assisted therapies.
2. Neurobiology of BPD: Why Psychedelics Are Theoretically Relevant
The biological underpinnings of BPD converge on several pathways that psychedelics are known to modulate:
Serotonergic dysregulation. BPD is associated with altered serotonin signaling, evidenced by elevated monoamine oxidase-A (MAO-A) distribution volume across prefrontal, anterior cingulate, and striatal regions, which correlates with severity of mood symptoms, suicidality, and cognition. The Kolla et al. (2016) Biol Psychiatry study demonstrated that this excess MAO-A activity may underpin the characteristic affective instability of BPD - a directly relevant target for serotonergic psychedelics.
Glutamatergic dysfunction and impaired neuroplasticity. Disrupted prefrontal-limbic connectivity, hyperreactive amygdalar responses, and impaired top-down emotional regulation are well documented in BPD neuroimaging studies. Reduced BDNF levels and impaired synaptic plasticity in frontolimbic circuits contribute to the chronic, treatment-resistant nature of the condition.
Trauma and PTSD overlap. A very high proportion of BPD patients have histories of childhood trauma, abuse, or neglect, and BPD and PTSD frequently co-occur. The dissociative symptoms, hypervigilance, and traumatic memory re-experiencing that overlap between the two conditions provide a mechanistic entry point for psychedelic-assisted trauma processing.
Rigid self-concept and identity disturbance. A core BPD feature is the absence of a stable, coherent sense of self. Psychedelics, particularly in the context of a mystical or "ego-dissolving" experience, have been theorized to disrupt rigid maladaptive self-referential thinking patterns.
3. Pharmacological Mechanisms of Candidate Psychedelics
3.1 Classic Serotonergic Hallucinogens (Psilocybin, LSD)
The primary mechanism of hallucinogens such as psilocybin (converted to psilocin in vivo), LSD, and mescaline is agonism at 5-HT2A receptors (see diagram below). These drugs may also have additional activity at other serotonin receptor subtypes.
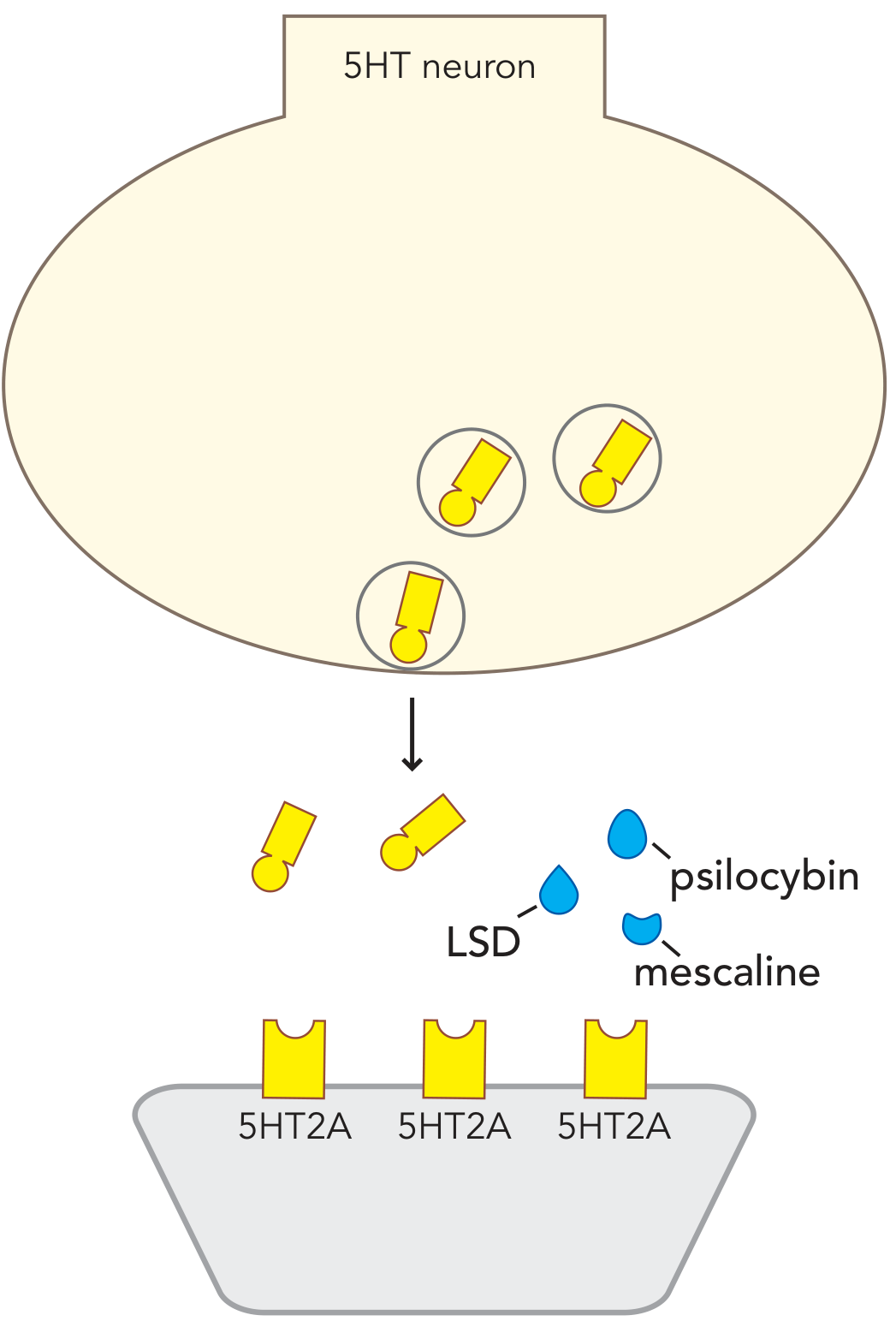
5-HT2A activation in the prefrontal cortex produces altered states of consciousness described as psychedelic - feelings of expanded sensory awareness, union with the universe, and emotional openness - distinct from the psychotomimetic effects of stimulants or PCP. Psilocybin-assisted psychotherapy is currently under investigation across treatment-resistant depression, OCD, addiction, cluster headaches, and a broadening list of conditions. Whether the psychological state or the direct pharmacology drives therapeutic outcomes remains an open question, as does whether neuroplastic changes analogous to those seen with ketamine are triggered via 5-HT2A. - Stahl's Essential Psychopharmacology, Neuroscientific Basis
3.2 MDMA (Empathogen/Entactogen)
MDMA is pharmacologically distinct from classic psychedelics. It is a synthetic amphetamine derivative that acts selectively on the serotonin transporter (SERT) as a competitive inhibitor and pseudosubstrate, promoting massive serotonin release and inhibiting reuptake, with lesser effects on norepinephrine and dopamine transporters. The resulting state is one of emotional openness, empathy, and a sense of relatedness - properties that make it particularly suited to trauma-focused psychotherapy. MDMA does not typically produce the hallucinatory perceptual distortions of psilocybin. - Stahl's Essential Psychopharmacology, Neuroscientific Basis
The idea behind MDMA-assisted psychotherapy (MDMA-AP) in BPD is that the empathic, emotionally open state it produces may render patients more able to explore painful traumatic memories alongside a therapist, facilitating reconsolidation of fearful memories in a new emotional context. MDMA has been most studied in PTSD, where it is posited to provide a "safe psychological window" for self-directed exploration of trauma. Given the profound overlap between PTSD and BPD in symptom profile and traumatic background, MDMA-AP is considered a plausible candidate.
3.3 Ketamine and Esketamine
Ketamine is an NMDA receptor antagonist and dissociative agent with rapid-acting antidepressant properties. It promotes prefrontal neural plasticity (likely via BDNF and AMPA receptor upregulation) and facilitates top-down executive control over limbic reactivity. Intranasal esketamine (Spravato) is FDA-approved for treatment-resistant depression and major depressive disorder with acute suicidal ideation. Ketamine is also being investigated for substance use disorders, where promoting prefrontal neuroplasticity may reverse drug-related shifts in neural control. - Stahl's Essential Psychopharmacology, Neuroscientific Basis
Ketamine is of particular interest in BPD for several reasons: (1) it acts rapidly on suicidal ideation, a hallmark BPD symptom; (2) it targets glutamatergic dysregulation in frontolimbic circuits; and (3) its neuroplastic effects may durably modify the maladaptive neural patterns underlying emotional dysregulation and impulsivity.
4. Existing Evidence: What Has Been Studied?
4.1 The Artna et al. (2026) Narrative Review
The most definitive synthesis to date is by Artna E, Sandhu G, Chisamore N, et al., "Psychedelics as a potential treatment for borderline personality disorder: A narrative review," published in Psychiatry Research, Volume 361, July 2026 (PMID: 41955843). This review, sourced from Ovid MEDLINE, PsychInfo, and Embase, included 22 studies examining ketamine, esketamine, and psilocybin in patients with BPD or BPD features. Key findings:
- Preliminary evidence supports safety and some efficacy for improvement in core BPD symptoms (emotional dysregulation, suicidal ideation) and socio-occupational functioning
- Across all compounds, no evidence of increased risk compared to non-BPD populations when treatment was delivered in controlled, supervised settings
- The included studies were heterogeneous in design (case reports, open-label trials, RCTs not focused on BPD), and almost none used BPD-specific primary outcome measures
- The reviewers concluded that "further high-quality evidence focusing on BPD-specific outcomes is needed"
4.2 MDMA-Assisted Psychotherapy: Theoretical Framework
Traynor JM, Roberts DE, Ross S, Zeifman R, Choi-Kain L (2022) in Focus (Am Psychiatr Publ) provided the first systematic theoretical framework for MDMA-AP in BPD. The authors argued that MDMA's promise in overlapping conditions (particularly PTSD) provides a plausible mechanistic rationale. They proposed initial treatment targets (emotional dysregulation, identity disturbance, interpersonal hyperreactivity) and hypothesized mechanisms of change, and laid out considerations for designing MDMA-AP clinical trials in BPD - notably addressing the high dropout rates and treatment heterogeneity that plague current BPD trials. (PMID: 37200873)
4.3 Ketamine-Assisted Psychotherapy: Case Evidence
Yeung A, Alpert M, Mischoulon D (2025) reported the first published case study of ketamine-assisted psychotherapy (KAP) in a patient with co-occurring BPD and depression, published in the Journal of Personality Disorders. KAP utilized both the antidepressant and dissociative/psychedelic effects of ketamine embedded within a psychotherapy framework, emphasizing the concept of an "inner healing intelligence" and the intersubjective therapeutic relationship. Positive outcomes were observed, and the authors called for more systematic research. (PMID: 40293802)
4.4 Broader Psychedelic Efficacy: Systematic Review Evidence
The most rigorous broader analysis is the Yao Y, Guo D, Lu TS, et al. (2024) systematic review and meta-analysis in Psychiatry Research, which included 126 articles and found that psilocybin demonstrated the strongest therapeutic effect across mental disorders (Hedges' g = -1.49, 95% CI [-1.67, -1.30]), followed by ayahuasca, MDMA, and LSD. Importantly, the review explicitly noted that "a small amount of evidence also supports psychedelics improving...borderline personality disorder," alongside OCD, eating disorders, and body dysmorphic disorder. (PMID: 38574699)
5. Mechanistic Rationale for BPD-Specific Targets
| BPD Core Domain | Proposed Psychedelic Mechanism |
|---|---|
| Emotional dysregulation / affective instability | 5-HT2A agonism (psilocybin); SERT-mediated serotonin surge (MDMA); glutamate/NMDA plasticity (ketamine) |
| Impulsivity | Prefrontal neuroplasticity and BDNF upregulation (ketamine); enhanced top-down PFC control |
| Unstable identity / rigid self-concept | Ego dissolution during psychedelic state may disrupt rigid self-referential patterns; increased cognitive and psychological flexibility |
| Trauma processing / PTSD overlap | MDMA-induced emotional openness for trauma reprocessing; reconsolidation disruption via hallucinogens/dissociatives |
| Interpersonal hyperreactivity | Empathic state induced by MDMA; enhanced therapeutic alliance during psilocybin therapy |
| Chronic suicidal ideation | Rapid anti-suicidal effects of ketamine/esketamine (FDA-approved for MDD with ASID) |
| Dissociation | Complex: ketamine's dissociative mechanism is both a potential tool and a risk given existing BPD dissociative symptoms |
As noted in Stahl's Essential Psychopharmacology: "hallucinogens, dissociatives, and entactogens such as psilocybin, MDMA, and ketamine have been employed in an attempt to block reconsolidation of activated memories during psychotherapy" - a mechanism directly applicable to the trauma-laden narratives common in BPD.
6. Safety Considerations
BPD patients have historically been excluded from psychedelic research due to three primary safety concerns:
-
Suicidal ideation and self-harm. The risk of psychedelic-induced psychological distress precipitating suicidal crisis is the most-cited concern. However, ketamine's rapid anti-suicidal properties represent a potential advantage rather than a liability, and the Artna et al. review found no evidence of worsened suicidal outcomes across included studies under controlled conditions.
-
Substance use comorbidity. Rates of substance use disorders (SUD) are elevated in BPD (reported in up to 65% of patients in some series). Most psychedelic trials exclude active SUD, limiting generalizability. However, ketamine is itself being studied specifically for addiction disorders, complicating this calculus.
-
Dissociation. Many BPD patients experience chronic dissociative symptoms. The dissociative effects of ketamine and the depersonalization possible with classic psychedelics could theoretically destabilize patients. The Artna review found that dissociative side effects were not more frequent or severe in BPD patients than in controls when delivered in supervised settings, but careful screening and monitoring are essential.
-
Psychosis risk. BPD is associated with brief stress-induced psychotic episodes. Classic psychedelics can produce psychotomimetic experiences, and the risk of precipitating or prolonging psychotic states requires careful attention. Patients with prominent psychotic features should likely be excluded.
-
Emotional intensity and re-traumatization. The emotional amplification characteristic of psychedelic states may be more intense and less predictable in patients with severe affect dysregulation. "Set, setting, and cast" - the mindset of the patient, the therapeutic environment, and the presence of a trained therapist - are considered critical variables in determining whether the psychedelic experience is therapeutic or harmful. - Stahl's Essential Psychopharmacology, Neuroscientific Basis
7. Current Treatment Landscape and Context
Standard pharmacotherapy in BPD is symptom-targeted and off-label:
- Emotional lability / rapid cycling: lithium, lamotrigine, valproate, low-dose antipsychotics (olanzapine, aripiprazole, clozapine)
- Affective aggression: SSRIs, anticonvulsants, low-dose antipsychotics
- Cognitive-perceptual distortions / brief psychosis: novel antipsychotics
- Benzodiazepines are generally contraindicated due to disinhibition risk
DBT remains the gold-standard psychosocial treatment with the most empirical support, targeting suicidality, self-harm, interpersonal effectiveness, and emotional regulation through a combination of individual therapy, skills group, phone coaching, and therapist consultation team. - Kaplan and Sadock's Synopsis of Psychiatry, pp. 1711-1712
Psychedelic-assisted therapies, if proven effective, would not replace DBT but could potentially accelerate its effects, address treatment-resistant cases, or reach patients who cannot access or sustain DBT.
8. Gaps, Limitations, and Future Directions
Several limitations constrain the current evidence base:
- No RCTs have been designed specifically for BPD as the primary indication for any psychedelic compound. All available data are either indirect (from trials that incidentally included patients with BPD features) or observational/case-based.
- BPD-specific outcome measures (e.g., Zanarini Rating Scale for BPD [ZAN-BPD], McLean Screening Instrument, MSI-BPD) are rarely used as primary endpoints. Most studies use generic depression, anxiety, or PTSD scales that do not capture the full BPD symptom constellation.
- Selection bias from exclusion criteria. The very practices that have excluded BPD patients from trials - concerns about suicide, SUD, and emotional instability - have left a research void that mirrors the clinical experience of treating this population.
- Heterogeneity of study designs. The 22 studies in the Artna review span case reports, open-label pilots, and RCTs in comorbid conditions, making any pooled conclusions methodologically challenging.
- Dissociation as a double-edged variable. Whether dissociative side effects in BPD represent a therapeutic window or a risk factor remains unresolved and will require careful sub-group analysis.
Priority recommendations for future research:
- Phase II RCTs with BPD as the primary indication, using BPD-validated outcome tools (ZAN-BPD, STEPPS scales)
- MDMA-AP trials combining trauma-focused therapy protocols adapted for BPD (e.g., MDMA augmentation of DBT)
- Ketamine/esketamine safety and dose-finding studies in BPD with concurrent suicidal ideation
- Neuroimaging biomarker studies examining whether psychedelics normalize frontolimbic dysconnectivity in BPD
- Longitudinal studies addressing durability of response and impact on functional outcomes
9. Conclusion
Psychedelic-assisted therapies - particularly ketamine, esketamine, psilocybin, and MDMA - represent a theoretically compelling and biologically plausible avenue for treating BPD. Their mechanisms (5-HT2A agonism, SERT-mediated serotonin release, NMDA antagonism, neuroplasticity induction, trauma memory reconsolidation) map onto the core neurobiological vulnerabilities of BPD: serotonergic dysregulation, impaired prefrontal-limbic connectivity, rigid maladaptive self-concepts, and unresolved trauma.
The landmark 2026 narrative review by Artna et al. synthesized 22 studies and found no signal of excess harm under controlled conditions, alongside preliminary evidence of benefit for emotional dysregulation, suicidal ideation, and socio-occupational functioning. The broader literature, including the Yao et al. (2024) meta-analysis and the Traynor et al. (2022) MDMA-AP framework, provides additional scaffolding. However, the evidence base remains preliminary. Carefully designed, BPD-specific RCTs with validated outcome measures are the essential next step before psychedelic-assisted therapy can be recommended for clinical use in this population.
Key References
| Citation | Study Type | Key Finding |
|---|---|---|
| Artna E et al., Psychiatry Res, 2026 (PMID: 41955843) | Narrative Review | 22 studies; preliminary evidence for safety and efficacy of ketamine, esketamine, psilocybin in BPD |
| Yao Y et al., Psychiatry Res, 2024 (PMID: 38574699) | Systematic Review & Meta-Analysis | Psilocybin strongest effect (g = -1.49) across mental disorders; small evidence for BPD benefit |
| Traynor JM et al., Focus, 2022 (PMID: 37200873) | Review | Theoretical rationale and clinical trial design considerations for MDMA-AP in BPD |
| Yeung A et al., J Pers Disord, 2025 (PMID: 40293802) | Case Report | First published case of KAP in co-occurring BPD and depression; positive outcomes |
| Kolla NJ et al., Biol Psychiatry, 2016 (PMID: 25698585) | Cohort Study | Elevated MAO-A in BPD correlates with mood severity and suicidality; serotonergic target rationale |
| Kaplan & Sadock's Synopsis of Psychiatry | Textbook | BPD diagnosis, differential, pharmacotherapy, and DBT |
| Stahl's Essential Psychopharmacology | Textbook | Mechanisms of psilocybin (5-HT2A), MDMA (SERT), ketamine (NMDA); psychedelic-assisted psychotherapy |
Disclosure note: The current evidence is preliminary. Psychedelic-assisted therapy for BPD is not an approved or standard-of-care intervention. All cited studies were conducted in supervised clinical settings by trained providers. Patients with BPD considering these approaches should be directed to evidence-based treatments (primarily DBT) while research matures.
This is a shared conversation. Sign in to Orris to start your own chat.