Give an cardio-respiratory changes occur during isotonic exercise
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
Cardiorespiratory Changes During Isotonic Exercise
Isotonic exercise (dynamic/rhythmic exercise - e.g., running, cycling) involves repeated muscle shortening with external work. It produces a distinct and coordinated cardiovascular and respiratory response that differs significantly from isometric exercise.
CARDIOVASCULAR CHANGES
1. Heart Rate (HR)
- Increases promptly at onset of exercise - even before metabolic changes occur
- Initial rise is largely due to decreased vagal (parasympathetic) tone; later, increased sympathetic discharge contributes
- Maximal HR: up to 200+ beats/min in children, rarely exceeds 195 beats/min in adults, and is lower in the elderly
- Trained athletes have a lower resting and exercise HR for any given workload due to larger stroke volume
2. Stroke Volume (SV)
- Markedly increased - this is the key feature distinguishing isotonic from isometric exercise
- Increased by:
- Enhanced myocardial contractility via sympathetic (β₁) stimulation
- Greater venous return (Frank-Starling mechanism)
- Venoconstriction (noradrenergic) reducing venous pooling
- Represented by an increased pulse pressure (Costanzo)
3. Cardiac Output (CO)
- CO = HR × SV; both components increase, driving CO to very high levels
- Can exceed 35 L/min during strenuous isotonic exercise (resting ~5 L/min)
- Increase is directly proportional to the rise in O₂ consumption
- In trained athletes, maximal CO is higher; VO₂max averages ~38 mL/kg/min in active men, ~29 mL/kg/min in active women
- Ganong's Review of Medical Physiology, 26th Ed.
4. Blood Pressure
- Systolic BP rises moderately (increased CO)
- Diastolic BP remains unchanged or falls - due to net fall in total peripheral resistance from vasodilation in exercising muscle
- This contrasts with isometric exercise where both systolic AND diastolic BP rise sharply
- After exercise, BP may transiently drop below baseline as residual metabolites keep muscle vessels dilated
5. Total Peripheral Resistance (TPR)
- Net fall in TPR - this is the hallmark of isotonic exercise
- Results from massive vasodilation in actively contracting skeletal muscle
- Locally mediated by: ↓tissue PO₂, ↑tissue PCO₂, accumulation of K⁺ and other vasodilator metabolites, local temperature rise
- 10- to 100-fold increase in the number of open capillaries in exercising muscle
6. Blood Flow Redistribution
Selective sympathetic arteriolar vasoconstriction occurs in:
- Skin, splanchnic regions, kidneys, and inactive muscles (α₁ receptors → ↑resistance, ↓flow)
While vasodilation occurs in:
- Exercising skeletal muscle (local metabolic override of sympathetic tone)
- Coronary circulation (↑O₂ demand)
- Cerebral circulation (maintained throughout)
- Skin (late - biphasic response: initial vasoconstriction, then vasodilation for heat dissipation as body temperature rises)
Costanzo Physiology, 7th Ed.
7. Venous Return
- Greatly increased, enabling the rise in cardiac output
- Mechanisms:
- Muscle pump - rhythmic skeletal muscle contractions squeeze veins
- Thoracic (respiratory) pump - increased breathing depth creates greater negative intrathoracic pressure
- Mobilization of blood from splanchnic reservoirs (increases arterial blood volume by ~30%)
- Noradrenergic venoconstriction reduces venous capacitance
- Ganong's Review of Medical Physiology, 26th Ed.
RESPIRATORY CHANGES
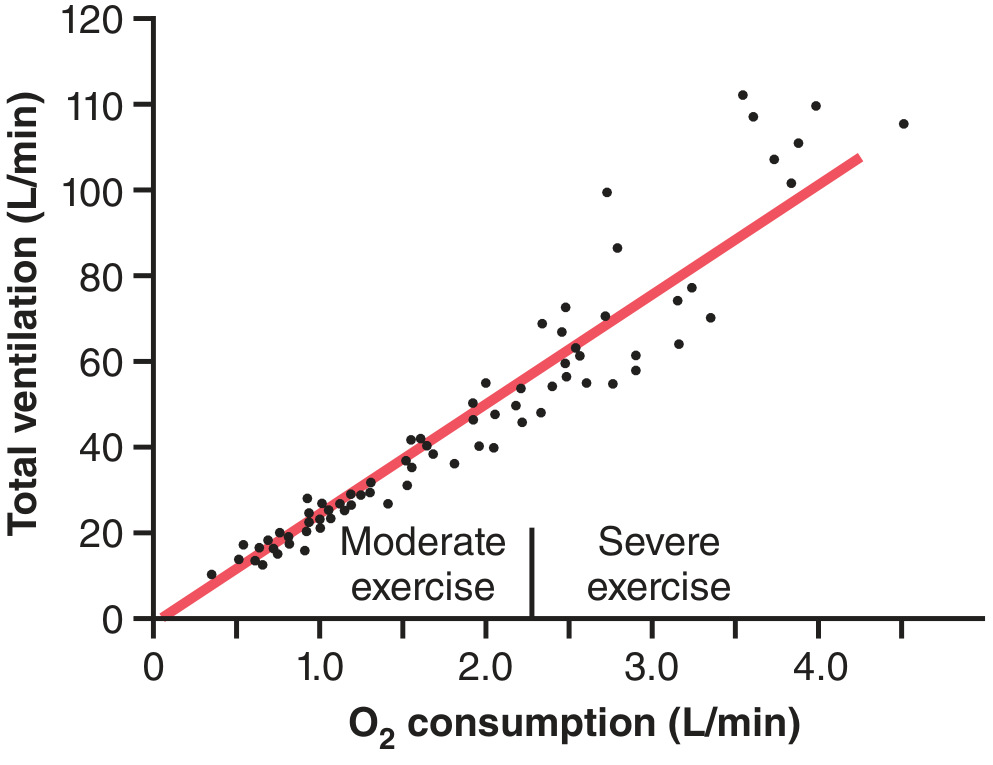
1. Ventilation (Minute Ventilation, V̇E)
- Increases dramatically and nearly linearly with O₂ consumption (and CO₂ production) during moderate exercise
- Can rise from a resting ~6 L/min to >100 L/min during heavy exercise
- Two phases:
- Immediate (neurogenic) phase: rapid increase at the very onset of exercise - before any blood gas changes - driven by central command from the cerebral motor cortex and signals from muscle mechanoreceptors
- Chemical phase (30-40 seconds in): CO₂ released from active muscles matches the increased ventilation, and arterial PCO₂ returns to normal
2. Arterial Blood Gases
- PaO₂: remains essentially normal during moderate isotonic exercise
- PaCO₂: initially falls slightly (over-ventilation from central command), then returns to ~40 mmHg as CO₂ output from muscles rises to match ventilation
- pH: maintained near normal during moderate exercise; falls (lactic acidosis) during severe exercise beyond the anaerobic threshold
- Key point: arterial blood gases do NOT change significantly during moderate exercise, confirming that the primary driver is neurogenic, not chemical
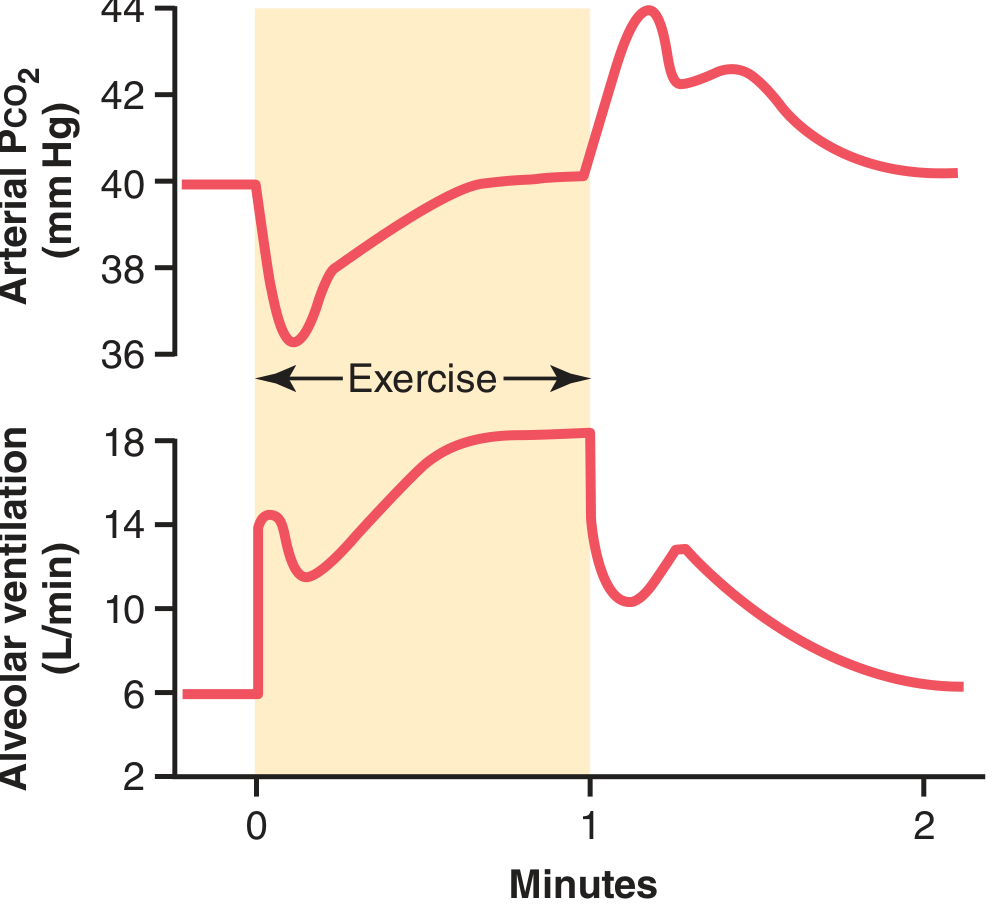
The figure above shows: at exercise onset, alveolar ventilation jumps immediately (neurogenic anticipatory drive), causing PCO₂ to drop briefly. Within ~30-40 seconds, PCO₂ returns to 40 mmHg as the two processes balance.
3. Mechanism of Ventilatory Control During Exercise
- Central command: cerebral motor cortex sends parallel signals to muscles AND to the brain stem respiratory center - explains the "anticipatory" increase in ventilation
- Proprioceptive input: muscle and joint mechanoreceptors send afferent signals to the respiratory center
- Chemical fine-tuning: peripheral chemoreceptors (for PO₂, PCO₂, H⁺) make final adjustments
- The neurogenic shift of the PCO₂-ventilation response curve is ~20-fold upward during heavy exercise, keeping arterial PCO₂ near 40 mmHg throughout
- This neurogenic response is partly learned - cerebral cortex involvement allows progressive adaptation with training
Guyton and Hall Textbook of Medical Physiology
4. Oxygen Consumption (VO₂)
- Rises in proportion to exercise intensity
- Skeletal muscle O₂ extraction increases (widened arteriovenous O₂ difference)
- VO₂max represents the ceiling and is the product of maximal CO × maximal tissue O₂ extraction - both increase with training
KEY COMPARISON: Isotonic vs. Isometric Exercise
| Parameter | Isotonic | Isometric |
|---|---|---|
| Heart rate | ↑↑ | ↑ |
| Stroke volume | ↑↑ (marked) | Minimal change |
| Cardiac output | ↑↑↑ (up to 35+ L/min) | Modest increase |
| Systolic BP | Moderate ↑ | Sharp ↑ |
| Diastolic BP | Unchanged or ↓ | Sharp ↑ |
| TPR | ↓ (net fall) | ↑ (net rise) |
| Muscle blood flow | ↑ (between contractions) | ↓ (vessels compressed) |
Sources:
- Ganong's Review of Medical Physiology, 26th Ed. - "Circulatory Changes during Exercise"
- Guyton and Hall Textbook of Medical Physiology - "Regulation of Respiration During Exercise"
- Costanzo Physiology, 7th Ed. - "Central Command" and "Overall Responses to Exercise"
This is a shared conversation. Sign in to Orris to start your own chat.