Femoral,Umbilical and para Umbilical hernia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive content from Bailey & Love and S. Das to compile a thorough answer. Let me compile the full response.
Femoral, Umbilical, and Para-Umbilical Hernia
FEMORAL HERNIA
Definition & Anatomy
A femoral hernia is a protrusion of extraperitoneal tissue, peritoneum, and sometimes abdominal contents through the femoral canal.
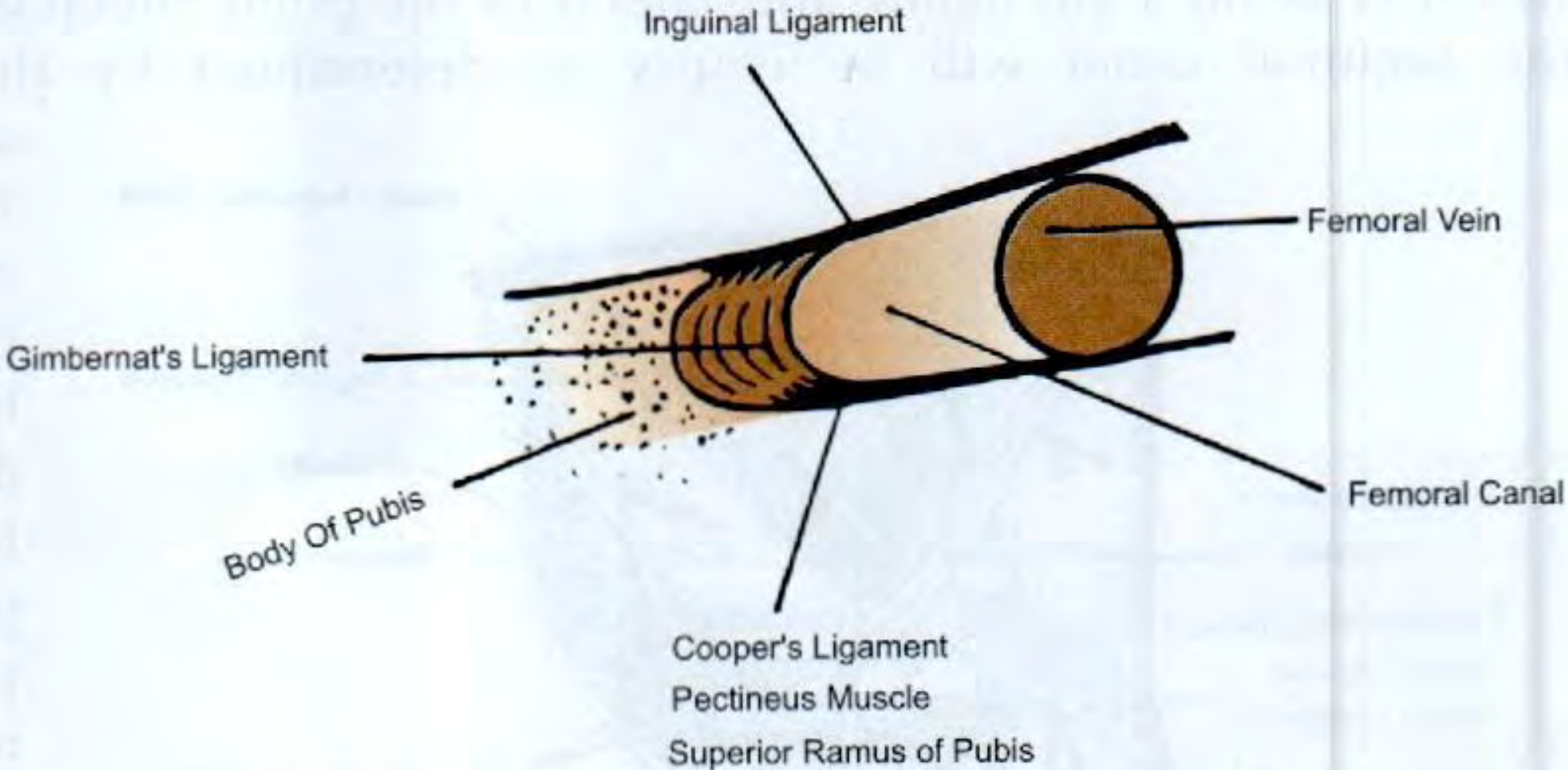
Boundaries of the femoral canal:
| Wall | Structure |
|---|---|
| Anterior | Inguinal ligament |
| Posterior | Pubic ramus, pectineus muscle; iliopectineal (Cooper's/Astley Cooper's) ligament |
| Medial | Lacunar (Gimbernat's) ligament — strong, curved, with a sharp unyielding edge |
| Lateral | Femoral vein |
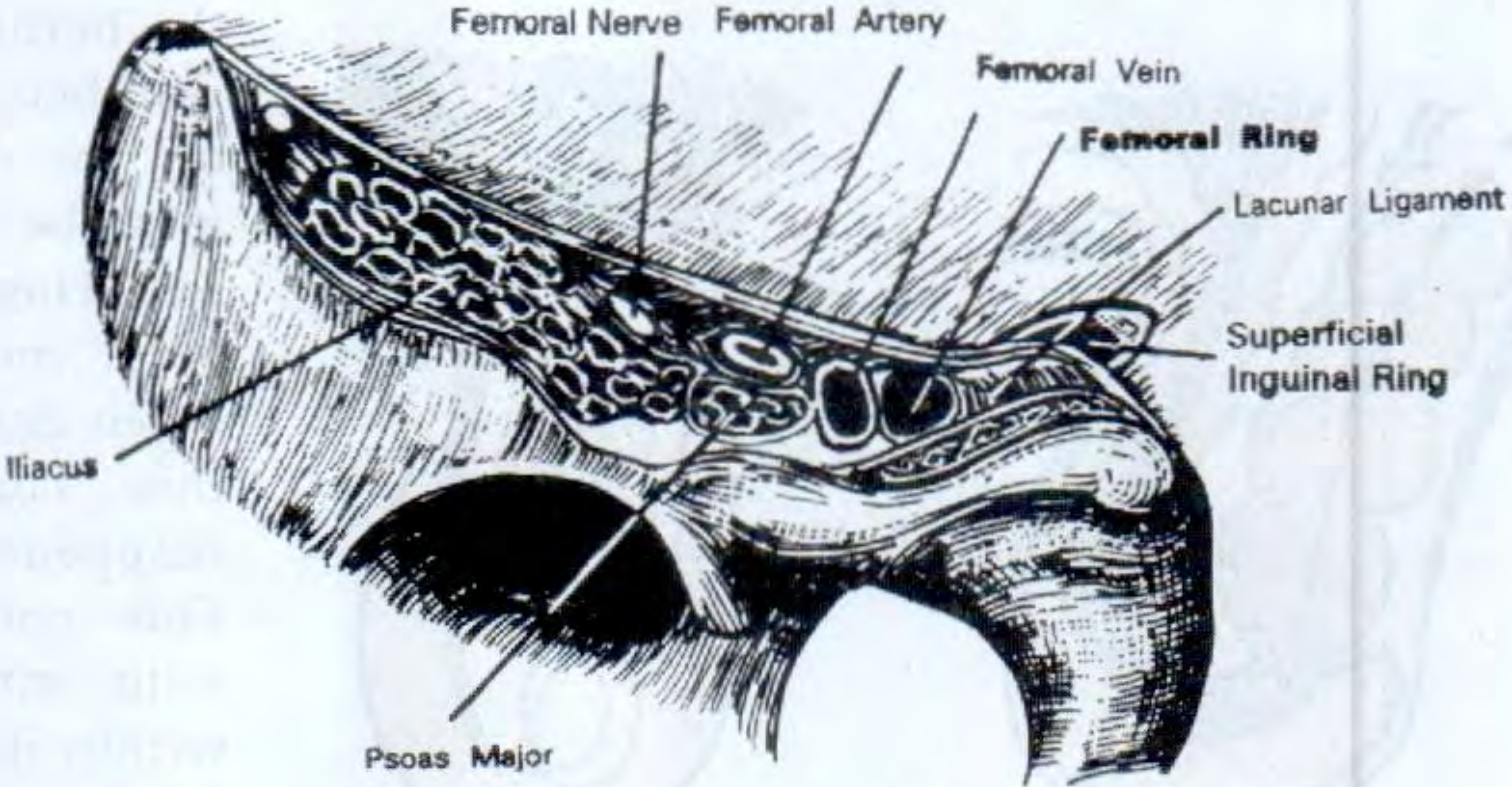
The hernia exits superficially through the saphenous opening, located 1½ inches (≈4 cm) below and lateral to the pubic tubercle. Within the rigid canal the sac remains narrow; once through the saphenous opening, it expands into a retort shape, with the bulbous end sometimes extending above the inguinal ligament.
Epidemiology
- Rare before age 20; peak incidence >50 years
- Commoner in women (2:1) — the female pelvis widens the femoral canal — but inguinal hernia is still the commonest groin hernia even in women
- Right side twice as common as left; 20% bilateral
- The rigid canal means strangulation is common (~50% present as emergencies)
Clinical Features & Diagnosis
- Swelling below and lateral to the pubic tubercle, below the inguinal ligament
- Often only 1–2 cm; easily mistaken for a lymph node
- Rapidly becomes irreducible; cough impulse may be absent due to tight neck
- In late stages, may reflect superiorly and mimic a direct inguinal hernia
Distinguishing femoral from inguinal hernia:
| Feature | Femoral Hernia | Inguinal Hernia |
|---|---|---|
| Position relative to pubic tubercle | Lateral | Medial |
| Position relative to inguinal ligament | Below (may extend above late) | Above |
| Cough impulse location | Saphenous opening (4 cm below/lateral to pubic tubercle) | Superficial inguinal ring |
| Invagination test | Inguinal canal empty | Canal occupied |
| Occluding deep inguinal ring | No effect on femoral hernia | Stops indirect inguinal hernia |
Differential Diagnosis
- Saphena varix — disappears on lying down; fluid thrill rather than expansile impulse; Schwartz's test positive
- Enlarged inguinal lymph node (including Cloquet's node within the canal)
- Psoas abscess — cold abscess from Pott's disease, tracks lateral to femoral vessels
- Lipoma, femoral artery aneurysm
Treatment — Surgery is mandatory; treat with urgency
There are three open approaches and laparoscopic options:
| Approach | Incision | Best For |
|---|---|---|
| Low (Lockwood) | Transverse over hernia | Elective; no bowel risk; can be done under LA |
| Inguinal (Lotheissen) | Inguinal canal incision (as for Bassini/Lichtenstein) | Elective; allows combined inguinal repair |
| High (McEvedy/Nyhus) | Transverse above inguinal canal, lateral rectus border | Emergency — strangulation risk; allows bowel resection |
- In all approaches: sac opened, contents inspected/reduced, defect closed (sutures or mesh plug). The lacunar ligament may need incision to aid reduction — beware an abnormal obturator artery branch ("Crown of Death").
- Laparoscopic repair (TAPP/TEP) is appropriate in selected elective cases.
UMBILICAL HERNIA
Classification
Any hernia closely related to the umbilicus falls under this category. Four main types:
1. Exomphalos (Omphalocele)
- Congenital: abdominal contents protrude into the umbilical cord, covered by a transparent diaphanous membrane (not skin)
- A neonatal surgical emergency
2. Congenital (Infantile) Umbilical Hernia
- Occurs through the centre of a congenitally weak umbilical scar
- Common in premature infants and Black infants (incidence up to 8× higher than in white infants); affects up to 10% of infants
- Appears weeks after birth; increases on crying — classic conical shape
- Wide neck → obstruction/strangulation extremely rare (<3 years)
- Content: usually small intestine (resonant on percussion)
- 90–95% resolve spontaneously by age 2–5 years as the umbilical scar thickens
Treatment:
- Conservative (reassurance) if <2 years and asymptomatic
- Surgical repair if persists beyond age 2: curved infra-umbilical incision, sac excised, defect closed with interrupted slowly absorbable sutures
3. Acquired (True) Umbilical Hernia in Adults
- Protrudes through the umbilical scar itself
- Rarer than para-umbilical hernia
- Causes: pregnancy, ascites, bowel distension, ovarian cyst, fibroid (any cause of raised intra-abdominal pressure)
- Always seek the underlying cause of raised IAP
4. Umbilical Hernia in Adults — Clinical Features (includes paraumbilical)
- Seen in overweight men (thinned midline raphe) or postpartum women
- Bulge typically slightly to one side, creating a crescent-shaped umbilicus
- Pain from tissue tension or intermittent bowel obstruction
- Large hernias: overlying skin becomes thin; ulceration possible; spontaneous rupture extremely rare
- Narrow neck relative to sac size → prone to become irreducible, obstructed, strangulated
Treatment:
- High strangulation risk → surgery advised when hernia contains bowel
- Small asymptomatic hernias may be observed but may enlarge
- Mayo repair ("waistcoat over trousers" overlap): transverse incision, sac opened/reduced, fascial edges overlapped with non-absorbable sutures — for defects ≤2 cm
- Mesh repair is recommended for all defects >2 cm and is now preferred even for smaller defects (lower recurrence)
- Open or laparoscopic approaches both acceptable
- Pregnancy: avoid repair before/during pregnancy; postpartum women should exercise and lose weight first
Special note — Liver cirrhosis: Extremely high mortality with Child's B/C disease. Careful patient selection and hepatology involvement required; fine continuous fascial sutures minimise ascites leakage post-op.
PARA-UMBILICAL HERNIA
Definition
The commonest acquired umbilical hernia. Protrudes through a defect adjacent to (most often just above) the umbilicus, in the linea alba between the two rectus muscles. The lower half of the sac fundus is characteristically covered by the umbilicus itself.
Under current guidelines, any hernia in the immediate vicinity of the umbilicus is now termed "umbilical." The distinction "paraumbilical" remains clinically useful, however.
Who Gets It?
- Middle-aged to elderly patients
- Obese women predominantly affected
- Conditions thinning the linea alba: obesity, pregnancy, liver disease with ascites
Clinical Features
- Develops in middle and old age
- Obese women most commonly affected
- Symptoms: pain and swelling — if very small, pain/discomfort may be the only complaint
- Surface smooth, edge distinct (unless patient is very obese)
- Contents:
- Omentum → firm lump
- Bowel → soft, resonant on percussion
- Many are irreducible — contents adhere to sac, or neck becomes narrow; if reducible, the firm fibrous edge of the linea alba defect can be palpated
- Intermittent abdominal pain common due to rigid, non-expanding defect; frank strangulation is less common but possible
Treatment
Same as for adult umbilical hernia:
- Mayo repair for small defects (≤2 cm) — fascial overlap with non-absorbable sutures
- Mesh repair for larger defects and preferred overall given recurrence data
- Laparoscopic repair is an option
Key Comparison Summary
| Feature | Femoral | Umbilical (child) | Umbilical/Para-umbilical (adult) |
|---|---|---|---|
| Site | Femoral canal → saphenous opening | Umbilical scar | Umbilical scar / adjacent linea alba |
| Who | Elderly thin women | Infants; Black race | Obese middle-aged women |
| Spontaneous resolution | No | Yes (90–95% by age 5) | No |
| Strangulation risk | Very high | Very low | Moderate–high (narrow neck) |
| Key ligament | Lacunar (Gimbernat's) | — | — |
| Surgery urgency | Urgent | Elective (if needed) | Elective (urgent if strangulated) |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., pp. 611–612, 1094–1095; S. Das Manual on Clinical Surgery 13th Ed., pp. 611–613, 621–622
This is a shared conversation. Sign in to Orris to start your own chat.