Dobutamine stress echo
Reading File
Finding Sources
Searching PubMed
"dobutamine stress echocardiography"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Dobutamine Stress Echocardiography (DSE)
Concept
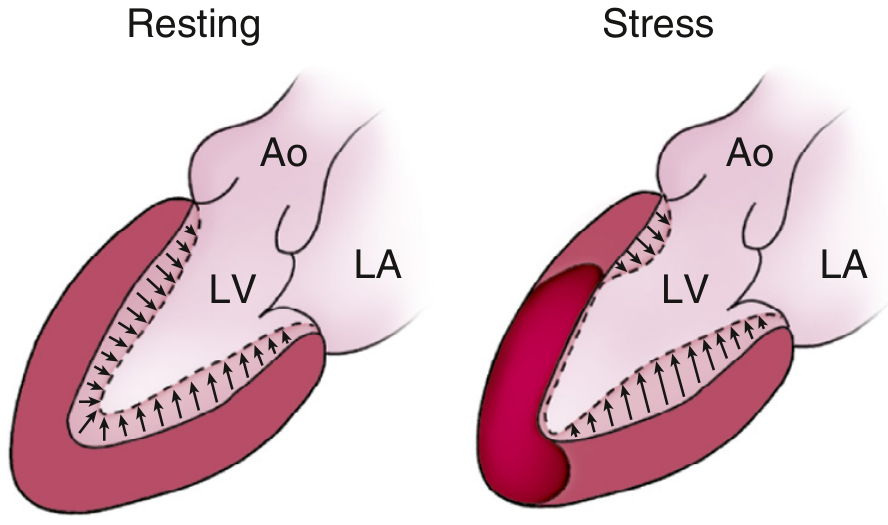
DSE uses dobutamine - a potent beta-1 agonist - to increase heart rate and myocardial contractility, mimicking the hemodynamic effects of exercise. At rest, endocardial motion and wall thickening are normal. After pharmacologic stress, segments supplied by significantly stenosed coronary arteries become ischemic and show reduced wall motion and thickening.
Indications
| Indication | Notes |
|---|---|
| Diagnosis of CAD in patients unable to exercise | Primary use - orthopedic limitations, peripheral vascular disease, severe COPD |
| Evaluation of known CAD | Extent and severity of ischemic territory |
| Myocardial viability assessment | Stunned or hibernating myocardium |
| Pre-operative cardiac risk stratification | Major non-cardiac surgery |
| Valve disease evaluation | Dynamic assessment of mitral regurgitation, aortic stenosis (low-flow, low-gradient AS) |
Protocol
Patient preparation:
- IV line placed; patient positioned in left lateral decubitus on echo stretcher with apical cutout
- Baseline data: heart rate, BP, 12-lead ECG, echocardiographic images
Standard infusion stages (3 minutes each):
| Stage | Dose |
|---|---|
| Low dose 1 | 5 μg/kg/min |
| Low dose 2 | 10 μg/kg/min |
| Mid dose | 20 μg/kg/min |
| High dose | 30 μg/kg/min |
| Peak | 40 μg/kg/min |
- If target heart rate (85% of maximum predicted = 220 - age) is not achieved at 40 μg/kg/min, atropine is added IV in divided doses of 0.25-0.5 mg (maximum 2 mg total). Atropine added at the 30 μg/kg/min stage reaches target heart rate faster with fewer side effects.
- Low-dose protocol (2.5 → 5 → 7.5 → 10 → 20 μg/kg/min) is preferred for patients with moderately-severely depressed LV function, multivessel disease, or high arrhythmia risk, and for viability assessment.
Images acquired at: rest, low-dose, prepeak, peak, and recovery
Views: Parasternal short-axis (base + mid-cavity), apical 4-chamber, 2-chamber, long-axis. Same depth settings must be used at all stages for comparison.
Endpoints for Stopping the Test
- Reaching maximum protocol dose (40 μg/kg/min)
- Patient's discomfort / intolerable symptoms
- New wall motion abnormality in two or more adjacent segments
- ST-segment elevation on ECG
- Reaching 85% of maximum predicted heart rate for age
- Systolic BP >200 or <100 mmHg, or diastolic BP >120 mmHg
- Significant ventricular arrhythmias
Monitoring
- Periodic BP (every 2-3 minutes)
- Continuous ECG monitoring
- Clinical observation for symptoms
- Crash cart, defibrillator, emergency cardiac medications, and IV esmolol (reverses dobutamine effects) must be immediately available
Interpretation: Ischemia Detection
| Wall Motion Finding | Interpretation |
|---|---|
| Normal at rest → hyperkinesis at peak | Normal (no ischemia) |
| Normal at rest → hypo/akinesis at peak | Inducible ischemia |
| Akinesis at rest → no change at any dose | Scar (non-viable) |
| Biphasic response | Viable myocardium with significant CAD |
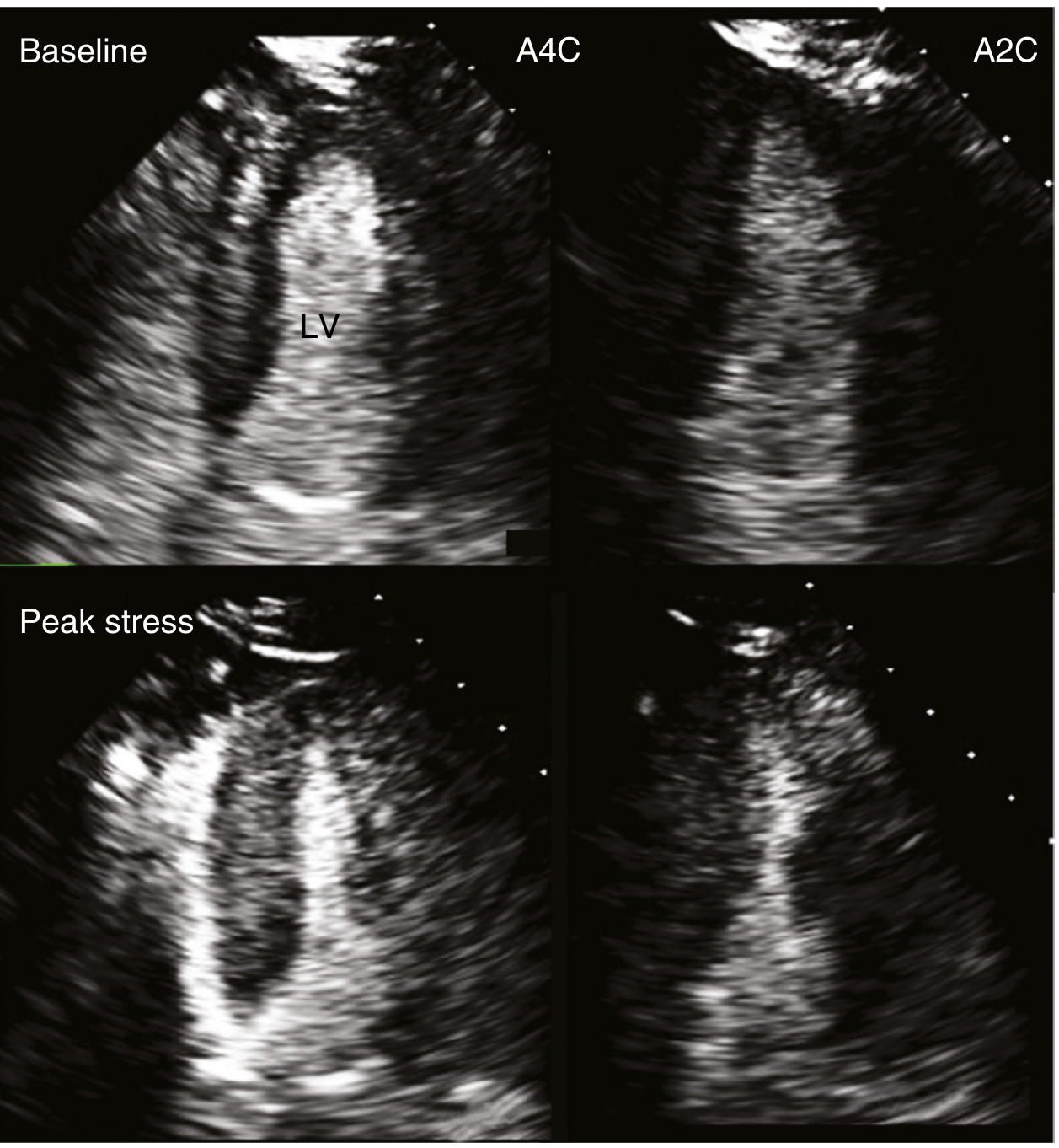
Positive test: New or worsening regional wall motion abnormality (hypokinesis or akinesis) in a previously normal or hypokinetic segment at peak stress, returning to baseline at recovery.
- Report should include: Peak heart rate as % of maximum predicted, symptoms, BP response. Note: BP and ECG changes are not diagnostic for CAD in DSE (unlike exercise treadmill testing).
Myocardial Viability Assessment (Low-Dose DSE)
DSE is a key tool for identifying hibernating myocardium (chronic hypo/akinesis at rest due to chronic ischemia that may recover after revascularization) and stunned myocardium (post-infarction dysfunction that may recover with time).
Biphasic response - the hallmark of viability:
- Low dose (5-10 μg/kg/min): improved wall thickening in the akinetic/hypokinetic segment
- High dose (40 μg/kg/min): worsening of that same segment (inducible ischemia)
This pattern indicates viable myocardium supplied by a significantly stenosed vessel - revascularization is likely to restore function. If there is no improvement at low dose and no side effects, the dose can be escalated. If there is worsening in hypokinetic segments during the low-dose protocol, the test should be terminated.
Complications and Safety
From a meta-analysis of 55,071 patients (Geleijnse et al., 2010 - Circulation 121:1756):
| Complication | Risk |
|---|---|
| Any major complication | 1 in 475 patients |
| Death | <0.01% |
| Myocardial infarction | 0.02% |
| Ventricular fibrillation | ~0.04% |
| Cardiac rupture, asystole, CVA | <0.01% each |
Common minor effects (~10%): premature atrial/ventricular beats, anxiety, palpitations, tremor, paresthesias, chest pain. Up to 4% have nonsustained supraventricular tachycardia. Short-acting IV beta-blockers (esmolol, metoprolol) effectively reverse dobutamine effects.
Limitations
- Endocardial definition - poor image quality in some patients (particularly anterior wall, due to adjacent lung); IV contrast agents should be used when endocardial definition is suboptimal
- Cardiac and respiratory motion - artifacts during high-dose infusion
- Inadequate stress - failure to reach target heart rate (more common in patients on beta-blockers); atropine mitigates this
- Abnormal resting LV function - harder to assess new wall motion abnormalities on a background of existing dysfunction
Comparison with Other Stress Modalities
| Feature | DSE | Exercise Echo | Vasodilator Stress |
|---|---|---|---|
| Mechanism | Increased HR + contractility | Increased HR + work | Coronary steal |
| Used when | Cannot exercise | Can exercise | Cannot exercise (also for nuclear) |
| BP/ECG diagnostic for CAD | No | Yes | No |
| Viability assessment | Yes (biphasic) | No | No |
| Image quality | Potentially difficult at peak | Best immediately post-exercise | Usually adequate |
Advanced techniques including speckle tracking strain imaging and 3D echocardiography are increasingly used with DSE to improve sensitivity and reduce reader subjectivity, though optimal protocols are still being defined. At rest, global longitudinal strain can detect subclinical LV dysfunction; during stress, strain rate is better than strain for ischemia detection.
- Textbook of Clinical Echocardiography, pp. 245-248, 263
- Pfenninger and Fowler's Procedures for Primary Care, p. 675
Esmolol dose
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I have enough data for a comprehensive answer.
Esmolol - Dosing Reference
Class: Ultra-short-acting, beta-1 selective (cardioselective) IV beta-blocker
Half-life: ~9 minutes (eliminated by erythrocyte esterases - not hepatic, not renal)
Onset: Within 60 seconds
Duration of effect: 10-20 minutes
Standard Dosing Protocol (SVT / Rate Control)
The dosing follows a stepwise bolus + maintenance pattern:
| Step | Bolus | Maintenance Infusion | Duration |
|---|---|---|---|
| 1st attempt | 0.5 mg/kg IV over 1 min | 50 mcg/kg/min | 4 min |
| 2nd attempt (if inadequate) | 0.5 mg/kg IV over 1 min | 100 mcg/kg/min | 4 min |
| 3rd attempt (if inadequate) | 0.5 mg/kg IV over 1 min | 150 mcg/kg/min | 4 min |
| Maximum | - | 300 mcg/kg/min | 4 min |
After each 4-minute maintenance period: if response is adequate, continue at the effective maintenance rate. If not, repeat the bolus and increase the infusion by 50 mcg/kg/min steps up to 300 mcg/kg/min maximum.
By Clinical Indication
| Indication | Dose |
|---|---|
| SVT / AF/flutter rate control | Load 0.5 mg/kg over 1 min → maintenance 50-300 mcg/kg/min (stepwise) |
| Hypertensive emergency | Load 250-500 mcg/kg IV over 1 min → maintenance infusion (titrate) |
| Aortic dissection | Same as hypertensive emergency; used as adjunct with vasodilator |
| Intraoperative tachycardia/hypertension | 0.5-1 mg/kg bolus; can repeat; infusion 50-300 mcg/kg/min |
| Reversal of dobutamine in stress echo | 0.5-1 mg/kg IV bolus (short bolus sufficient given brief need) |
| Thyrotoxic crisis | 50-100 mcg/kg/min infusion |
| Pediatric | Maintenance 100-200 mcg/kg/min; increase bolus in 100 mcg/kg steps |
Indications
- Rapid conversion of SVT
- Ventricular rate control in AF or atrial flutter (non-preexcited)
- Non-compensated sinus tachycardia requiring slowing
- Adjunctive therapy for torsades de pointes (VT)
- Hypertensive emergencies, aortic dissection
- Perioperative hypertension/tachycardia
Contraindications
- 2nd or 3rd degree heart block
- Decompensated/frank heart failure
- Bradycardia
- Use with IV verapamil (additive AV block)
- Active bronchospasm (use with caution; beta-1 selectivity is lost at high doses)
- Diabetes (caution - masks hypoglycemia symptoms)
Practical Notes
-
At therapeutic doses - beta-1 selective (cardiac). At higher doses - loses selectivity, also blocks beta-2 (lung, vessels)
-
No hepatic/renal dose adjustment needed (erythrocyte metabolism)
-
If extravasation occurs - can cause skin necrosis and blistering
-
In stress echo context: a small bolus (0.5-1 mg/kg) rapidly terminates persistent tachycardia, palpitations, or other dobutamine side effects within 1-2 minutes
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 301
-
Tintinalli's Emergency Medicine, Table 57-5
This is a shared conversation. Sign in to Orris to start your own chat.