Rat poisoning case
Reading File
Finding Sources
Finding Sources
Searching PubMed
rodenticide poisoning management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information to deliver a thorough answer. Let me compile this into a well-structured response.
Rat Poisoning (Rodenticide Toxicology)
Rodenticides are broadly classified as anticoagulants and non-anticoagulants. Each has a distinct mechanism, clinical presentation, and management approach.
1. Anticoagulant Rodenticides
First Generation - Warfarin
- Mechanism: Inhibits Vitamin K epoxide reductase - blocks synthesis of factors II, VII, IX, X (and proteins C and S)
- Clinical: Significant coagulopathy requires large single doses or repeated exposures. Onset of anticoagulant effect: 12-48 hours. Half-life: ~42 hours
- Treatment:
- Single small ingestion in children: no treatment necessary
- Potentially toxic ingestion: activated charcoal
- Monitor INR at baseline, 12-24 hours
- Vitamin K1 (phytonadione) if INR >2.0: children 1-5 mg/day PO; adults 20 mg/day PO in 2-4 divided doses
Second Generation - Superwarfarins (Brodifacoum, Difenacoum, Bromadiolone)
These are the most clinically significant group, responsible for ~80% of human rodenticide exposures in the US.
- Mechanism: Same as warfarin, but far more potent and prolonged
- Half-life of brodifacoum: ~120 days - a single ingestion can cause anticoagulation for weeks to months
- Clinical: Coagulopathy within 24-48 hours of intentional ingestion; unexplained bleeding/coagulopathy should raise suspicion (patient may not disclose ingestion)
- Key point: NOT detected by warfarin assays - specific reference lab serum assays are required
- Treatment:
- Acute intentional ingestion: gastric lavage (if early) + activated charcoal
- Baseline INR, repeat at 12 and 24 hours
- If INR elevated but no active hemorrhage: oral Vitamin K1 at high doses (50-100 mg/day or more in adults), continued for weeks to months due to long half-life
- Active hemorrhage: FFP or PCC + IV Vitamin K1
- Pediatric accidental ingestions are unlikely to cause significant toxicity; monitor INR at 24 and 48 hours
Also include indandiones (diphacinone, chlorophacinone): similar mechanism and clinical profile to superwarfarins.
2. Non-Anticoagulant Rodenticides
Aluminum Phosphide (ALP) / Zinc Phosphide
One of the most lethal rodenticides encountered clinically, particularly in South Asia.
- Mechanism: Releases phosphine gas (PH3) on contact with moisture/gastric acid - a mitochondrial toxin inhibiting cytochrome c oxidase
- Odor: Garlic-like smell from mouth, gastric contents (forensically significant)
- Fatal dose ALP: 1-3 g (1-3 tablets); fatal period typically 6-12 hours; mortality 35-100%
- Zinc phosphide: Similar but slower onset due to gradual phosphine release
- Clinical features by severity:
| Severity | Features |
|---|---|
| Mild (inhalation) | Mucous membrane irritation, respiratory distress, nausea, headache |
| Moderate | Ataxia, paresthesia, tremors, diplopia, jaundice, weakness |
| Severe | ARDS, cardiac arrhythmias, CHF, pulmonary edema, convulsions, coma |
| Ingestion | GIT: N/V/D; CVS: hypotension, shock, arrhythmias, myocarditis, pericarditis; Respiratory: cough, dyspnea, pulmonary edema; Hepatic: jaundice; Renal: ARF; CNS: altered sensorium, coma |
- Most common cause of death: Cardiogenic shock
- Treatment (no specific antidote):
- Gastric lavage with potassium permanganate (after endotracheal intubation) - oxidizes phosphine to non-toxic phosphate; repeat 2-3 times
- Activated charcoal 100g with sorbitol (not water)
- Antacids - reduce gastric phosphine absorption
- Liquid paraffin - aids gut excretion
- Magnesium sulphate IV - reduces organ toxicity, corrects hypomagnesemia and arrhythmias (1g IV, repeated q2h, then 1-1.5g q6h for 5-7 days)
- Aggressive IV fluids: 4-6L in first 3-6 hours (50% normal saline)
- Low-dose dopamine 4-6 mcg/kg/min
- IV hydrocortisone 400 mg q4-6h
- Oxygen for hypoxia; sodium bicarbonate for metabolic acidosis
- Peritoneal dialysis/hemodialysis if renal failure
- Postmortem: Garlic odor, blood-stained froth, congested GI mucosa, centrizonal hemorrhagic necrosis of liver
Strychnine
Found in old rodenticide products and some Ayurvedic formulations.
- Mechanism: Competitive antagonist of glycine at postsynaptic spinal cord and brainstem motor neurons
- Fatal dose: 50-100 mg (oral); 1-3g of Strychnos seeds
- Clinical:
- Painful muscle spasms, opisthotonos, trismus ("risus sardonicus"/sardonic smile)
- Mydriasis, proptosis
- Patient remains conscious between convulsive episodes (key distinguishing feature)
- Death from respiratory failure
- Differential diagnosis: Must be distinguished from tetanus, rabies, meningitis, cocaine toxicity
- Key difference from tetanus: History of poisoning vs. wound; no trismus prodrome; no autonomic instability
| Feature | Strychnine | Tetanus |
|---|---|---|
| History | Poisoning | Wound/injury |
| Onset | Rapid (minutes) | Gradual (days) |
| Consciousness | Preserved between spasms | Variable |
| Trismus | Present | Present |
| Autonomic effects | Absent | Common (late) |
- Treatment:
- Airway control first
- Minimize sensory stimulation (quiet, dark room)
- Activated charcoal (within ~1 hour of ingestion)
- Avoid gastric lavage - may precipitate convulsions
- Diazepam IV 10-15 mg (adults), 0.1-0.3 mg/kg (children) for seizures
- Midazolam 5-10 mg; phenobarbitone 10 mg/kg if benzodiazepines insufficient
- Intubation + mechanical ventilation if needed
- Neuromuscular blockade (succinylcholine then non-depolarizing agents) if hyperthermia persists
- IV sodium bicarbonate for acidosis; dantrolene for refractory hyperthermia
Barium Carbonate
- Mechanism: Blocks potassium channels - causes severe hypokalemia
- Clinical: Onset within ~8 hours; severe vomiting, diarrhea, abdominal pain, muscle weakness, paralysis, cardiac dysrhythmias, respiratory failure
- Treatment: Activated charcoal + sodium/magnesium sulfate added to lavage (converts barium carbonate to less soluble barium sulfate); aggressive potassium replacement
Sodium Fluoroacetate (Compound 1080)
- Mechanism: Blocks the Krebs cycle (fluoroacetate → fluorocitrate → inhibits aconitase)
- Clinical: Nausea, vomiting, respiratory distress, lactic acidosis, seizures, coma, cardiac dysrhythmias, ventricular tachycardia/fibrillation, hypocalcemia, hyperkalemia
- Treatment: Activated charcoal; seizure and dysrhythmia control; glycerol monoacetate, calcium gluconate, sodium succinate, ethanol loading (experimental); toxicologist consultation required
Thallium
- Route of use: Formerly a common rodenticide (now largely banned)
- Mechanism: Mimics potassium, inhibits cellular enzymes
- Classic triad: Alopecia (2-3 weeks post-exposure), painful peripheral neuropathy, gastrointestinal illness
- Treatment: Prussian blue (ferric ferrocyanide) to bind thallium in the gut
Arsenic
- Clinical: Cholera-like diarrhea followed weeks-months later by peripheral neuropathy, Mees' lines (nail changes), skin changes (hyperpigmentation, keratosis)
- Treatment: Chelation with succimer (DMSA) or dimercaprol (BAL)
Yellow/White Phosphorus
- Clinical: Skin/oral burns, luminescent vomitus ("smoking stool syndrome"), garlic odor, direct cardiotoxicity, nephrotoxicity, late multiorgan failure with hepatorenal dysfunction
- Treatment: Supportive; cardiac monitoring; electrolyte correction; maintain serum glucose
Tetramine (TETS / Tetramethylenedisulfotetramine)
- Mechanism: Blocks GABA-A receptors in the CNS
- Clinical: Rapid onset - headache, nausea, dizziness, then loss of consciousness, refractory seizures, death (respiratory failure)
- Highly toxic: ~6-7 mg sufficient to kill an adult
- No antidote; treat with benzodiazepines/barbiturates for seizures
Summary Table
| Agent | Mechanism | Key Feature | Antidote/Treatment |
|---|---|---|---|
| Warfarin | Vit K antagonist | Coagulopathy | Vitamin K1 |
| Superwarfarins (brodifacoum) | Vit K antagonist | Half-life 120 days | High-dose Vit K1 (weeks-months) |
| Aluminum phosphide | Phosphine - mitochondrial toxin | Garlic odor; cardiogenic shock | Supportive; MgSO4; no antidote |
| Zinc phosphide | Phosphine - mitochondrial toxin | Slower onset than ALP | Supportive |
| Strychnine | Glycine antagonist | Conscious between spasms | Benzos; dark quiet room |
| Barium carbonate | K+ channel block | Hypokalemia; paralysis | K+ replacement; sulfate lavage |
| Na fluoroacetate | Krebs cycle block | Lactic acidosis; VF | Supportive; glycerol monoacetate |
| Thallium | K+ mimic; enzyme inhibitor | Alopecia (delayed) | Prussian blue |
| Arsenic | Sulfhydryl binding | Peripheral neuropathy (delayed) | Succimer/BAL |
| Tetramine | GABA-A block | Rapid refractory seizures | Benzos; no antidote |
Sources:
- The Essentials of Forensic Medicine and Toxicology, 36th Ed. (2026)
- Tintinalli's Emergency Medicine
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
- Brenner and Rector's The Kidney
Recent literature: A 2025 meta-analysis (PMID 40702417) highlights metallophosphide (ALP/ZnP) poisoning as a rising public health problem particularly in Ethiopia and South Asia. A 2025 forensic case series (PMID 40974629) reviewed 88 anticoagulant rodenticide cases with implications for forensic diagnosis.
Xylocard
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have sufficient information for a comprehensive answer. Here is the full clinical profile of Xylocard:
Xylocard (Lignocaine / Lidocaine)
Xylocard is the brand name for lignocaine (lidocaine) 2% injection, available as a 5 mL ampoule (100 mg/5 mL). It is manufactured by AstraZeneca and is one of the most widely used antiarrhythmic agents in emergency and critical care settings in India.
Drug Profile
| Property | Detail |
|---|---|
| Generic name | Lignocaine / Lidocaine |
| Brand | Xylocard (AstraZeneca) |
| Class | Vaughan-Williams Class IB antiarrhythmic |
| Also classified | Local anesthetic (amide type) |
| Route | IV (antiarrhythmic); also IM, topical, epidural, spinal |
| Strength | 2% (20 mg/mL), 5 mL ampoule = 100 mg |
Mechanism of Action
Lidocaine acts by blocking fast voltage-gated sodium (Na+) channels in cardiac membranes. As a Class IB agent:
- Binds preferentially to inactivated Na+ channels - greater effect on rapidly firing (ischemic/arrhythmic) tissue
- Shortens the action potential duration and effective refractory period in the His-Purkinje system and ventricular myocardium
- Suppresses automaticity - reduces spontaneous phase 4 depolarization in ectopic foci
- No significant effect on normal conduction - does not significantly slow AV conduction or sinus rate at therapeutic doses
- Little effect on atrial tissue - hence useless for atrial arrhythmias
- Minimal effect on the surface ECG at therapeutic doses - no significant change in PR interval, QRS width, or QT interval (unlike Class IA agents)
Indications (Cardiac - Antiarrhythmic Use)
- Ventricular tachycardia (VT) - hemodynamically stable VT
- Ventricular fibrillation (VF) - refractory VF/pulseless VT (second-line after amiodarone, or when amiodarone unavailable)
- Ventricular ectopics - suppression of ventricular premature beats in specific contexts (e.g., after MI with frequent PVCs causing hemodynamic compromise)
- Post-ROSC VF/pulseless VT - maintenance infusion may be considered after return of spontaneous circulation
- Digitalis-induced arrhythmias - lidocaine or phenytoin preferred when AV block is present
Note: The 2015 AHA/ACLS guidelines removed lidocaine from the routine cardiac arrest algorithm. A 2016 multicenter RCT (ALPS trial) showed no improvement in survival or neurologic outcome with lidocaine (or amiodarone) vs. placebo for out-of-hospital cardiac arrest (OHCA) from VF/pulseless VT. Lidocaine remains an option when amiodarone is unavailable.
Dosing
Acute Arrhythmia (IV bolus)
- Loading dose: 1-1.5 mg/kg IV bolus (typically 75-100 mg in an adult)
- Repeat bolus: 0.5-0.75 mg/kg IV if arrhythmia persists, after 5-10 minutes
- Maximum total bolus dose: 3 mg/kg
Maintenance Infusion (post-conversion)
- Usual rate: 1-4 mg/min IV infusion
- If arrhythmia recurs during infusion: give additional 0.5 mg/kg bolus and increase infusion rate up to 4 mg/min
Dose Adjustments (CRITICAL)
- Liver disease (hepatically metabolized): same bolus, reduce infusion rate by 50%
- Age >70 years: same bolus, reduce infusion rate by 50%
- Heart failure/low cardiac output: reduce both bolus and infusion (reduced hepatic blood flow slows clearance)
Pharmacokinetics
| Parameter | Value |
|---|---|
| Onset (IV) | 45-90 seconds |
| Duration (single bolus) | 10-20 minutes |
| Distribution | Rapid, wide - highly lipid soluble |
| Protein binding | ~70% (to alpha-1 acid glycoprotein) |
| Metabolism | Hepatic (first-pass extensive - hence not oral) |
| Active metabolites | MEGX (monoethylglycinexylidide), GX - may contribute to toxicity |
| Elimination | Renal (<10% unchanged) |
| Half-life (IV) | ~1.5-2 hours (prolonged in liver disease/CHF) |
Toxicity
Toxicity occurs with bolus doses exceeding 3 mg/kg or with accumulation in liver disease.
CNS Toxicity (dose-dependent, early warning signs precede cardiac toxicity)
- Perioral/tongue numbness and tingling (paresthesia) - earliest sign
- Dizziness, drowsiness, tinnitus, reduced hearing
- Disorientation, confusion
- Muscle tremors
- Seizures (at high doses)
Cardiovascular Toxicity (higher doses)
- Myocardial depression
- Hypotension
- Widening QRS complex
- Bradycardia, AV block
- Circulatory collapse
Key point: CNS toxicity (perioral paresthesia, tremors) is the early warning - always precedes cardiac toxicity at typical doses. If a patient on a lidocaine infusion develops these symptoms, stop or reduce the infusion immediately.
Contraindications
- High-degree AV block (2nd or 3rd degree) without a pacemaker
- Sinoatrial block
- Stokes-Adams syndrome
- Severe sinus bradycardia
- Known hypersensitivity to amide-type local anesthetics
- Wolff-Parkinson-White (WPW) syndrome with SVT - may accelerate conduction through accessory pathway
- Atrial arrhythmias - ineffective (no significant effect on atrial tissue)
Important Drug Interactions
- Beta-blockers / cimetidine: Reduce hepatic clearance of lidocaine - increase toxicity risk
- Phenytoin (IV): Additive cardiac depression
- Procainamide: Additive CNS/cardiac toxicity
- Succinylcholine: Lidocaine prolongs its effect
Comparison: Lidocaine vs. Amiodarone in VT/VF
| Feature | Lidocaine (Xylocard) | Amiodarone |
|---|---|---|
| Class | IB | III (mixed) |
| Onset | Seconds | Minutes |
| VF/VT efficacy | Moderate | Superior |
| Survival benefit (OHCA) | Not demonstrated (ALPS 2016) | Not demonstrated (ALPS 2016) |
| Current guideline status | Second-line / if amiodarone unavailable | First-line |
| CNS toxicity | Common at high doses | Less common (short-term) |
| Hypotension | Less | More (infusion) |
Other Uses of Lignocaine
Beyond the antiarrhythmic use of Xylocard, lignocaine is also used as:
- Local anesthetic for infiltration, nerve blocks, epidural, spinal anesthesia
- Topical anesthetic (viscous lignocaine for oropharyngeal procedures)
- IV lignocaine infusion for perioperative analgesia (reduces opioid requirements - systemic anti-inflammatory and analgesic effects)
- Intubation - IV bolus before laryngoscopy to blunt the hemodynamic response and reduce ICP surge
Sources:
- Tintinalli's Emergency Medicine (Lidocaine/Lignocaine section, p. 200)
- Harrison's Principles of Internal Medicine 22E (2025)
- Goldman-Cecil Medicine
- Fischer's Mastery of Surgery
Vt treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
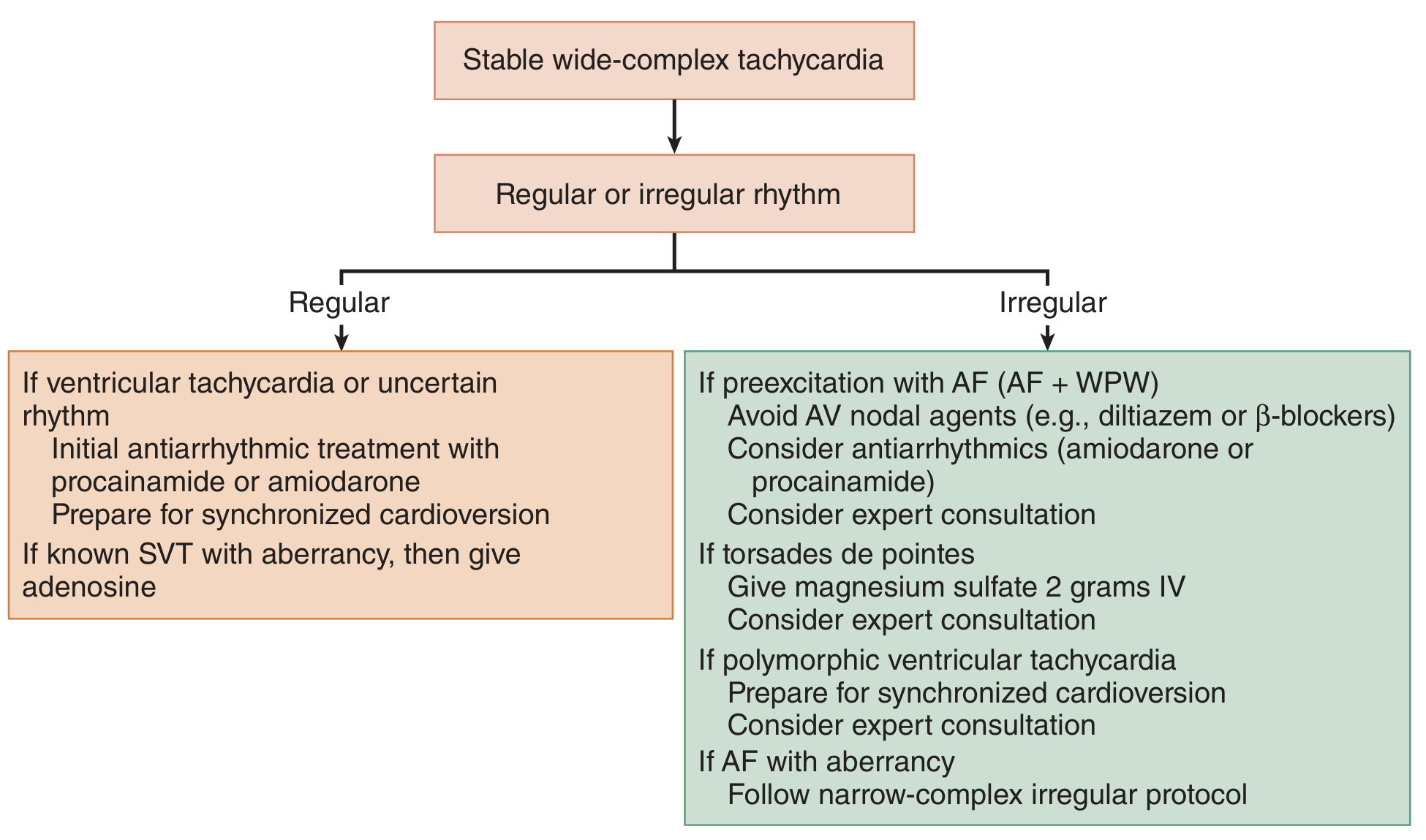
Here is a comprehensive, structured guide to VT treatment:
Ventricular Tachycardia (VT) - Treatment
Step 1: Immediate Risk Stratification
The first and most critical question is always: Does the patient have a pulse?
VT
├── Pulseless VT → Treat as VF (defibrillation + ACLS)
└── VT with pulse
├── Hemodynamically UNSTABLE → Immediate synchronized cardioversion
└── Hemodynamically STABLE → Pharmacologic treatment
Signs of hemodynamic instability:
- Hypotension (SBP <90 mmHg)
- Altered mental status / loss of consciousness
- Acute chest pain / ischemia
- Signs of pulmonary edema / acute heart failure
- Shock
Step 2: VT Classification Matters
| Type | Definition | Key Feature |
|---|---|---|
| Monomorphic VT | Uniform QRS morphology | Regular, constant-looking complexes |
| Polymorphic VT | Varying QRS morphology | Changes shape beat to beat |
| Torsades de Pointes (TdP) | Polymorphic VT + QTc >450 ms | "Twisting of the points" pattern; associated with QT prolongation |
| Sustained VT | Lasts >30 sec or requires termination | High risk of deterioration |
| Non-sustained VT | Self-terminating <30 sec | Often incidental; may not need acute Rx |
A. Pulseless VT - Treat as VF
Follow standard ACLS cardiac arrest algorithm:
- CPR - High-quality, uninterrupted chest compressions
- Defibrillation - Immediate unsynchronized shock
- Biphasic: 120-200 J (manufacturer-recommended)
- Monophasic: 360 J
- Epinephrine 1 mg IV/IO every 3-5 minutes
- Antiarrhythmics (after 2nd failed shock):
- Amiodarone (first-line): 300 mg IV bolus; repeat 150 mg if no response
- Lidocaine (alternative if amiodarone unavailable): 1-1.5 mg/kg IV bolus
- Continue 2-minute CPR cycles with rhythm checks
- Treat reversible causes (5 Hs and 5 Ts)
Note: A 2016 multicenter RCT (ALPS trial) showed neither amiodarone nor lidocaine improved survival to discharge or neurological outcomes vs. placebo for OHCA from VF/pulseless VT. However, both are still guideline options.
B. Hemodynamically UNSTABLE VT (with pulse)
Immediate synchronized DC cardioversion - do not delay for pharmacologic attempts.
- Sedate if possible (midazolam, etomidate, or ketamine)
- Energy: 100-200 J biphasic (synchronized mode); if fails, escalate
- After cardioversion: start IV antiarrhythmic infusion to prevent recurrence
- Critical: Always use SYNCHRONIZED mode to avoid R-on-T and VF induction
- Exception: If the QRS is very wide/bizarre and sync fails to lock - use unsynchronized
C. Hemodynamically STABLE Monomorphic VT
Pharmacologic treatment is first-line.
Drug Options (in order of preference):
1. Procainamide (Drug of Choice for stable monomorphic VT)
- Dose: 20-50 mg/min IV (or 100 mg every 5 min) until:
- Arrhythmia terminates, OR
- QRS widens by >50%, OR
- Hypotension occurs, OR
- Maximum dose reached (17 mg/kg)
- Maintenance: 1-4 mg/min infusion
- Also useful when rhythm is uncertain (works for VT AND AF/SVT)
- Evidence: Recent study showed superiority of procainamide over amiodarone for conversion of stable VT
- Caution: Avoid in acute MI and LV dysfunction
2. Amiodarone (Preferred if LV dysfunction / AMI)
- Dose: 150 mg in 100 mL D5W IV over 10 minutes
- Followed by: 1 mg/min infusion for 6 hours, then 0.5 mg/min for 18 hours
- Breakthrough: Additional 150 mg boluses over 10 min
- Maximum daily dose: 2.2 g
- Preferred over procainamide in setting of acute MI or reduced EF
- Also covers SVT with aberrancy if uncertain rhythm
3. Lidocaine (Xylocard) - Third-line
- Loading: 50-100 mg IV over 2-3 min; may repeat in 5 min
- Maintenance: 1-4 mg/min infusion
- Reduce infusion by 50% in liver disease or age >70
- Less effective than procainamide or amiodarone for stable VT
4. Electrical cardioversion - if drugs fail or patient deteriorates
D. Torsades de Pointes (Polymorphic VT + Long QT)
This is treated differently from regular VT - standard antiarrhythmics can worsen it.
| Step | Action |
|---|---|
| 1 | Stop all QT-prolonging drugs (cause removal) |
| 2 | IV Magnesium sulfate 2 g IV over 2 min - first-line, even if Mg is normal |
| Then infuse | 1-2 g/h magnesium maintenance |
| 3 | Correct electrolytes - K+ >4.5 mEq/L, Mg2+ >2 mEq/L |
| 4 | Overdrive pacing (temporary transcutaneous or transvenous) at 90-120 bpm to shorten QT |
| 5 | Isoproterenol infusion - increases heart rate, shortens QT (useful in acquired long QT) |
| 6 | If hemodynamically unstable: immediate defibrillation |
| Avoid | Class IA (procainamide), Class III agents (amiodarone) - they further prolong QT |
E. Polymorphic VT with Normal QT Interval
Usually ischemia-driven.
- Treat the underlying ischemia (urgent revascularization)
- IV beta-blockers
- IV amiodarone
- Prepare for synchronized cardioversion if unstable
Summary Drug Dosing Table
| Drug | IV Dose | Indication | Notes |
|---|---|---|---|
| Procainamide | 20-50 mg/min to max 17 mg/kg; then 1-4 mg/min infusion | Stable monomorphic VT (1st line) | Stop if QRS widens >50% or hypotension |
| Amiodarone | 150 mg over 10 min; then 1 mg/min x6h, 0.5 mg/min x18h | Stable VT with AMI/low EF (1st line); pulseless VT (300 mg bolus) | Max 2.2 g/day |
| Lidocaine | 50-100 mg over 2-3 min; then 1-4 mg/min | Stable VT (3rd line); pulseless VT (alternative) | Reduce dose in liver disease/elderly |
| Magnesium sulfate | 2 g IV over 2 min; then 1-2 g/h | Torsades de Pointes, QT prolongation | Also for hypomagnesemia-related VT |
| DC Cardioversion | 100-200 J (biphasic, synchronized) | Unstable VT with pulse | Sedate first; use sync mode |
| Defibrillation | 120-200 J biphasic (unsynchronized) | Pulseless VT | Part of ACLS arrest algorithm |
F. Long-Term / Definitive Management
After acute stabilization, address the root cause and prevent recurrence:
- ICD (Implantable Cardioverter-Defibrillator) - mainstay for secondary prevention and in patients with reduced EF (EF <35%) and sustained VT. Guideline class I indication for most patients with structural heart disease and sustained VT/VF
- Catheter ablation - curative for idiopathic VTs (e.g., RVOT tachycardia, fascicular VT); palliative for scar-related VT causing frequent ICD shocks. Preferred over long-term antiarrhythmics for idiopathic VT
- Oral antiarrhythmics - amiodarone, sotalol, mexiletine (as ICD adjuncts to reduce VT burden)
- Beta-blockers - reduce VT recurrence, especially post-MI; also reduce appropriate ICD shocks
- Treat underlying cause - revascularize ischemia, optimize heart failure, correct electrolytes, stop offending drugs
Key Clinical Pearls
- "When in doubt, treat as VT" - wide-complex regular tachycardia with history of heart disease is VT until proven otherwise
- Adenosine will NOT terminate VT - it helps diagnose/treat SVT with aberrancy; useful diagnostically
- Calcium channel blockers and beta-blockers are DANGEROUS in VT - may cause hemodynamic collapse
- Procainamide is safer than adenosine when rhythm is uncertain (wide-complex, unsure VT vs SVT) - it works for both
- Torsades requires magnesium, not amiodarone - amiodarone further prolongs QT
- Electrical storm (≥3 VT/VF episodes in 24h): IV beta-blockers (esmolol) + amiodarone + consider urgent ablation
Sources:
- Tintinalli's Emergency Medicine (Chapters 18, 23)
- Sabiston Textbook of Surgery
- Goldman-Cecil Medicine
- The Washington Manual of Medical Therapeutics
- Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.