TB according to harrison
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content on TB from Harrison's 22E. Let me compile this into a thorough, well-organized response.
Tuberculosis (TB) — Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Chapter 183 by Mario C. B. Raviglione & Andrea Gori
Overview
TB, caused by bacteria of the Mycobacterium tuberculosis complex, is one of the oldest diseases known to humans. In 2023, it returned to being the top cause of infectious death from a single agent (after COVID-19 displaced it during 2020-2022). Population genomic studies suggest M. tuberculosis emerged ~70,000 years ago in Africa. If untreated, the disease is fatal in >70% of cases; if properly treated, drug-susceptible TB is curable in the vast majority.
Etiologic Agent
The M. tuberculosis complex has eight subgroups:
- M. tuberculosis (sensu stricto) - by far the most important human pathogen
- M. africanum - closely related, cases in West, Central, and East Africa
- M. bovis - bovine tubercle bacillus; resistant to pyrazinamide; ~140,000 human cases/year (2020), mainly in Africa; transmitted via unpasteurized milk
- M. caprae - related to M. bovis
- Other rare agents: M. pinnipedii, M. mungi, M. microti (the "vole" bacillus - less virulent), M. canetti
There is no known environmental reservoir for any of these organisms.
Microbiological characteristics:
- Rod-shaped, non-spore-forming, thin aerobic bacterium: 0.5 x 3 μm
- Neutral on Gram staining; classified as acid-fast bacilli (AFB) - once stained, cannot be decolorized by acid alcohol
- Acid fastness due to high content of mycolic acids, long-chain cross-linked fatty acids, and other cell-wall lipids
- Other acid-fast organisms: Nocardia, Rhodococcus, Legionella micdadei, Isospora, Cryptosporidium
- Cell wall structure: lipids (mycolic acids) linked to arabinog alactan and peptidoglycan - results in very low permeability, reducing effectiveness of most antibiotics
- Genome: 4.4 million base pairs, 4043 genes, high G+C content (65.6%)
Epidemiology
- 10.8 million estimated new TB cases worldwide in 2023 (rate: 134/100,000)
- 8 countries account for two-thirds of all cases: India (26%), Indonesia (10%), China (6.8%), Philippines (6.8%), Pakistan (6.3%), Nigeria (4.6%), Bangladesh (3.5%), DRC (3.1%)
- 55% males, 33% females, 12% children
- 1.25 million deaths from TB in 2023, including 160,000 among HIV co-infected persons; 98% in low- and middle-income countries
- ~97% of cases from low- and middle-income countries
High-risk groups:
- HIV-infected individuals (highest risk)
- Close contacts of active TB cases
- Immigrants from high-prevalence countries
- Healthcare workers
- Incarcerated persons
- Persons with silicosis, DM, malnutrition, renal failure, TNF-α inhibitor therapy
Pathogenesis and Immunity
Transmission
Spread occurs via airborne droplet nuclei produced when patients with pulmonary TB cough, sneeze, talk, or sing. Droplet nuclei (1-5 μm) can remain suspended in the air for hours. A single patient can infect many contacts.
Natural History After Infection
- Droplet nuclei reach alveoli and are ingested by alveolar macrophages
- If not eliminated, bacilli multiply within macrophages
- Bacilli spread via lymphatics to regional lymph nodes (primary complex / Ghon complex)
- Early hematogenous spread seeds the lungs and other organs (kidneys, bones, brain)
- Cell-mediated immunity develops within 2-10 weeks, usually halting multiplication
- ~90-95% of infected individuals develop latent TB infection (LTBI) without disease
- In ~5-10%, primary TB or subsequent reactivation TB develops
In the lung cavity:
- Bacilli spill into airways from caseous foci, multiply within the cavity, and discharge into the environment through coughing and talking
- In young children with poor natural immunity, hematogenous dissemination may result in fatal miliary TB or tuberculous meningitis
Role of Macrophages and Monocytes
- Alveolar macrophages phagocytose bacilli; alternatively activated macrophages are more susceptible to early growth
- Bactericidal activity mediated by reactive oxygen intermediates (ROI) and nitric oxide
- Cytokines secreted: TNF-α, IL-1 regulate release of reactive intermediates; TNF-α is key - too much leads to immunopathology, too little leads to inadequate containment
- Macrophages can undergo apoptosis as a defensive mechanism
- Neutrophils also involved, though timing and effectiveness remain uncertain
Role of T Lymphocytes
- CD4+ T lymphocytes are crucial - defects in CD4+ cells (e.g., HIV infection) explain inability to contain mycobacterial proliferation
- TH1 cells produce IFN-γ (activates macrophages) and IL-2
- TH2 cells produce IL-4, IL-5, IL-10, IL-13 and promote humoral immunity
- CD8+ T cells - cytotoxic responses, lysis of infected cells
- IFN-γ induces reactive oxygen/nitrogen intermediates and regulates bactericidal genes
- Granuloma formation: hallmark of host response, contains but may not eliminate infection
Clinical Features
Pulmonary TB (most common - ~2/3 of cases)
Symptoms:
- Productive cough (often weeks to months)
- Hemoptysis
- Fever, night sweats
- Weight loss, anorexia, fatigue ("consumption")
- Chest pain (with pleuritis)
- Dyspnea (extensive disease)
Chest X-ray findings:
- Primary TB: hilar/paratracheal lymphadenopathy, lower/mid-zone consolidation, pleural effusion
- Reactivation TB (most common form): upper lobe infiltrates, cavitation (pathognomonic), fibrosis, calcified nodules (Ghon complex)
- Miliary TB: diffuse bilateral 1-2 mm nodules ("millet seeds")
Extrapulmonary TB (up to 1/3 of cases)
Lymph node TB (scrofula): Most common extrapulmonary form; painless lymph node enlargement, mainly cervical; nodes may form cold abscesses and draining sinus tracts
Pleural TB: Unilateral effusion; may resolve spontaneously; high risk of developing pulmonary TB later if untreated
Skeletal TB (Pott's disease): Spine most commonly affected (lower thoracic); vertebral collapse, paravertebral "cold abscess," cord compression (Pott's paraplegia)
Meningeal TB: Most serious form; subacute presentation; basal meningitis, cranial nerve palsies, hydrocephalus; high mortality/morbidity; CSF: lymphocytosis, elevated protein, low glucose
Miliary TB: Hematogenous dissemination; fever, weight loss, dyspnea, hepatosplenomegaly; bilateral miliary pattern on CXR; associated with HIV and immunosuppression
Genitourinary TB: Dysuria, frequency, hematuria; "sterile pyuria"; calyceal destruction, hydronephrosis; urine AFB culture important
Pericardial TB: Constrictive pericarditis may develop; elevated JVP, Kussmaul's sign
Diagnosis
Latent TB Infection (LTBI) Diagnosis
-
Tuberculin Skin Test (TST / Mantoux):
- 5 TU PPD injected intradermally; read at 48-72 h
- Positive: ≥5 mm (HIV+, close contacts, immunosuppressed); ≥10 mm (high-risk groups, recent immigrants); ≥15 mm (low-risk)
- Limitations: false positives with BCG vaccination and NTM; false negatives in immunosuppressed patients
-
Interferon-γ Release Assays (IGRAs):
- QuantiFERON-TB Gold Plus and T-SPOT.TB
- More specific than TST (not affected by BCG); preferred in BCG-vaccinated individuals
- Cannot differentiate LTBI from active TB
- Reduced sensitivity in immunocompromised patients
- Cannot identify individuals with highest risk of progression
Active TB Diagnosis
-
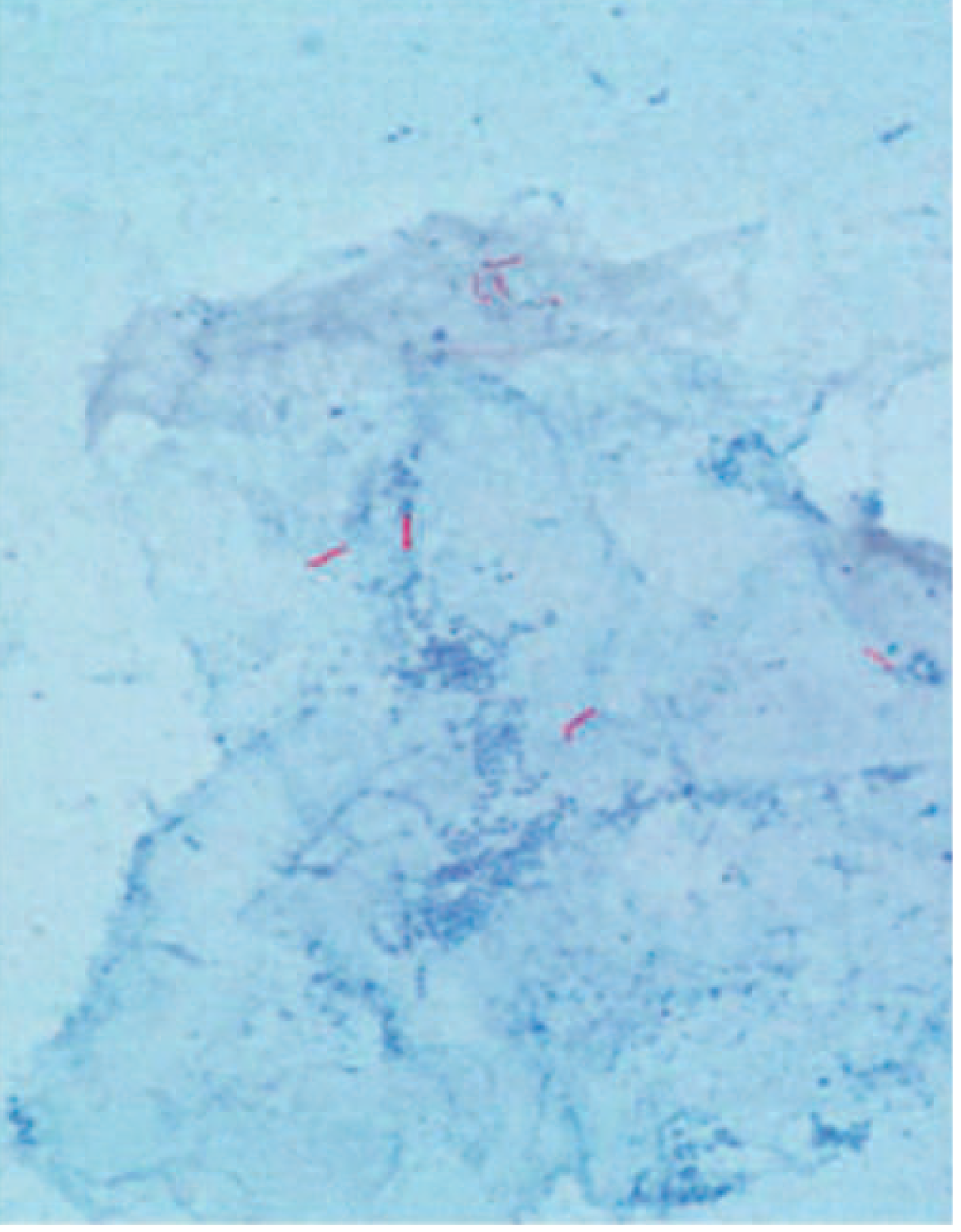
Sputum microscopy (AFB smear):
- Rapid, cheap; detects ~5,000-10,000 bacilli/mL
- Ziehl-Neelsen or fluorochrome staining
- Sensitivity ~50-80% in pulmonary TB; poor for extrapulmonary/paucibacillary disease
-
Mycobacterial culture:
- Gold standard; Lowenstein-Jensen medium (solid) or BACTEC/MGIT (liquid)
- More sensitive; allows drug susceptibility testing (DST)
- Takes 2-8 weeks (liquid) to 6-8 weeks (solid)
-
Molecular diagnostics (WHO-recommended):
- Xpert MTB/RIF (GeneXpert): Simultaneous detection of M. tuberculosis and rifampin resistance; results in ~2 hours; endorsed as initial diagnostic test by WHO
- Line probe assays (LPA): Detect resistance to rifampin and isoniazid (MDR screen)
- Whole genome sequencing (WGS): Increasingly used for comprehensive resistance profiling and outbreak investigation
-
Imaging: CXR essential; CT chest more sensitive for cavities, miliary pattern, mediastinal nodes
Treatment
Aims of TB Treatment
- Prevent morbidity and death, cure TB, prevent recurrences and emergence of drug resistance
- Interrupt transmission by rendering patients noninfectious
Standard Treatment for Drug-Susceptible TB
Four major first-line drugs: Isoniazid (H), Rifampin (R), Pyrazinamide (Z), Ethambutol (E)
| Phase | Drugs | Duration |
|---|---|---|
| Intensive (initial) phase | HRZE | 2 months |
| Continuation phase | HR | 4 months |
| Total standard duration | 6 months |
Extension of continuation phase to 7 months (total 9 months) for:
- Cavitary disease
- 2-month pyrazinamide course not completed
- Sputum cultures positive beyond 2 months (delayed conversion) - also warrants evaluation for resistance
Newer 4-month regimen (2020 multinational RCT):
- Daily rifapentine + isoniazid + pyrazinamide + moxifloxacin for 8 weeks, then rifapentine + isoniazid + moxifloxacin for 9 weeks
- Non-inferior to traditional 6-month HRZE - now has conditional WHO recommendation
Treatment of Latent TB Infection (LTBI)
| Regimen | Duration | Notes |
|---|---|---|
| Isoniazid + rifapentine (3HP) | 3 months, weekly | Regimen of choice in children >2 yrs and all adults including HIV+; NOT for pregnant women |
| Rifampin alone (4R) | 4 months, daily | Currently preferred over 9H in adults/children |
| Isoniazid + rifampin (3HR) | 3 months, daily | Effective, safe, tolerable |
| Isoniazid alone (6-9H) | 6-9 months | Historically standard; now less preferred |
| Rifapentine + isoniazid (1HP) | 1 month, daily | Non-inferior to 9H in HIV+ patients; included in 2020 WHO LTBI guidelines |
MDR-TB Treatment
MDR-TB = resistance to at least isoniazid and rifampin. WHO groups drugs for longer MDR-TB regimens (18-20 months):
| Group | Drugs |
|---|---|
| Group A (all three should be included) | Levofloxacin or moxifloxacin; Bedaquiline; Linezolid |
| Group B (at least one) | Clofazimine; Cycloserine or terizidone |
| Group C (to complete regimen when A/B unavailable) | Ethambutol; Delamanid; Pyrazinamide; Imipenem-cilastatin or meropenem; Amikacin; Ethionamide; p-aminosalicylic acid |
Kanamycin and capreomycin are NOT to be included in longer MDR regimens.
Shorter MDR regimen (6 months - BPaLM):
- Bedaquiline + pretomanid + linezolid ± moxifloxacin
- Represents a major advance; now endorsed by WHO for pre-XDR and XDR-TB
TB and HIV Co-infection
- HIV is the most powerful risk factor for progression from LTBI to active TB
- TB is the leading cause of death in HIV-positive persons
- CD4+ T cell depletion by HIV explains inability to contain mycobacterial proliferation
- Atypical presentation in advanced HIV: lower lobe disease, hilar adenopathy, absent cavitation, miliary pattern
- Both diseases treated simultaneously; ART initiation: within 2 weeks of starting TB treatment if CD4 <50 cells/μL; within 8-12 weeks if CD4 >50
- Immune reconstitution inflammatory syndrome (IRIS) can occur after ART initiation
Prevention
- BCG vaccination: Protects primarily against disseminated forms (miliary, meningitis) in children; limited efficacy against pulmonary TB in adults; not recommended in immunocompromised patients
- Infection control: Administrative, environmental, and personal protective measures in healthcare settings
- Treatment of LTBI: Most effective tool for elimination strategy
- Contact tracing and screening of high-risk populations
Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 183 - Raviglione & Gori; Chapter 186 - Antimycobacterial Agents
This is a shared conversation. Sign in to Orris to start your own chat.