Hemorrhagic shock
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hemorrhagic shock"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full response.
Hemorrhagic Shock
Hemorrhagic shock is a state of life-threatening circulatory failure caused by rapid, significant loss of intravascular blood volume, leading to inadequate oxygen delivery to tissues, cellular hypoxia, and - if uncorrected - irreversible organ failure and death.
1. Definition and Overview
Hemorrhagic shock results from a rapid reduction in intravascular blood volume from any cause. Rapid hemorrhage first triggers increased cardiac contractility and heart rate (HR), followed by baroreceptor activation and peripheral vasoconstriction. An initial slight increase in diastolic BP with narrowing of pulse pressure progresses to decreased ventricular filling, reduced cardiac output, and then a fall in systolic BP. Critically, HR and BP responses are notoriously variable - no firm conclusion can be made at the bedside about the presence or degree of hemorrhagic shock from vital signs alone.
- ROSEN's Emergency Medicine, p. 58
2. Pathophysiology
Macrocirculatory Response
An imbalance develops between systemic O2 delivery and O2 consumption. Blood loss causes hemodynamic instability, coagulopathy, decreased O2 delivery, reduced tissue perfusion, and cellular hypoxia. The initial response is mediated by the neuroendocrine system: reduced arterial pressure triggers vasoconstriction and catecholamine release to preserve flow to the heart, kidney, and brain at the expense of other vascular beds.
Released hormones and mediators include: renin, angiotensin, vasopressin (ADH), growth hormone, glucagon, cortisol, epinephrine, and norepinephrine. As oxygen debt mounts, damage-associated molecular patterns (DAMPs), mitochondrial DNA, and formyl peptides contribute to systemic inflammatory response.
- Miller's Anesthesia, 10e, p. 9383
Microcirculatory Response
Individual ischemic cells take up interstitial fluid, further depleting intravascular volume. Cellular edema may restrict blood flow in adjacent capillaries, causing the "no-reflow" phenomenon - preventing reversal of ischemia even after macroperfusion is restored.
Ischemic cells produce lactate and free radicals which accumulate in circulation. They also release inflammatory factors: prostacyclin, thromboxane, prostaglandins, leukotrienes, endothelin, complement, interleukins, TNF, and others. This inflammatory cascade becomes a disease process independent of its origin and lays the foundation for multiple organ failure (MOF).
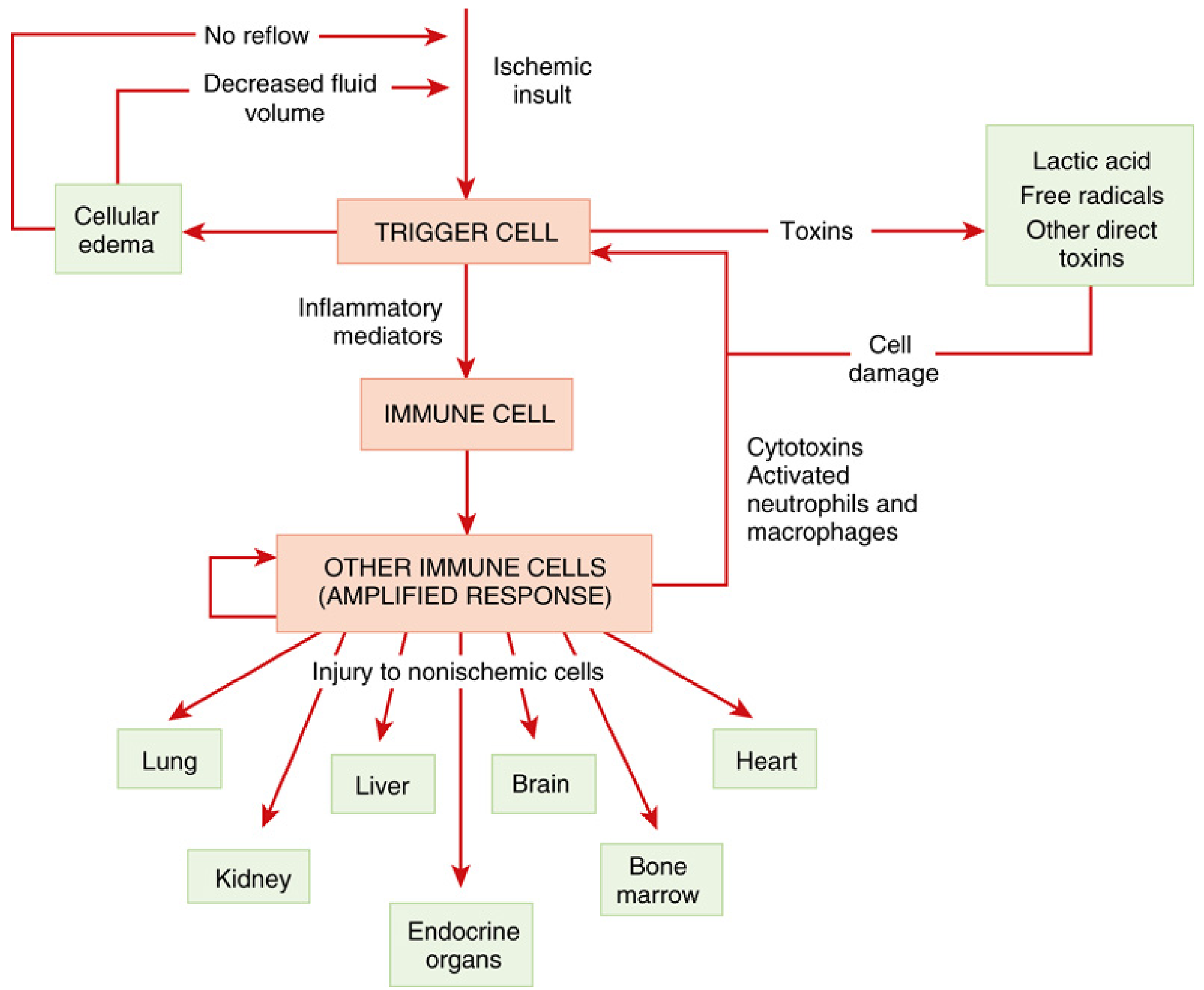
The "shock cascade" - ischemia triggers a self-amplifying immune response injuring non-ischemic organs. (Miller's Anesthesia, 10e)
The Role of Base Deficit and Lactate
Even before cardiac output declines, blood flow is redirected away from non-critical organs, which begin producing lactic acid. Acidosis often precedes any significant decrease in cardiac output. Bicarbonate ions buffer the blood pH, keeping it near neutral even as lactic acid accumulates. The base deficit (amount of strong base needed to normalize 1 L of blood to pH 7.4) represents an index of how far the bloodstream has depleted this reserve.
-
Normal base deficit: more positive than -2 mEq/L
-
A more negative base deficit can appear early in hemorrhage, even while blood pH and BP remain normal
-
The base deficit therefore distinguishes trivial blood loss from clinically significant hemorrhage
-
ROSEN's Emergency Medicine, p. 58
3. Progressive vs. Nonprogressive Shock
This is one of the most important physiologic concepts in understanding hemorrhagic shock:

Figure 24.2 from Guyton & Hall - Blood loss above a critical threshold shifts the patient from compensated to progressive (irreversible) shock.
Nonprogressive (Compensated) Shock: If blood loss does not cross a critical threshold, compensatory mechanisms prevail:
- Baroreceptor reflexes - powerful sympathetic stimulation (activated within 30 seconds)
- CNS ischemic response - even more powerful sympathetic activation (triggered when MAP falls below ~50 mmHg)
- Reverse stress-relaxation - blood vessels contract around diminished blood volume
- Renin-angiotensin-aldosterone activation - arteriolar constriction + salt/water retention
- Vasopressin (ADH) secretion - arteriolar/venous constriction + renal water retention
- Catecholamine release - increased HR and vasoconstriction
- Fluid shifts - absorption from interstitial spaces and intestinal tract, thirst
Progressive Shock: Beyond the critical threshold, shock causes more shock via positive feedback vicious cycles:
-
Decreased coronary flow → myocardial depression → further decreased cardiac output
-
Vasomotor center failure (ischemia of medullary centers)
-
Cardiac depression from acidosis, free radicals, and inflammatory mediators
-
Breakdown of gut barrier → bacterial translocation → potentiates ARDS
-
Guyton and Hall Textbook of Medical Physiology, pp. 300-302
4. Organ-Specific Responses
| Organ | Response |
|---|---|
| Brain | Prime trigger of neuroendocrine response; cortical reflexes depressed during hypotension - reversible with mild hypoperfusion, permanent with prolonged ischemia |
| Heart | Initially protected; maintained or increased coronary flow until late stages; lactate/free radicals act as negative inotropes - terminal event in shock spiral |
| Kidney | Maintains GFR via selective vasoconstriction; prolonged hypotension → renal cell hibernation → tubular epithelial necrosis → renal failure; high incidence of acute adrenal insufficiency (86% in one observational study) |
| Lung | Filter for inflammatory by-products; neutrophil/platelet aggregation → increased capillary permeability → ARDS; sentinel organ for MOD |
| Gut | Earliest organ affected; intense vasoconstriction → "no-reflow" → intestinal cell death → breakdown of gut barrier → bacterial translocation → potentiates ARDS and MOD |
| Liver | Complex microcirculation susceptible to reperfusion injury; contributes to inflammatory response; failure of synthetic function (coagulopathy) |
- Miller's Anesthesia, 10e, pp. 9385-9387
5. Classification of Hemorrhagic Shock
The ATLS classification based on volume of blood loss:
| Class I | Class II | Class III | Class IV | |
|---|---|---|---|---|
| Blood loss (mL) | Up to 750 | 750-1500 | 1500-2000 | >2000 |
| Blood loss (% BV) | Up to 15% | 15-30% | 30-40% | >40% |
| Pulse rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal/increased | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | >20-30 | 30-40 | >35 |
| Urine output (mL/h) | >30 | 20-30 | 5-15 | Negligible |
| CNS/mental status | Slightly anxious | Mildly anxious | Anxious + confused | Confused + lethargic |
Note: Pregnant patients maintain a larger circulating blood volume and must lose a relatively larger volume before manifesting signs of hypovolemia.
- Schwartz's Principles of Surgery, 11e, p. 220
6. Initial Resuscitation Strategy
Patients can be stratified by their response to initial fluid resuscitation:
- Responders: Vital signs normalize - unlikely to have significant ongoing hemorrhage; proceed with orderly evaluation
- Transient responders: Initially improve, then deteriorate hemodynamically - challenging to triage; likely ongoing hemorrhage
- Nonresponders: Persistent hypotension despite aggressive resuscitation - mandate immediate source identification and intervention
Hemorrhage Control
Five potential sources of blood loss: scalp, chest, abdomen, pelvis, extremities. Estimated blood loss by fracture site:
-
Each rib fracture: 100-200 mL
-
Tibial fracture: 300-500 mL
-
Femoral fracture: up to 1500 mL
-
Pelvic fracture: massive, potentially exsanguinating
-
Schwartz's Principles of Surgery, 11e, pp. 220-221
7. Resuscitation: Blood Products and Damage Control
In hemorrhagic shock, blood products are the resuscitative fluid of choice. Crystalloid administration leads to anemia and coagulopathy.
Component Therapy
- Massive transfusion protocol (MTP): 1:1:1 ratio of FFP : pRBCs : platelets
- Early empiric use of type O RBCs (O-negative for women of childbearing age) and thawed AB plasma at a 2:1 ratio pending type-specific blood
Whole Blood
Recent data suggest that whole blood may be superior to component therapy when available in hemorrhagic shock.
Viscoelastic Testing (TEG/ROTEM)
- TEG and ROTEM provide dynamic, real-time assessment of clotting ability and strength
- Guide targeted use of FFP, cryoprecipitate, platelets, or tranexamic acid (TXA)
- Mortality benefit demonstrated vs. empiric MTP in penetrating trauma patients receiving >10 units pRBCs (33.3% vs. 54.1% in one 2013 study)
- Endorsed by the Eastern Association for the Surgery of Trauma (EAST) guidelines
Tranexamic Acid (TXA)
TXA is an important adjunct in hemorrhagic shock. Prompt recognition of fibrinolysis via viscoelastic assays enables timely TXA administration.
Vasopressors
While evidence for early vasopressors in hemorrhagic shock is limited, they may be a necessary temporizing adjunct. A specific vasopressin-deficient state may occur in prolonged shock where vasopressin administration is helpful.
- Sabiston Textbook of Surgery, pp. 2892-2903
8. Anesthetic Considerations
Any IV anesthetic given to a trauma patient in hemorrhagic shock may potentiate profound hypotension and even cardiac arrest by inhibiting circulating catecholamines.
- Etomidate is preferred for induction - maintains hemodynamics better than alternatives in hemorrhagic shock
- Opioids should be given in reduced doses to minimize hemodynamic consequences and prevent prolonged effect
- Propofol is particularly hazardous - avoid or use with extreme caution
- Miller's Anesthesia, 10e, pp. 4687-4696
9. Complications
| Complication | Mechanism |
|---|---|
| ARDS | Pulmonary neutrophil/platelet aggregation; gut bacterial translocation; inflammatory mediators |
| AKI | Renal hypoperfusion → tubular necrosis; relative adrenal insufficiency compounds this |
| Coagulopathy / "Lethal Triad" | Dilution (crystalloid), acidosis, hypothermia - each impairs clotting; the triad is self-reinforcing |
| Multiple organ failure (MOF) | Progressive inflammatory cascade; lung is the sentinel organ |
| "No-reflow" phenomenon | Cellular edema in capillary beds prevents reversal of ischemia even after macroperfusion is restored |
Key References:
- Guyton and Hall Textbook of Medical Physiology - Chapter 24: Circulatory Shock
- Schwartz's Principles of Surgery, 11e - Chapter 7: Trauma
- Miller's Anesthesia, 10e - Chapter 62: Pathophysiology and Resuscitation from Hemorrhagic Shock
- Sabiston Textbook of Surgery - Hemorrhagic Shock management
- ROSEN's Emergency Medicine - Hemorrhagic Shock
Causes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I have comprehensive data. Here is the full breakdown of causes of hemorrhagic shock.
Causes of Hemorrhagic Shock
Hemorrhagic shock arises whenever blood loss - from any site, internal or external - exceeds the body's compensatory capacity. The causes are best organized by anatomical category and clinical setting.
1. Traumatic Causes
Trauma is the most common cause overall, especially in young adults. ATLS identifies five anatomical compartments where life-threatening blood can accumulate:
External / Compressible Hemorrhage
- Scalp lacerations (highly vascular; easily underestimated)
- Extremity wounds - lacerations, amputations, penetrating injuries
- Open fractures with soft-tissue disruption
Thoracic (Chest)
- Hemothorax - blunt or penetrating trauma to lung parenchyma, intercostal vessels, or great vessels
- Massive hemothorax: initial chest tube output >1 L is an indication for immediate thoracotomy
- Aortic injury (blunt deceleration or penetrating)
- Cardiac laceration
Abdominal / Peritoneal
- Solid organ injury: spleen (most common in blunt abdominal trauma), liver, kidneys
- Mesenteric vascular injury
- Penetrating injuries: gunshot/stab wounds to abdominal viscera and vasculature
- Extensive hemoperitoneum detected on eFAST
Pelvic
- Pelvic fractures - venous plexus and internal iliac artery disruption; potentially exsanguinating
- Pelvic fractures are notorious for massive occult blood loss - pelvis can accommodate several liters
- Wrapping with a pelvic binder is an immediate temporizing measure
Extremity Fractures (Long Bone)
-
Each rib fracture: 100-200 mL
-
Tibial fracture: 300-500 mL
-
Femoral fracture: up to 1,500 mL
-
When fractures are additive, cumulative blood loss can be hemodynamically significant
-
Schwartz's Principles of Surgery, 11e, pp. 220-221
2. Gastrointestinal Hemorrhage
GI bleeding is among the most common non-traumatic causes of hemorrhagic shock.
Upper GI Bleeding (proximal to ligament of Treitz)
| Cause | Notes |
|---|---|
| Peptic ulcer disease (PUD) | Most common cause (~40% of upper GI hemorrhage); includes gastric and duodenal ulcers |
| Esophageal/gastric varices | Cause of upper GI bleeding in cirrhotic patients ~59% of the time; high mortality |
| Erosive esophagitis / gastritis | Including stress ulcers in critically ill patients |
| Mallory-Weiss tears | Mucosal lacerations at gastroesophageal junction from retching |
| Dieulafoy's lesion | Aberrant submucosal artery; can cause massive occult bleeding |
| Aortoenteric fistula | Rare but immediately life-threatening; especially after prior aortic graft surgery |
Lower GI Bleeding (distal to ligament of Treitz)
| Cause | Notes |
|---|---|
| Diverticular bleeding | Most common cause of massive lower GI hemorrhage in adults |
| Angiodysplasia (arteriovenous malformations) | Common in elderly |
| Colorectal malignancy | Usually slower bleeding but can be acute |
| Ischemic colitis | Especially in elderly or post-aortic surgery |
| Inflammatory bowel disease | Ulcerative colitis > Crohn's disease |
| Meckel's diverticulum | Classic cause in children and young adults |
- Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
3. Obstetric and Gynecological Causes
A major cause of hemorrhagic shock in women of reproductive age. "Bleeding during the third trimester should always be considered an emergency because shock may occur within minutes." (Roberts and Hedges' Clinical Procedures in Emergency Medicine)
| Cause | Notes |
|---|---|
| Postpartum hemorrhage (PPH) | Most common obstetric cause; defined as >500 mL (vaginal) or >1000 mL (C-section) blood loss; causes include uterine atony, retained placenta, lacerations |
| Placenta previa | Painless antepartum hemorrhage; placenta overlies cervical os |
| Placental abruption (abruptio placentae) | Painful antepartum hemorrhage; premature separation of placenta |
| Uterine rupture | Risk in scarred uterus (prior C-section); catastrophic hemorrhage |
| Ruptured ectopic pregnancy | Classic presentation: amenorrhea + abdominal pain + hemodynamic instability + positive pregnancy test; a true emergency |
| Ruptured ovarian cyst / hemorrhagic corpus luteum | Can cause significant intraperitoneal bleeding |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine; Miller's Anesthesia, 10e
4. Vascular Causes
| Cause | Notes |
|---|---|
| Ruptured abdominal aortic aneurysm (AAA) | Classically presents as hypotension + back/flank pain + pulsatile mass; immediately life-threatening |
| Ruptured thoracic aortic aneurysm | Associated with hypertension and connective tissue disorders (Marfan, Ehlers-Danlos) |
| Aortoenteric fistula | Often secondary to prior aortic graft; "herald bleed" followed by exsanguination |
| Splenic artery aneurysm rupture | Rare; risk increased in pregnancy; hemoperitoneum |
| Mesenteric artery or vein rupture | Post-traumatic or spontaneous |
| Arteriovenous malformations | In any organ system |
- Current Surgical Therapy, 14e, p. 2377
5. Iatrogenic / Procedural Causes
- Post-surgical hemorrhage (abdominal, pelvic, thoracic, vascular surgery)
- Post-procedural bleeding (endoscopy, biopsy, arterial line placement, cardiac catheterization)
- Anticoagulant-related hemorrhage (warfarin, heparin, DOACs) - particularly in elderly patients
- Thrombolytic therapy complications
6. Spontaneous / Medical Causes
| Cause | Notes |
|---|---|
| Hemophilia A/B and other coagulation factor deficiencies | Spontaneous or post-minor trauma hemorrhage |
| Severe thrombocytopenia | ITP, TTP, HIT, bone marrow failure |
| Anticoagulant overdose | Warfarin, heparin, DOACs |
| Disseminated intravascular coagulation (DIC) | Consumption of clotting factors; paradoxically both thrombotic and hemorrhagic |
| Hepatic failure | Impaired synthesis of coagulation factors (I, II, V, VII, IX, X) + portal hypertension |
| Spontaneous retroperitoneal hemorrhage | Can be massive; often anticoagulant-related or from adrenal hemorrhage |
| Intracranial hemorrhage | Subarachnoid or intracerebral hemorrhage does not directly cause hemorrhagic shock (skull is a closed box) but can cause neurogenic shock and coagulopathy |
7. Summary Mnemonic: "TRAUMA + GI + OB + VASC"
| Category | Key Examples |
|---|---|
| Trauma | Chest, abdomen, pelvis, long bones, external wounds |
| GI bleeding | PUD, varices, diverticular disease, Mallory-Weiss |
| Obstetric/gynecologic | PPH, placenta previa, abruption, ruptured ectopic |
| Vascular | Ruptured AAA, aortoenteric fistula, splenic aneurysm |
| Iatrogenic | Post-surgical, anticoagulation |
| Coagulopathy | Hemophilia, DIC, liver failure |
The most common causes encountered in emergency settings are trauma (all age groups), GI bleeding (especially in older adults), and obstetric hemorrhage (in women of childbearing age). Tintinalli's notes that massive transfusion protocols originally developed for trauma are now routinely applied to postpartum hemorrhage and massive GI bleeding as well, reflecting the shared final common pathway of hemorrhagic shock regardless of cause.
- Tintinalli's Emergency Medicine, p. 1538; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.