Explain 10 heart diseases with ecg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG patterns 10 heart diseases STEMI atrial fibrillation heart block WPW Brugada long QT ventricular tachycardia hypertrophic cardiomyopathy pericarditis
I now have comprehensive information from multiple authoritative textbooks (Braunwald's, Harrison's, Tintinalli's, Fuster & Hurst's, Goldman-Cecil, Ganong's). Let me compose a detailed, well-organized answer covering 10 heart diseases with their ECG findings.
10 Heart Diseases and Their ECG Findings
Here is a thorough breakdown of 10 major cardiac conditions, each explained with its pathophysiology, clinical features, and characteristic ECG pattern.
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causes transmural (full-thickness) myocardial ischemia and necrosis. It is a medical emergency requiring immediate reperfusion.
ECG findings (evolving sequence):
| Phase | ECG Changes |
|---|---|
| Hyperacute (minutes) | Tall, peaked "hyperacute" T waves |
| Acute (hours) | ST-segment elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in precordial leads; reciprocal ST depression in opposite leads |
| Established | Pathological Q waves (width ≥40 ms, depth ≥25% of R wave) develop |
| Reperfusion/Resolution | ST normalizes; T-wave inversions persist |
Lead localization:
- Inferior MI (RCA): II, III, aVF - with reciprocal depression in I, aVL
- Anterior MI (LAD): V1-V4
- Lateral MI (LCx): I, aVL, V5-V6
- Posterior MI: dominant R wave in V1-V2, ST depression anteriorly (mirror image)
"Profound ST elevation or depression in multiple leads usually indicates very severe ischemia. The division of acute myocardial infarction into ST-segment elevation and non-ST elevation types is useful since the consistent efficacy of primary PCI in STEMI makes prompt identification imperative." - Harrison's Principles of Internal Medicine, 22E
Key pearl: Right ventricular infarction accompanies inferior STEMI - recognized by ST elevation in right-sided leads (V3R, V4R). This changes management (avoid nitrates and diuretics).
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) & Unstable Angina
What it is: Partial occlusion of a coronary artery causing subendocardial ischemia. Troponin rises in NSTEMI but not in unstable angina.
ECG findings:
- ST depression (horizontal or downsloping) ≥0.5 mm in ≥2 contiguous leads - this is the hallmark
- T-wave inversions - particularly deep, symmetric inversions in precordial leads suggest proximal LAD disease (Wellens syndrome pattern)
- No pathological Q waves (distinguishes from STEMI)
- ECG may be completely normal in up to 6% of cases
"The diagnosis of NSTEMI depends on abnormal elevation of cardiac biomarkers but may include ECG changes not meeting criteria for STEMI." - Tintinalli's Emergency Medicine
Wellens Syndrome (critical LAD stenosis): Biphasic or deeply inverted T waves in V2-V3 during pain-free period - indicates critical proximal LAD stenosis about to cause a large anterior MI.
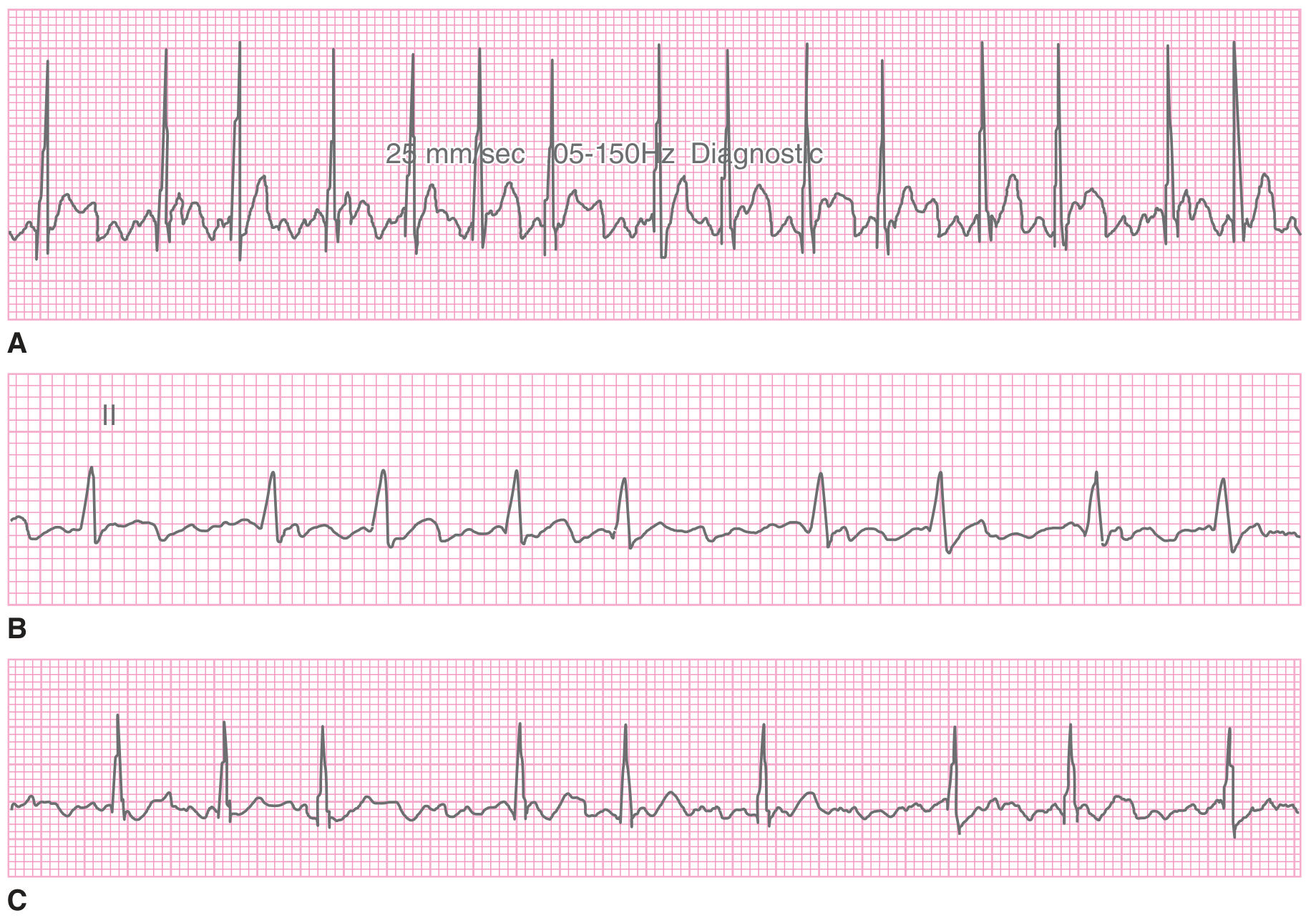
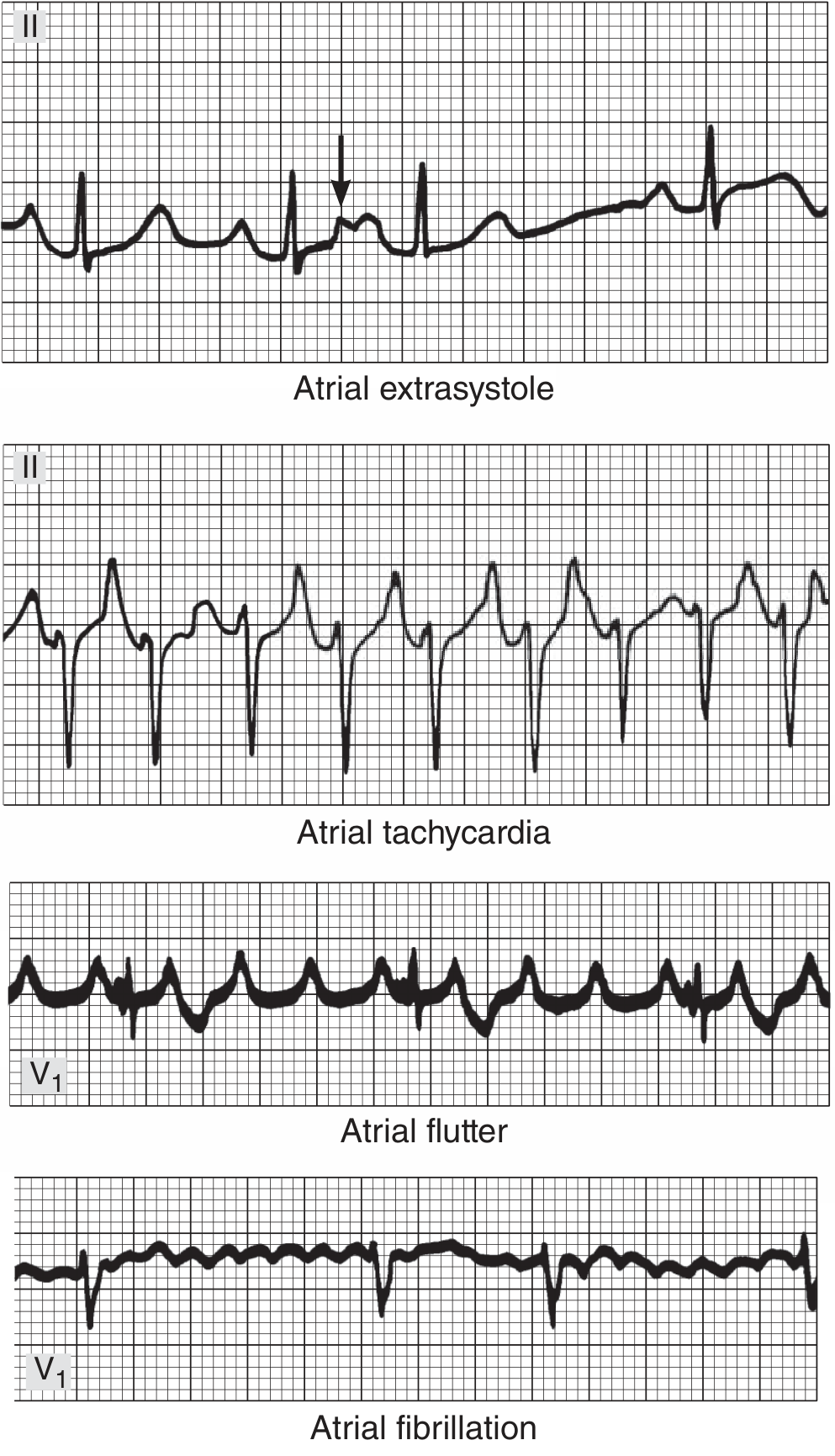
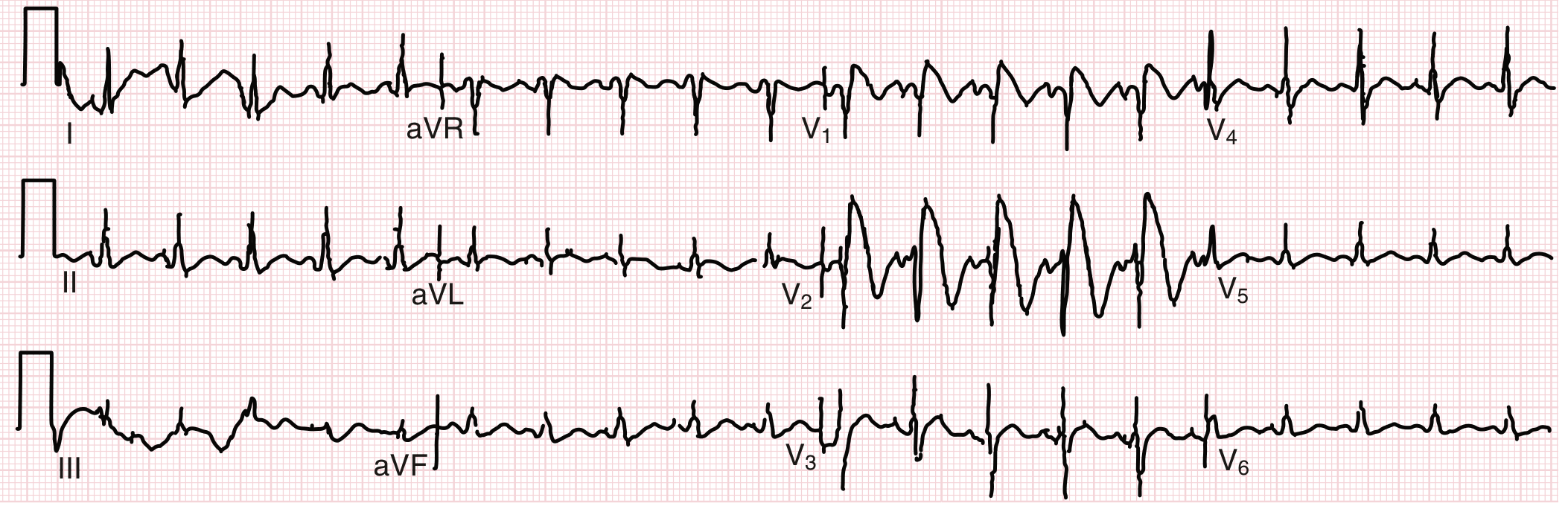
3. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized electrical activity in the atria producing an irregular ventricular response. Most common sustained arrhythmia, affecting >33 million people worldwide.
ECG findings:
- Absent P waves - replaced by irregular fibrillatory baseline ("f waves") at 350-600 bpm, best seen in V1
- Irregularly irregular RR intervals - the hallmark finding; no two consecutive RR intervals are equal
- Narrow QRS (unless aberrant conduction or bundle branch block)
- Ventricular rate typically 100-160 bpm if uncontrolled
Rate categories:
- Rapid AF: ventricular rate >100 bpm
- Controlled AF: ventricular rate 60-100 bpm
- AF with WPW: extremely rapid, irregular, wide-complex - life-threatening (avoid AV nodal agents)
4. Atrial Flutter
What it is: A macro-reentrant circuit in the right atrium, typically cycling at 250-350 bpm. Often converts to AF or sinus rhythm.
ECG findings:
- Classic "sawtooth" flutter waves (F waves) at ~300 bpm, best seen in leads II, III, aVF
- Regular or regularly-irregular ventricular response
- Most commonly 2:1 conduction (ventricular rate ~150 bpm) - always consider flutter when rate is 150 bpm
- QRS usually narrow
Key pearl: A ventricular rate of exactly 150 bpm with narrow QRS should always raise suspicion for 2:1 atrial flutter - look carefully for flutter waves buried in QRS or T waves.
5. Complete (Third-Degree) Heart Block
What it is: No impulses conduct from atria to ventricles through the AV node. Atria and ventricles beat independently - "AV dissociation." Causes include ischemia (inferior MI), degeneration (Lev/Lenegre disease), drugs, infection (Lyme carditis), and infiltrative disease.
ECG findings (from Tintinalli's Emergency Medicine):
| Feature | Finding |
|---|---|
| P waves | Regular, independent atrial rate (usually 60-100 bpm) |
| QRS complexes | Regular, slow escape rhythm |
| PR interval | Variable - no consistent relationship between P and QRS |
| QRS morphology | Narrow if junctional escape (40-60 bpm); wide and bizarre if ventricular escape (<40 bpm) |
- AV dissociation is the defining feature: P waves "march through" QRS complexes with no fixed relationship
- Junctional escape (narrow QRS) is more stable than ventricular escape (wide QRS)
- Often symptomatic: syncope, presyncope, fatigue; requires permanent pacemaker
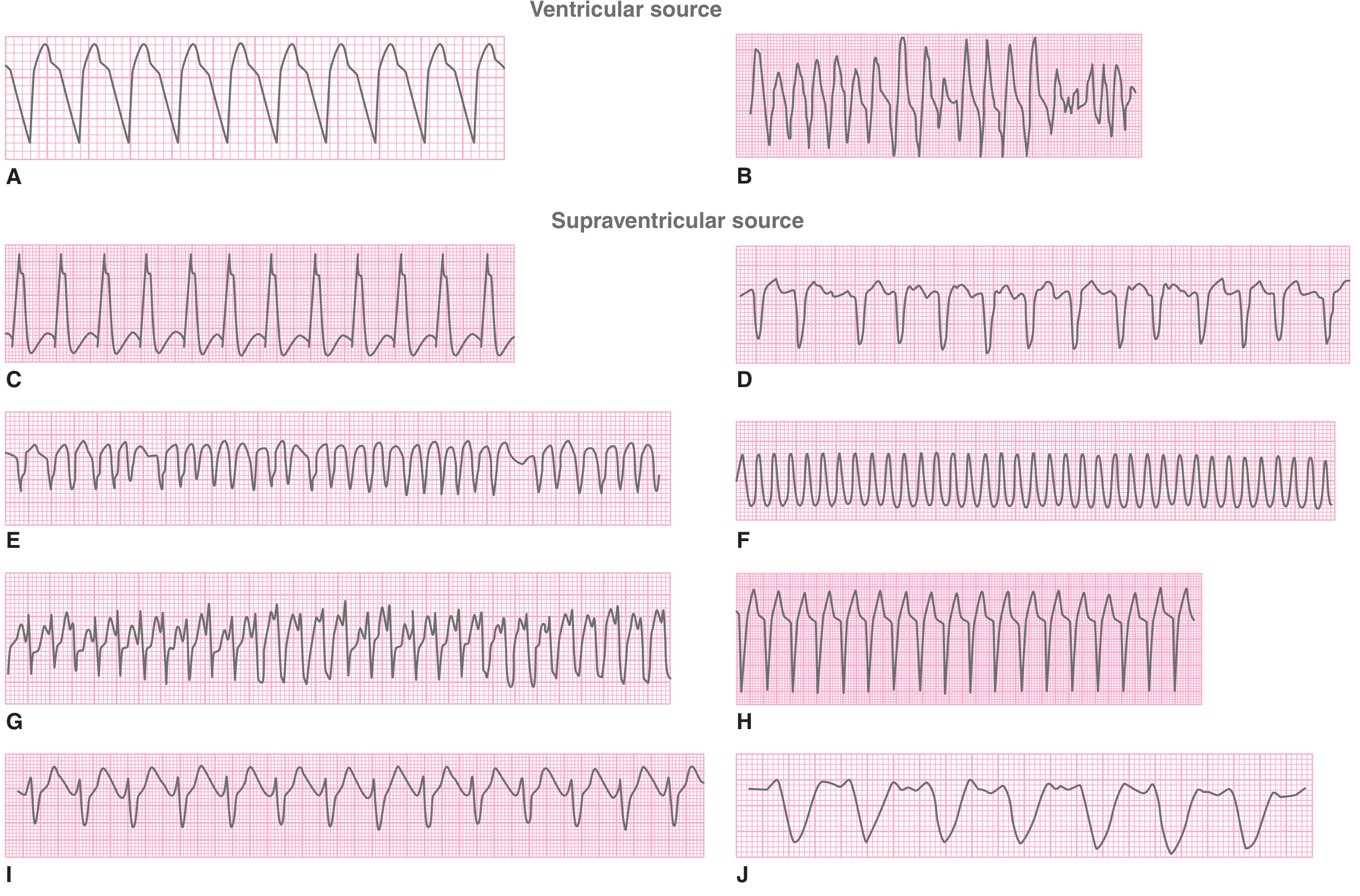
6. Ventricular Tachycardia (VT) and Ventricular Fibrillation (VF)
What it is: VT - rapid, dangerous rhythm originating below the bundle of His. VF - chaotic ventricular electrical activity causing cardiac arrest. Common causes include post-MI scar, cardiomyopathy, channelopathies (Long QT, Brugada).
VT ECG findings:
- Wide QRS (≥120 ms) at rate >100 bpm (usually 140-220 bpm)
- AV dissociation (P waves at different rate, not related to QRS) - most specific finding
- Fusion beats and capture beats - pathognomonic when present
- Brugada's criteria for VT: RS interval >100 ms in any precordial lead, AV dissociation, QRS morphology not fitting typical LBBB or RBBB pattern
- Axis may be markedly abnormal (northwest axis "no man's land")
VF ECG findings:
- Completely chaotic, irregular deflections with no discernible P waves, QRS, or T waves
- Coarse VF: large amplitude deflections (early, more likely to respond to defibrillation)
- Fine VF: small amplitude deflections (late, worse prognosis)
Note: Treat any wide-complex tachycardia as VT until proven otherwise.
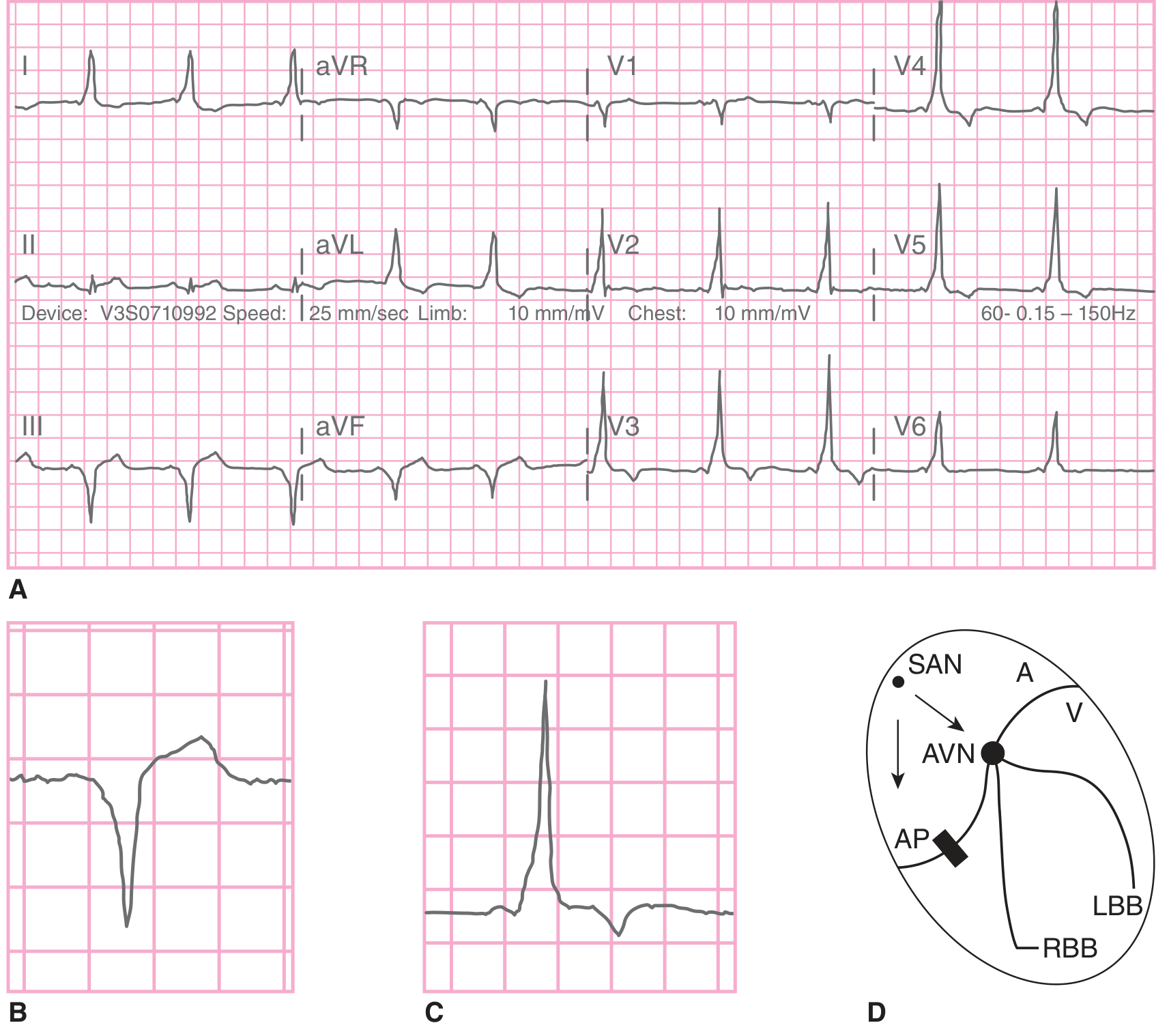
7. Wolff-Parkinson-White (WPW) Syndrome
What it is: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Can cause dangerous tachyarrhythmias. Found in ~1-3/1000 people.
ECG findings (the WPW triad in sinus rhythm):
| Feature | Finding |
|---|---|
| PR interval | Short (<120 ms) - bypass tract conducts faster than AV node |
| Delta wave | Slurred upstroke of the QRS - slow conduction through ventricular myocardium before normal conduction takes over |
| QRS duration | Widened (≥120 ms) due to delta wave |
- Secondary ST-T wave changes discordant to delta wave
- Pseudo-infarction pattern: delta waves can mimic Q waves (especially inferior or lateral leads)
- During SVT: orthodromic AVRT = narrow QRS, retrograde P after QRS; antidromic AVRT = very wide, bizarre QRS (difficult to distinguish from VT)
- AF with WPW: irregular, very rapid (>250 bpm), bizarre wide-complex tachycardia - life-threatening
"Baseline ECG abnormalities during normal sinus rhythm may reveal a combination of a short PR interval and a delta wave." - Symptom to Diagnosis, 4th Edition
8. Long QT Syndrome (LQTS)
What it is: Delayed ventricular repolarization, either congenital (channelopathy - LQT1-15 subtypes) or acquired (drugs, electrolyte disturbances). Predisposes to torsades de pointes (TdP) and sudden cardiac death.
ECG findings:
- Prolonged QTc interval - primary finding
- QTc >450 ms in males
- QTc >460 ms in females (QTc >500 ms = high-risk for TdP)
- Torsades de pointes (TdP): Polymorphic VT where QRS complexes appear to "twist" around the isoelectric line, at 200-250 bpm - hallmark arrhythmia of LQTS
- T-wave morphology varies by subtype:
- LQT1: Broad-based T wave with long T-wave duration
- LQT2: Notched or biphasic T waves
- LQT3: Late-onset T wave with prolonged isoelectric ST segment (triggered by bradycardia/sleep)
- U waves may be prominent
"Long QT syndrome is characterized by prolongation of the corrected QT interval, syncope, and sudden death caused by torsades de pointes and ventricular fibrillation." - Tintinalli's Emergency Medicine
Common acquired causes: Quinidine, sotalol, amiodarone, macrolides, antipsychotics, hypokalemia, hypomagnesemia.
9. Brugada Syndrome
What it is: A sodium channelopathy (SCN5A gene mutation in ~25% of cases) causing characteristic ECG changes and high risk of sudden cardiac death from VF, predominantly in young Asian males. Often manifests at night or during fever.
ECG findings:
- Type 1 (diagnostic - "coved" pattern): Coved ST-segment elevation ≥2 mm followed by negative T wave in V1-V2 (and occasionally V3); often with incomplete RBBB morphology - this is the only diagnostic pattern
- Type 2 ("saddle-back" pattern): Saddle-back ST elevation ≥2 mm in V1-V2; not diagnostic alone, but can convert to Type 1 with sodium-channel blockers (e.g., flecainide, ajmaline challenge)
- Type 3: Saddle-back or coved ST elevation <1 mm - non-diagnostic
"Brugada syndrome is a congenital sudden death syndrome involving characteristic electrocardiographic abnormalities. These typically include ST-segment elevation (unrelated to ischemia, electrolyte abnormalities, or structural heart disease) in the right precordial (V1 to V3) leads of the ECG." - Braunwald's Heart Disease
Key pearls:
- ECG pattern can be intermittent - fever, autonomic tone, and sodium-channel blockers can unmask it
- A pseudo-RBBB morphology: NOT true RBBB but mimics it
- Definitive treatment: implantable cardioverter-defibrillator (ICD)
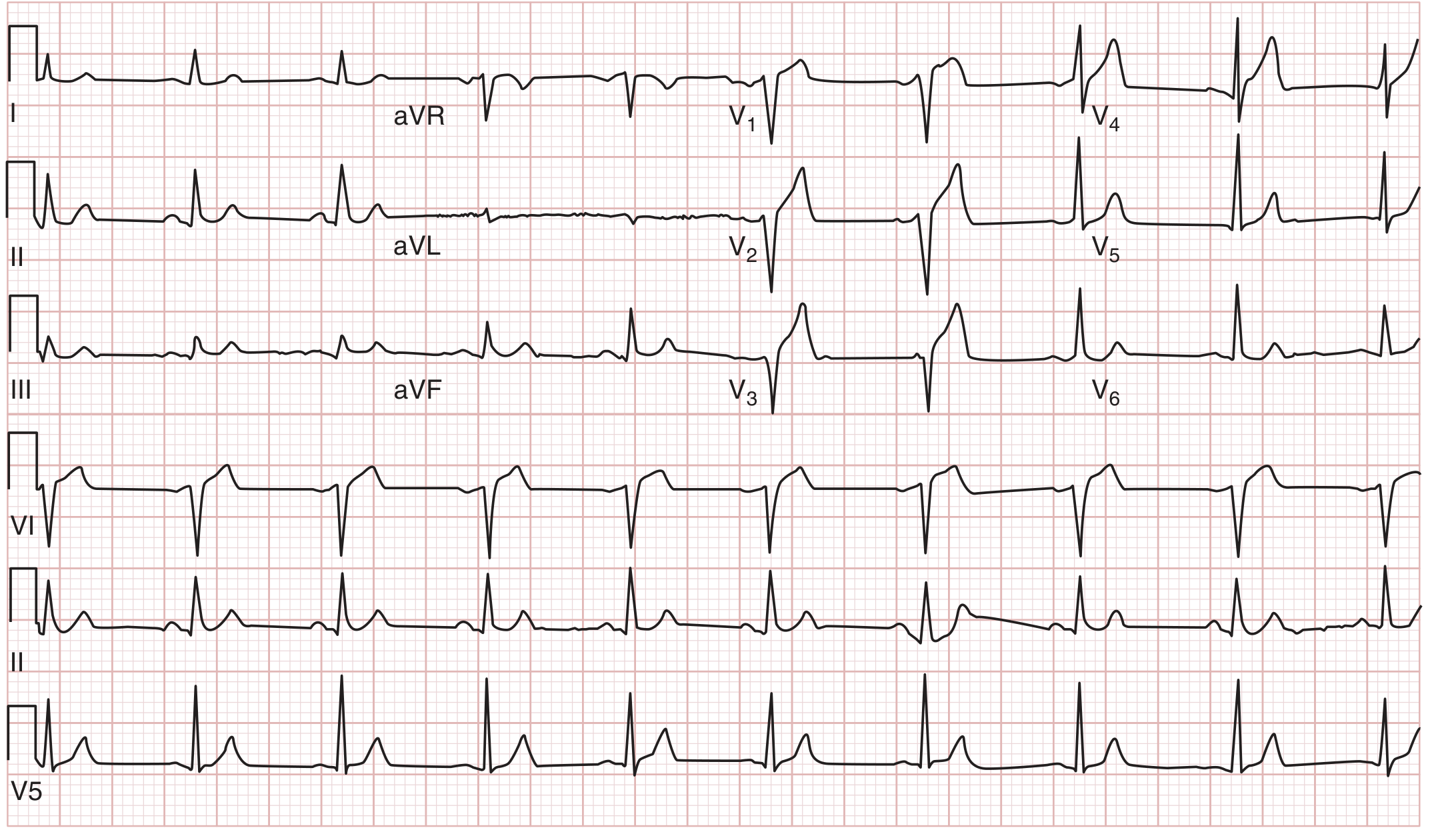
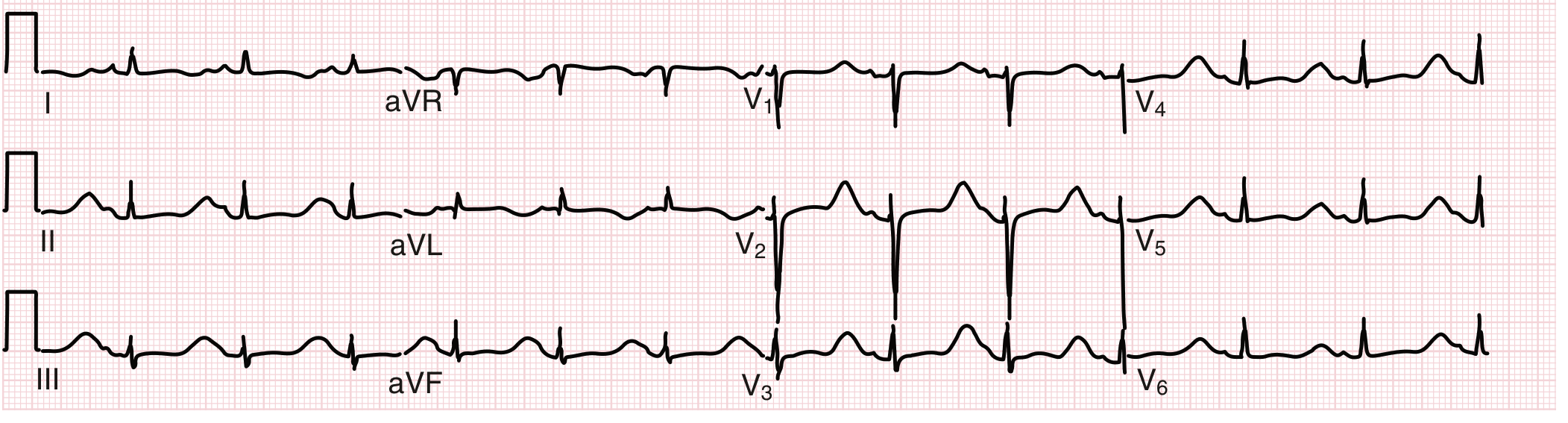
10. Pericarditis (Acute)
What it is: Inflammation of the pericardium, usually viral (Coxsackievirus, echovirus), also autoimmune, post-MI (Dressler's), or idiopathic. ECG changes reflect epicardial inflammation.
ECG findings (classic 4-stage evolution):
| Stage | Timing | ECG Finding |
|---|---|---|
| Stage 1 | Days 1-2 | Diffuse ST elevation (saddle-shaped/concave upward) in nearly all leads except aVR and V1; PR depression in most leads (PR elevation in aVR) |
| Stage 2 | Days 3-7 | ST returns to baseline; PR depression persists |
| Stage 3 | Weeks 1-3 | Diffuse T-wave inversions (after ST has normalized, unlike MI where inversion occurs while ST is still elevated) |
| Stage 4 | Weeks-months | ECG normalizes |
Key distinguishing features from STEMI:
- ST elevation in pericarditis is diffuse (not localized to one territory) and concave upward ("saddle-shaped")
- PR segment depression - unique to pericarditis (reflects atrial inflammation), most obvious in lead II
- No reciprocal ST depression (except in aVR and V1)
- No pathological Q waves
- Spodick's sign: Downsloping TP segment in early stages (present in ~80% of cases)
Quick Reference Summary
| # | Condition | Hallmark ECG Feature |
|---|---|---|
| 1 | STEMI | Localized convex ST elevation + Q waves |
| 2 | NSTEMI/UA | ST depression, T-wave inversions, no Q waves |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular RR |
| 4 | Atrial Flutter | Sawtooth F waves ~300 bpm, 2:1 block |
| 5 | Complete Heart Block | AV dissociation, slow escape rhythm |
| 6 | VT / VF | Wide QRS tachycardia / chaotic deflections |
| 7 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 8 | Long QT Syndrome | QTc >450/460 ms + torsades de pointes |
| 9 | Brugada Syndrome | Coved ST elevation in V1-V2 (Type 1) |
| 10 | Acute Pericarditis | Diffuse concave ST elevation + PR depression |
Sources: Braunwald's Heart Disease 2-Vol Set (Cardiovascular Medicine); Harrison's Principles of Internal Medicine 22E (2025); Tintinalli's Emergency Medicine, Comprehensive Study; Fuster and Hurst's The Heart, 15th Edition; Goldman-Cecil Medicine International Edition; Symptom to Diagnosis, 4th Edition; Ganong's Review of Medical Physiology, 26th Edition.
With ecg images
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have high-quality textbook ECG images for all 10 conditions. Here is the complete illustrated guide:
10 Heart Diseases with ECG Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural myocardial injury. Three simultaneous electrical defects produce ECG changes: rapid repolarization, decreased resting membrane potential, and delayed depolarization in infarcted cells - all producing ST elevation over the infarct zone.
ECG Features:
- Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in precordial leads
- Reciprocal ST depression in opposite leads
- Evolving pathological Q waves (necrosis marker)
- Hyperacute tall T waves in the very earliest phase
Lead Localization: Inferior (II, III, aVF) = RCA; Anterior (V1-V4) = LAD; Lateral (I, aVL, V5-V6) = LCx
2. NSTEMI / Unstable Angina
Pathophysiology: Partial occlusion causes subendocardial (not transmural) ischemia. The subendocardium is most vulnerable because it receives coronary blood flow last.
ECG Features:
- Horizontal or downsloping ST depression ≥0.5 mm in ≥2 contiguous leads
- Symmetric T-wave inversions - deep inversions in V2-V3 = Wellens syndrome (critical proximal LAD stenosis)
- No pathological Q waves
- ECG may be completely normal (does not exclude NSTEMI - diagnosis requires troponin)
The distinction from STEMI is critical: no localized ST elevation, no Q-wave development, and troponin elevation drives the diagnosis.
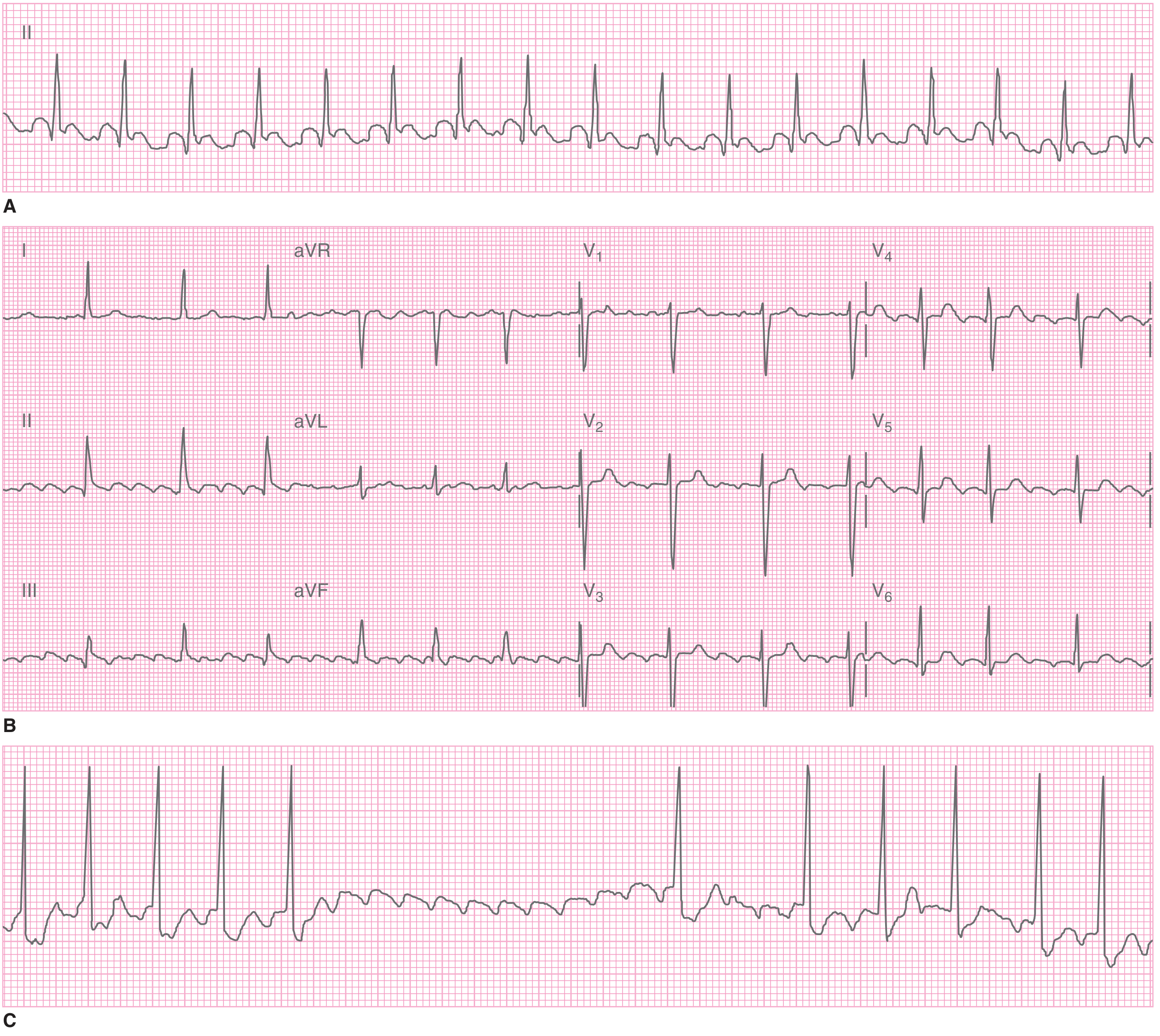
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized re-entrant wavelets in both atria fire at 350-600 bpm. The AV node filters most impulses but conducts irregularly, producing an irregularly irregular ventricular response.
ECG Features:
- Complete absence of P waves - replaced by irregular fibrillatory "f waves" (best seen in V1)
- Irregularly irregular RR intervals - the hallmark (no two consecutive RR intervals are equal)
- Narrow QRS unless aberrant conduction
- Ventricular rate typically 100-170 bpm if uncontrolled
4. Atrial Flutter
Pathophysiology: A single large macro-reentrant circuit rotates counterclockwise in the right atrium at ~300 bpm. The AV node cannot conduct all impulses and typically allows every 2nd impulse through (2:1 block).
ECG Features:
- Classic "sawtooth" flutter waves (F waves) at 250-350 bpm, most visible in leads II, III, aVF and V1
- Regular or fixed-ratio ventricular response (2:1 = rate ~150 bpm; 3:1 = ~100 bpm; 4:1 = ~75 bpm)
- Narrow QRS (unless aberrant conduction)
- Rate of exactly 150 bpm should always raise suspicion for flutter with 2:1 block
5. Complete (Third-Degree) Heart Block
Pathophysiology: Total failure of AV conduction - no sinus impulses reach the ventricles. The atria and ventricles beat completely independently. A subsidiary escape pacemaker (junctional or ventricular) maintains ventricular activity at a slow rate.
ECG Features:
- P waves present, regular, at normal sinus rate (60-100 bpm)
- QRS complexes present but at a slow, independent escape rate
- No fixed PR interval - P waves "march through" QRS complexes without any relationship
- Junctional escape: narrow QRS at 40-60 bpm (more stable)
- Ventricular escape: wide, bizarre QRS at <40 bpm (less stable, worse prognosis)
- Ventricular rate is regular but slower than atrial rate

6. Ventricular Tachycardia (VT) and Ventricular Fibrillation (VF)
Pathophysiology: VT - rapid ectopic rhythm originating below the bundle of His; most commonly from post-MI scar reentry. VF - completely chaotic ventricular electrical activity with no coordinated contraction; causes cardiac arrest.
VT ECG Features:
- Wide QRS (≥120 ms) tachycardia at rate >100 bpm (usually 140-220 bpm)
- Monomorphic VT: consistent QRS morphology beat to beat; regular rhythm
- Polymorphic VT: varying QRS morphology and axis
- AV dissociation: P waves at different (slower) rate unrelated to QRS - most specific sign
- Fusion beats and capture beats: pathognomonic when present
VF ECG Features:
- Completely chaotic, irregular deflections - no organized P waves, QRS, or T waves
- Coarse VF: large amplitude (early); Fine VF: small amplitude (late, worse prognosis)
7. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, conducting impulses directly from atria to ventricles. This causes ventricular pre-excitation - the ventricle starts depolarizing before normal His-Purkinje conduction arrives, creating the delta wave.
ECG Features (the WPW triad in sinus rhythm):
| Feature | Finding | Mechanism |
|---|---|---|
| Short PR | < 120 ms | Bypass tract conducts faster than AV node |
| Delta wave | Slurred initial QRS upstroke | Slow cell-to-cell conduction from AP insertion |
| Wide QRS | ≥ 120 ms | Delta wave adds to QRS duration |
- Secondary ST-T changes discordant to delta wave direction
- Pseudo-Q-waves (delta waves mimicking infarction) can cause false-positive MI diagnosis
- AF with WPW: extremely rapid (>200 bpm), bizarre, wide, irregular tachycardia - life-threatening; avoid AV nodal agents
8. Long QT Syndrome (LQTS)
Pathophysiology: Prolonged ventricular repolarization - either congenital (channelopathy affecting K⁺ or Na⁺ channels) or acquired (drugs, electrolytes). Prolongs the window of vulnerability to early afterdepolarizations, triggering torsades de pointes (TdP).
ECG Features:
- Prolonged QTc - males >450 ms, females >460 ms (high risk for TdP when >500 ms)
- Torsades de pointes: Polymorphic VT where QRS complexes appear to "twist" around the isoelectric line ("twisting of the points") at 200-250 bpm
- T-wave morphology by subtype: LQT1 = broad-based T wave; LQT2 = notched/biphasic T wave; LQT3 = late T wave after long isoelectric ST
- Prominent U waves
- Torsades often self-terminates but can degenerate to VF
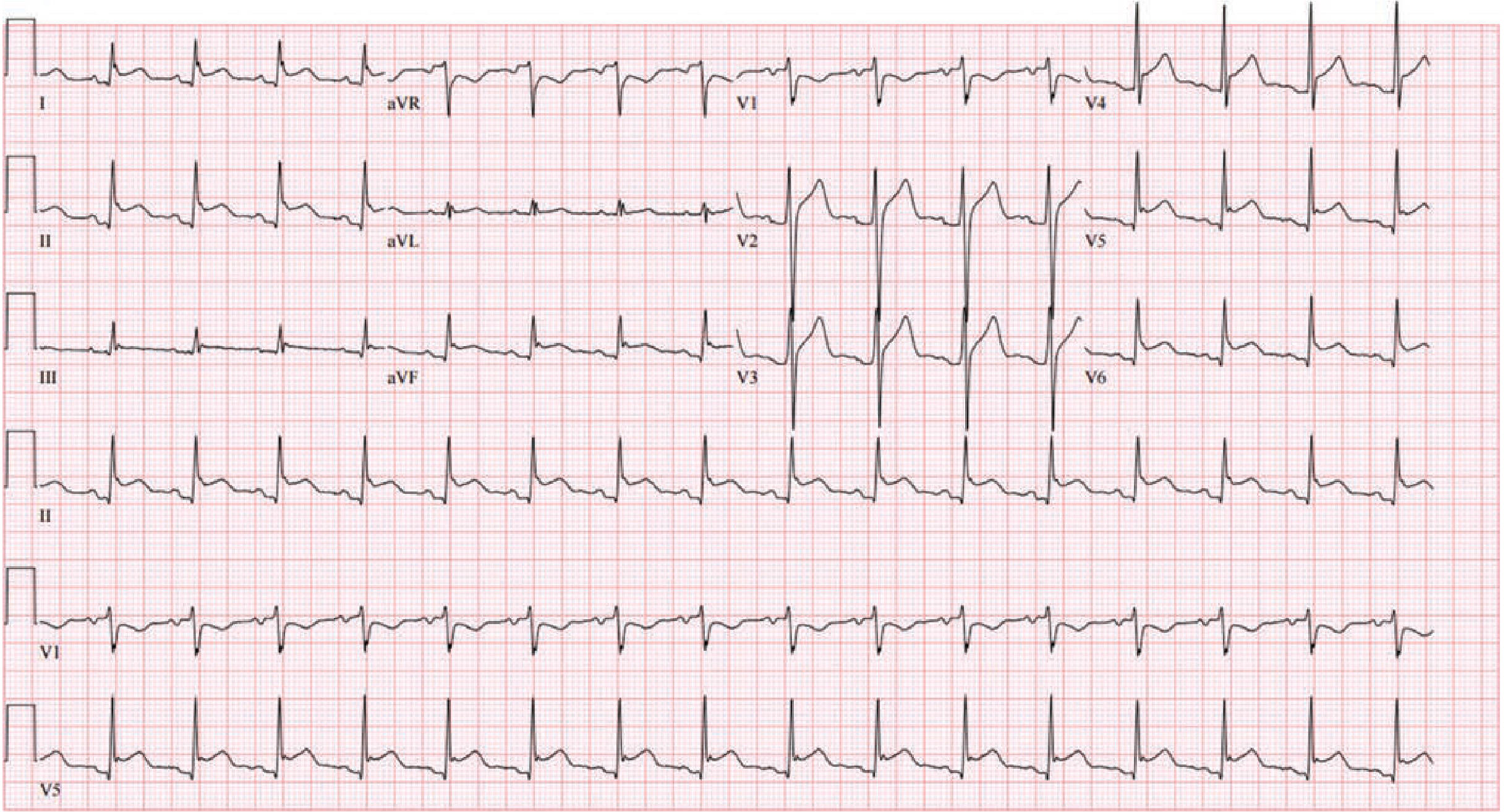
9. Brugada Syndrome
Pathophysiology: Sodium channelopathy (SCN5A mutation in ~20% of cases) causing loss of the action potential dome in right ventricular epicardium. This creates a voltage gradient between endocardium and epicardium that manifests as ST elevation in right precordial leads and predisposes to VF.
ECG Features:
- Type 1 (diagnostic - "coved" pattern): ≥2 mm coved ST elevation with negative T wave in V1-V2, often with RBBB-like morphology - the ONLY pattern that is diagnostic
- Type 2 ("saddle-back"): ≥2 mm saddle-back ST elevation - not diagnostic alone but can convert to Type 1 with sodium-channel blocker challenge (ajmaline/flecainide)
- Pattern can be intermittent - fever, vagal tone, and certain drugs unmask it
- Predominantly affects young Asian males; often manifests during sleep
10. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium spreads to the adjacent epicardium (epicardial myocarditis), causing widespread subepicardial injury that produces diffuse ECG changes. The inflamed pericardium also involves the atria, causing PR depression.
ECG Features - Classic 4 Stages:
| Stage | PR Segment | ST Segment | T Wave |
|---|---|---|---|
| Stage 1 (acute, days 1-2) | Depressed (especially II, aVF, V4-V6) | Diffuse elevation (concave/saddle-shaped) in I, II, aVF, V2-V6; aVR shows ST depression | Upright, tall |
| Stage 2 (days 3-7) | Isoelectric or still depressed | Returns to baseline | Amplitude decreases |
| Stage 3 (weeks 1-3) | Isoelectric | Isoelectric | Diffuse T-wave inversions |
| Stage 4 (weeks-months) | Normal | Normal | Normal |
Key distinguishing features from STEMI:
- ST elevation is diffuse (all leads except aVR/V1) and concave upward ("saddle-shaped") - not localized
- PR segment depression (atrial injury) - present in most leads; PR elevation in aVR
- No reciprocal ST depression (unlike STEMI)
- No pathological Q waves
- ST:T amplitude ratio >0.25 in V6 or lead I favors pericarditis over early repolarization
Quick Reference Summary
| # | Condition | Hallmark ECG Feature |
|---|---|---|
| 1 | STEMI | Localized convex ST elevation, evolving Q waves, reciprocal depression |
| 2 | NSTEMI/UA | ST depression ± T-wave inversions; no Q waves |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular RR intervals |
| 4 | Atrial Flutter | Sawtooth F waves ~300 bpm, fixed AV ratio (2:1 = 150 bpm) |
| 5 | Complete Heart Block | AV dissociation; slow independent escape rhythm |
| 6 | VT / VF | Wide-complex tachycardia / chaotic deflections |
| 7 | WPW Syndrome | Short PR + delta wave + widened QRS |
| 8 | Long QT Syndrome | QTc >450/460 ms; torsades de pointes |
| 9 | Brugada Syndrome | Type 1 coved ST elevation in V1-V2 |
| 10 | Acute Pericarditis | Diffuse concave ST elevation + PR depression (all leads except aVR) |
Sources: Tintinalli's Emergency Medicine (Comprehensive Study); Fuster & Hurst's The Heart, 15th Ed; Goldman-Cecil Medicine International Edition; Ganong's Review of Medical Physiology, 26th Ed; Washington Manual of Medical Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.