Epidymeal cyat treay
Reading File
Finding Sources
Searching PubMed
epididymal cyst spermatocele treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of epididymal cyst treatment, based on authoritative urology and surgical textbooks.
Epididymal Cyst - Overview and Treatment
What is it?
An epididymal cyst is a benign, fluid-filled cyst arising from cystic degeneration of the epididymal tubules. The fluid is clear (unlike a spermatocele, which contains spermatozoa and looks like barley water). They are:
- Very common - found in ~31% of men aged 20-39 and up to 43% of asymptomatic men aged 40-59
- Usually multiple and vary in size
- Often bilateral, most common in middle age
- Feel like tiny bunches of grapes posterior to and separate from the testis
- They transilluminate on examination
Spermatocele is a closely related entity - a unilocular retention cyst containing sperm, typically at the epididymal head above the upper pole of the testis.
Ultrasound Appearance
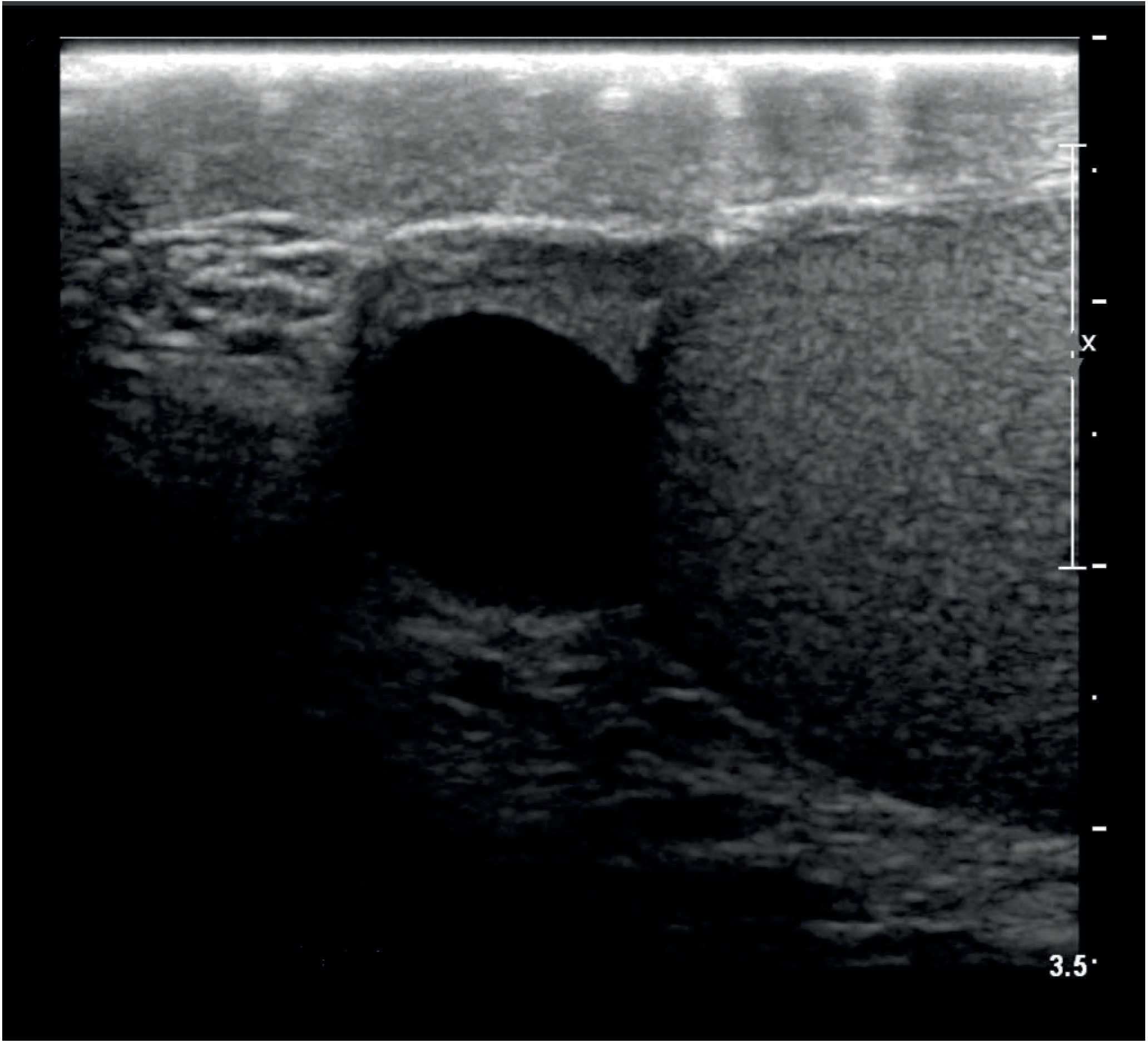
Treatment
1. Conservative (Watch and Wait) - First Line
- Most epididymal cysts are asymptomatic and require no treatment
- Treatment is only indicated for: discomfort, infection, disability due to size, or infertility concerns
- Diagnosis should be confirmed by ultrasound to rule out intratesticular pathology
2. Aspiration - Generally Avoided
- Aspiration alone is ineffective because epididymal cysts are usually multilocular - fluid reaccumulates
- Not recommended as a standalone treatment
3. Surgical Excision (Spermatocelectomy / Epididymal Cyst Excision)
- Indicated when cysts are large, symptomatic, or causing significant discomfort
- Approach: Trans-scrotal incision, dissection to the tunica vaginalis, opening the tunica, exposing the cyst, dissecting it down to its stalk, and ligating it with absorbable suture
- Single large cysts can be excised individually
- Recurrent or multilocular cysts often require partial or total epididymectomy
4. Special Considerations - Fertility Counselling (Very Important)
- Men of reproductive age must be counselled about the risk of obstructive azoospermia following surgery
- Risk is highest when the cyst is in the corpus or cauda of the epididymis
- Excision is expected to interfere with sperm transport from the testis on that side
Summary
| Situation | Management |
|---|---|
| Small, asymptomatic | Conservative - observation |
| Aspiration | Not recommended (multilocular, recurs) |
| Symptomatic / large | Surgical excision via scrotal approach |
| Multilocular / recurrent | Partial or total epididymectomy |
| Young man wanting fertility | Counsel about azoospermia risk before operating |
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1588; Campbell-Walsh-Wein Urology, p. 2464
Rate of recuurence in opena and endovacuslar varicose vein sugery
Reading File
Finding Sources
Searching PubMed
varicose vein recurrence open surgery endovenous ablation
Reading File
Reading Article
Reading File
Finding Sources
Reading File
Reading File
Excellent data gathered. Here is a thorough, evidence-based answer.
Recurrence Rates: Open vs. Endovascular Varicose Vein Surgery
Defining Recurrence
Recurrence rates vary considerably in the literature because definitions differ. "Recurrence" can mean:
- Clinical recurrence - visible, symptomatic varicose veins returning
- Duplex-detected recurrence - reflux or varicosities seen on ultrasound even without symptoms
- PREVAIT (Presence of Varices After Interventional Treatment) - a more standardised modern definition
This heterogeneity makes direct comparisons across studies challenging.
Open Surgery (High Ligation + Stripping - HLS)
| Timeframe | Recurrence Rate |
|---|---|
| 5-10 years (significant clinical recurrence) | 10-35% |
| Duplex-detected (minor/subclinical) | Up to 70% |
| Mean PREVAIT across studies (18 months to 5 years) | ~34.4% |
- Recurrence is more common after short saphenous vein (SSV) surgery than great saphenous vein (GSV) surgery
- Higher BMI increases recurrence risk
- Stripping of the incompetent axial vein reduces recurrence compared to ligation alone
Causes of recurrence after open surgery:
- Neovascularisation - most common mechanism (new valveless veins bridging the ligated junction to tributaries); range 29.8-91% of recurrences
- Residual/refluxing axial vein
- Inadequate initial surgery (missed junctions)
- New junctional reflux
Endovascular Methods
Endovenous Laser Ablation (EVLA)
- Mean PREVAIT rate: ~16.6% (follow-up 112 days to 5 years)
- Most common recurrence mechanism: development of new varicose veins (40-81.6% of cases)
- Re-intervention rates after recurrence: 0-57% across studies
Radiofrequency Ablation (RFA)
- Lowest reported PREVAIT rate: ~6.7% (follow-up 106 days to 5 years)
- Dominant recurrence mechanism is different: recanalization of the occluded saphenous trunk (accounts for up to 67% of RFA recurrences, vs. neovascularisation for HLS/EVLA)
- Re-intervention rate in one study: 6.67%
Head-to-Head Comparison Summary
| Technique | PREVAIT / Recurrence Rate | Primary Recurrence Mechanism |
|---|---|---|
| Open (HLS) | ~34.4% | Neovascularisation (29-91%) |
| EVLA | ~16.6% | New varicose veins (40-82%) |
| RFA | ~6.7% | Recanalization (up to 67%) |
Key point from Schwartz's Surgery: "Endovenous laser treatment and RFA result in durable ablation of the GSV, with rates of varicose vein recurrence and clinical severity scores comparable to those seen with open surgery" - though a 2023 systematic review found HLS had the highest recurrence numerically.
Recurrence After Re-do Open Surgery
Open surgery for recurrent varicose veins (after any prior treatment) carries a high complication rate of approximately 40%, most commonly lymph leak and wound infection. This has made endovenous techniques the preferred approach for recurrent disease where anatomically feasible.
Causes of Recurrence (All Techniques)
- Neovascularisation at the groin junction
- Recanalization of the treated vein (especially RFA)
- Progression of disease in untreated segments
- New tributary incompetence
- Inadequate initial treatment
Sources:
- [Bailey & Love's Short Practice of Surgery, 28th Ed.](p. 1060) - clinical and duplex recurrence figures, causes
- Schwartz's Principles of Surgery, 11th Ed., p. 2455
- Mulholland & Greenfield's Surgery, 7th Ed., p. 5234-5235
- Miranda et al., 2023 (PMID 37795801) - Systematic review of PREVAIT after HLS, EVLA and RFA across 14 studies, 2795 patients
Herinotomy age limit and h hirontomy done
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Excellent content gathered. Here is the complete answer.
Herniotomy vs Herniorrhaphy - Age, Indications & How They Are Done
The Core Distinction
| Procedure | What it means | When used |
|---|---|---|
| Herniotomy | Excision/ligation of the hernial sac only - no floor repair | Children (and occasionally adults with small indirect hernias) |
| Herniorrhaphy / Hernioplasty | Herniotomy + reconstruction of the inguinal floor (with sutures or mesh) | Adults and adolescents with floor weakness |
Herniotomy - Age Limit & Rationale
Used in: Children - because in a child the hernia is an indirect hernia caused purely by a patent processus vaginalis (a congenital defect). The inguinal floor is otherwise completely normal. Once the sac is removed/ligated, the deep ring closes naturally - no floor repair is needed.
Age limit: There is no absolute cut-off number, but the principle is:
- Children up to puberty - herniotomy (high ligation) is the standard
- Post-pubertal males - anatomy resembles adults (larger inguinal ring, possible transverse fascia defects), so floor reconstruction may be needed
- Textbooks acknowledge: "It is unclear as to which age/size a child becomes an adult with respect to principles of hernia repair" - individualized assessment is required for adolescents, especially those with weak inguinal floors or direct hernias
Key rule: Herniotomy alone is rarely used in adults - it would not address the floor weakness that exists in adult hernias.
How Herniotomy is Done (Steps)
- Incision - transverse skin crease incision over the inguinal canal, starting at the pubic tubercle extending laterally
- Expose external oblique - incise Scarpa's fascia, clear fat, expose external oblique aponeurosis
- Open external oblique - incise in line of its fibres through the external ring; free the lower leaf from the spermatic cord
- Isolate the cord - lift spermatic cord, pass a Penrose drain around it for retraction
- Open cremaster - separate cremasteric fibres to expose the hernia sac (which lies anteromedial to cord structures); ilioinguinal and iliohypogastric nerves are preserved
- Dissect the sac - carefully dissect the sac free from the vas deferens and testicular vessels
- High ligation - the sac is dissected to its neck at the internal ring (proximally), twisted to reduce any contents, and transfixed + ligated at the internal ring (this is the "high ligation")
- Divide and excise - the sac is divided distal to the ligature and excess sac removed
- Optional: the sac can be opened before ligation to allow digital examination of the abdominal cavity and femoral ring
- Alternative: the sac may simply be inverted (not opened) - less pain as the highly innervated peritoneum is not violated
- Close in layers - external oblique, Scarpa's fascia, skin
For laparoscopic herniotomy in children: an encircling purse-string suture is placed laparoscopically at the internal ring to obliterate the processus vaginalis.
How Herniorrhaphy Differs (Adults)
In adults the inguinal floor is weak, so after dealing with the sac (same as herniotomy), a floor repair is added:
- Tissue repairs (Bassini, Shouldice) - native tissues are used to reinforce the posterior wall of the inguinal canal
- Tension-free mesh repair (Lichtenstein) - a flat mesh is sutured to the inguinal floor; this is the gold standard in adults, with recurrence rates <2%
- Preperitoneal repairs (open or laparoscopic - TEP, TAPP) - mesh placed in the preperitoneal space to cover all groin hernia defects
For large indirect inguinoscrotal hernias in adults: complete sac removal risks cord/testicular complications, so the sac is transected at the midpoint of the canal and the distal sac left in situ.
Summary
Child (indirect hernia, normal floor)
→ HERNIOTOMY = high ligation of sac only
Adult / post-pubertal (floor weakness ± indirect/direct)
→ HERNIORRHAPHY = herniotomy + floor reconstruction (mesh or tissue)
Sources: Mulholland & Greenfield's Surgery, 7th Ed., pp. 3686-3687; Bailey & Love's Short Practice of Surgery, 28th Ed., p. 278
This is a shared conversation. Sign in to Orris to start your own chat.