Notes on male and female infertility that also include points 1.Order and interpret relevant investigations of Sexual dysfunction and Infertility 2. Describe differential diagnosis of Sexual dysfunction and Infertility
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed to compile comprehensive notes. Here are the full study notes:
Male and Female Infertility - Comprehensive Notes
PART 1: DEFINITIONS AND EPIDEMIOLOGY
- Infertility = failure to achieve pregnancy after 1 year of unprotected intercourse
- 15-20% of all couples are affected
- Causes are distributed roughly:
- 1/3 male factors alone
- 1/3 female factors alone
- 1/3 combination of both
- ~20% unexplained (idiopathic)
- Female fertility peaks at ages 20-24, declines progressively after 32, steep decline after 40
- In female couples desiring conception, donor sperm is needed - they are not "infertile" in the traditional sense
Workup should begin after 6 months (not 1 year) if the woman is over 35, has irregular menses, known history of pelvic inflammatory disease (PID), STI, or exposure to gonadotoxic agents.
PART 2: MALE INFERTILITY
Causes / Differential Diagnosis
| Diagnostic Category | Incidence (%) |
|---|---|
| Idiopathic infertility | 50-60 |
| Varicocele (most common identifiable cause) | 15-35 |
| Primary testicular failure (Klinefelter syndrome, Y chromosome microdeletions, cryptorchidism, irradiation, orchitis, drugs) | 10-20 |
| Genital tract obstruction (congenital absence of vas, vasectomy, epididymal obstruction) | 5 |
| Hypogonadotropic hypogonadism (pituitary adenomas, panhypopituitarism, hyperprolactinemia) | 3-4 |
| Other (sperm autoimmunity, drugs, toxins, systemic illness) | 5 |
| Coital disorders | <1 |
Full Differential Diagnosis - Male Infertility Factors:
Endocrine Disorders:
- Hypothalamic dysfunction (Kallmann syndrome)
- Pituitary failure (tumor, radiation, surgery)
- Hyperprolactinemia (drug-induced, tumor)
- Androgen insensitivity syndrome (AIS)
- Exogenous androgens (anabolic steroids)
- Thyroid disorders
- Adrenal hyperplasia
- Testicular failure
Anatomic:
- Congenital absence of vas deferens (associated with CFTR mutations)
- Obstructed vas deferens
- Congenital abnormalities of ejaculatory system
- Varicocele
- Retrograde ejaculation
Abnormal Spermatogenesis:
- Unexplained azoospermia
- Chromosomal abnormalities (e.g., Klinefelter 47,XXY)
- Mumps orchitis
- Cryptorchidism
- Chemical or radiation exposure
Abnormal Motility:
- Absent cilia - Kartagener syndrome (Primary Ciliary Dyskinesia)
- Antisperm antibody formation
Psychosocial:
- Unexplained impotence
- Decreased libido
Investigations for Male Infertility
Step 1: History & Physical Examination
- Reproductive history, STD history, contraception
- Medications (especially anabolic steroids, chemotherapy, antihypertensives)
- Recreational drug, alcohol, and environmental toxin exposure
- Sexual history: erectile function, ejaculatory technique, lubricant use
- Surgical history (vasectomy, hernia repair, pelvic surgery)
- Family history of genetic diseases
- Physical: external genitalia for androgenization, hair pattern (virilization), gynecomastia, neurologic findings (anosmia, visual impairment), testicular atrophy
Step 2: Semen Analysis (First-Line Test)
- Most important laboratory test in male fertility evaluation
- Semen analyzed within 1 hour of collection
- Two consecutive abnormal results required before proceeding to further workup
Normal Seminal Fluid Values (WHO Reference):
| Parameter | Normal Value |
|---|---|
| Ejaculate volume | >1.5 mL |
| Sperm density | >15 million/mL |
| Total sperm count | >39 million/ejaculate |
| Motility | >32% progressive; >40% total |
| Morphology | >4% normal (Kruger strict criteria) |
| pH | 7.2-8.0 |
| Liquefaction | Within 40 minutes |
| Fructose | >1200 µg/mL |
| Zinc | >75 µg/mL |
Sperm abnormalities terminology:
- Azoospermia = no sperm in ejaculate
- Oligospermia = low sperm count (<15 million/mL)
- Asthenospermia = reduced motility
- Teratospermia = abnormal morphology
Step 3: Endocrine Evaluation (if semen analysis abnormal x2)
- Testosterone (total) - assess Leydig cell function
- LH - distinguishes primary vs. secondary hypogonadism
- FSH - marker of spermatogenesis integrity (elevated = testicular failure)
- Prolactin - rule out hyperprolactinemia
- TSH - rule out thyroid disease
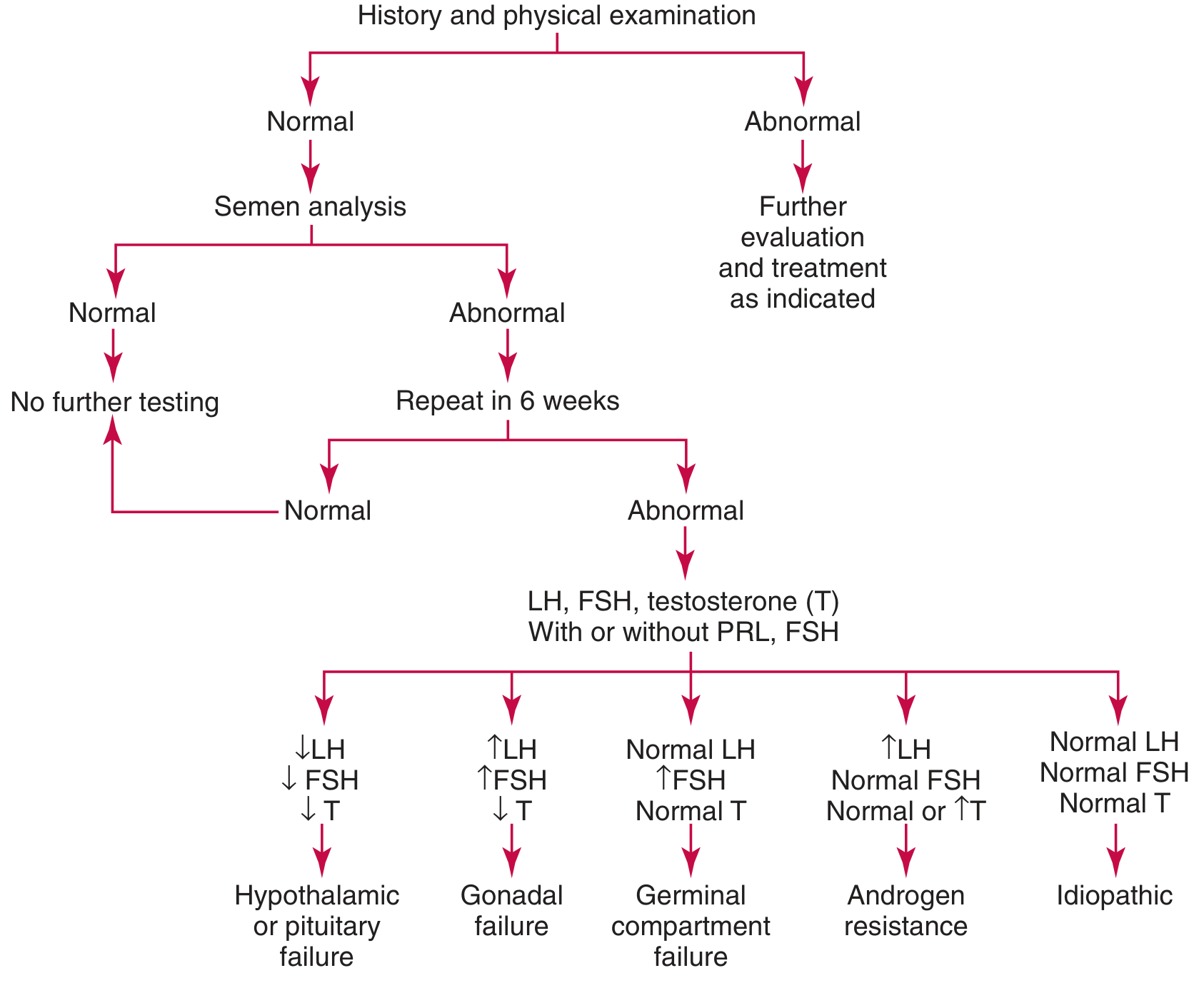
Hormonal Pattern Interpretation:
| Pattern | Diagnosis |
|---|---|
| ↓LH, ↓FSH, ↓Testosterone | Hypothalamic or pituitary failure (hypogonadotropic hypogonadism) |
| ↑LH, ↑FSH, ↓Testosterone | Gonadal (primary testicular) failure |
| Normal LH, ↑FSH, Normal T | Germinal compartment failure (Sertoli cell only) |
| ↑LH, Normal FSH, Normal or ↑T | Androgen resistance |
| All normal | Idiopathic |
Algorithm for Evaluating Male Infertility:
Step 4: Additional Investigations (as indicated)
- Karyotype / Chromosomal analysis - rule out Klinefelter (47,XXY), Y chromosome microdeletions
- CFTR mutation testing - if bilateral congenital absence of vas deferens
- Testicular biopsy - differentiate obstructive from non-obstructive azoospermia
- Scrotal Doppler ultrasound - confirm varicocele
- Post-ejaculate urinalysis - rule out retrograde ejaculation
- Anti-sperm antibodies - immunologic cause
- Transrectal ultrasound (TRUS) - evaluate ejaculatory ducts
- MRI pituitary - if hyperprolactinemia confirmed
Management of Male Infertility
- Treat underlying infection with appropriate antibiotics
- Varicocelectomy for varicocele
- Counseling about environmental factors (avoid heat, toxins)
- IUI (Intrauterine Insemination) for mild male factor
- ICSI (Intracytoplasmic Sperm Injection) for severe male factor - outcomes comparable to conventional IVF
- Referral to infertility specialist
PART 3: FEMALE INFERTILITY
Causes / Differential Diagnosis
Female Infertility Factors:
Ovarian/Hormonal Factors (40% of female infertility):
- Polycystic Ovarian Syndrome (PCOS) - most common cause of anovulation
- Primary Ovarian Insufficiency (POI) / premature menopause
- Hypergonadotropic hypogonadism (gonadal dysgenesis, resistant ovary syndrome)
- Hypogonadotropic hypogonadism (Kallmann syndrome, pituitary/hypothalamic insufficiency)
- Hyperprolactinemia (tumor, drugs)
- Luteal phase deficiency
- Thyroid disorders (hypothyroidism, hyperthyroidism)
- Liver disease, obesity, androgen excess
- Anorexia, excessive exercise, stress
Tubal Factors (20-40%):
- Tubal occlusion or scarring from PID
- Salpingitis isthmica nodosa
- Infectious salpingitis (Chlamydia, Gonorrhea)
- Previous ectopic pregnancy
- Post-surgical adhesions
Uterine Factors (up to 15%):
- Leiomyomata (fibroids, esp. submucosal)
- Congenital malformation (Mullerian anomalies)
- Intrauterine adhesions (Asherman syndrome)
- Endometritis / abnormal endometrium
Cervical Factors (<5%):
- Cervical stenosis
- Inflammation or infection
- Abnormal mucous viscosity
Peritoneal/Pelvic Factors:
- Endometriosis (30-40% when combined with tubal)
- Pelvic adhesions
Immunologic:
- Antisperm antibodies
Psychosocial:
- Decreased libido, anorgasmia
Unexplained (~20%)
Investigations for Female Infertility
Step 1: History & Physical Examination
- Menstrual history: regularity, cycle length, dysmenorrhea
- Obstetric history: prior pregnancies, miscarriages
- History of PID, STIs, pelvic surgery
- Medications and gonadotoxin exposure
- Physical: external genitalia for androgen excess (clitoromegaly, hirsutism), thyroid exam, galactorrhea, uterine and adnexal pathology
Step 2: Confirm Ovulation
- Urinary LH ovulation predictor kits (detect LH surge) - recommended
- Mid-luteal serum progesterone (7 days before anticipated menses) - value >3 ng/mL indicates ovulation; >10 ng/mL = adequate luteal phase
- Transvaginal ultrasound - follicular tracking
- Note: Basal body temperature (BBT) is no longer routinely recommended
Step 3: Ovarian Reserve Assessment
- Serum FSH on Day 3 of menstrual cycle - value >12 IU/L = poor ovarian reserve
- Serum Estradiol (E2) on Day 3 - elevated E2 with normal FSH can still suggest poor reserve
- Anti-Mullerian Hormone (AMH) - best single marker of ovarian reserve; not cycle-dependent
- Antral Follicle Count (AFC) on transvaginal ultrasound
- Women >35 should always have ovarian reserve testing
Step 4: Ovarian/Hormonal Investigations
| Factor | Tests |
|---|---|
| Ovulatory factors | Urinary LH kit; serum progesterone (luteal phase); transvaginal US; TSH, FSH, LH, prolactin, androgens |
| Cervical factors | Cervical mucus evaluation; postcoital test |
| Uterine factors | Ultrasonography, hysterosalpingography (HSG), hysteroscopy, sonohysterography, MRI |
| Tubal factors | Hysterosalpingography (HSG); laparoscopy with chromotubation; fluoroscopic or hysteroscopic tubal cannulation |
| Peritoneal factors | Ultrasonography, diagnostic laparoscopy |
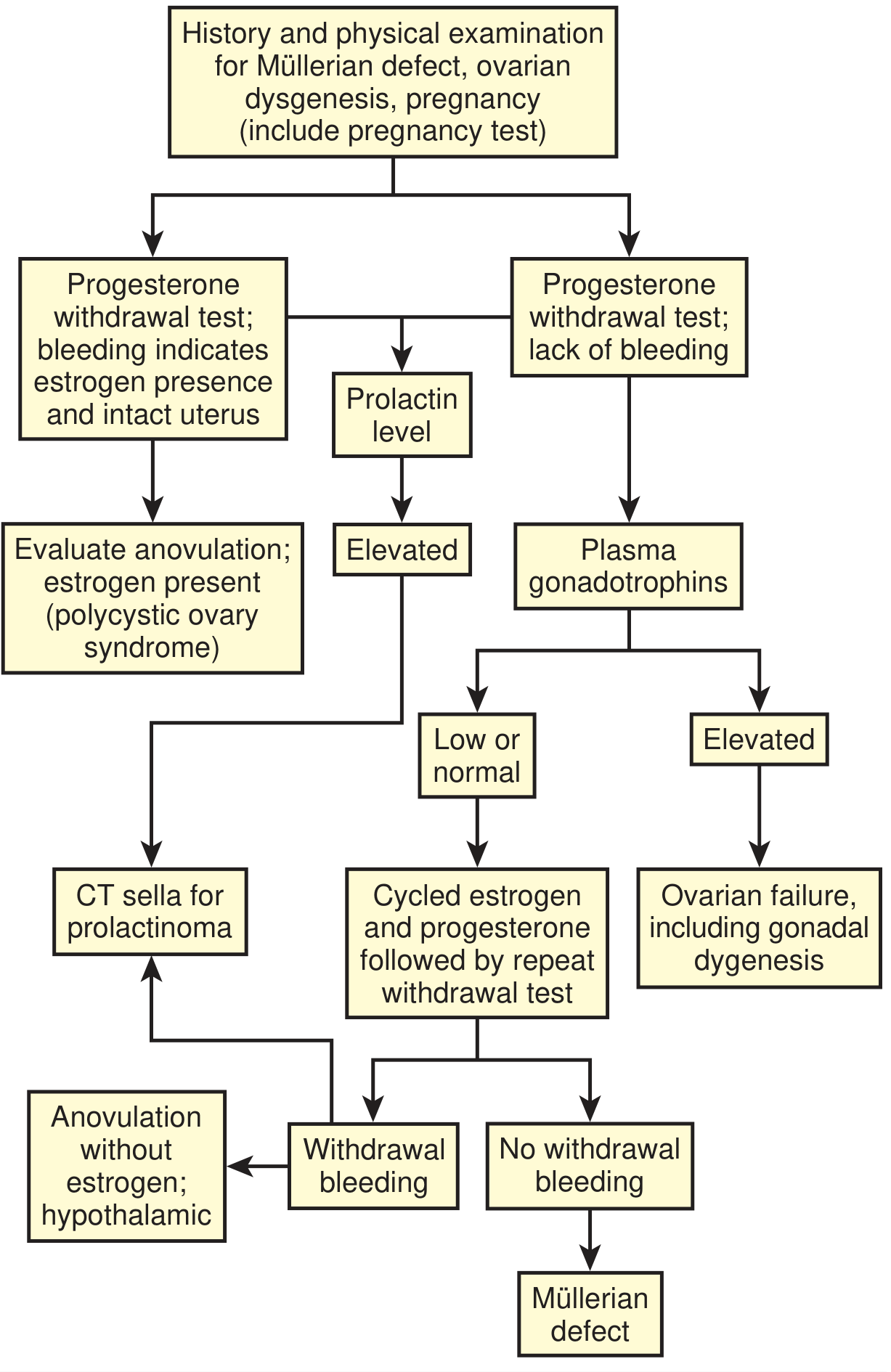
Diagnostic Algorithm for Female (Amenorrhea/Ovulatory Dysfunction):
Step 5: Additional Investigations
- Serum AMH - most reliable ovarian reserve marker
- 17-OH Progesterone - elevated in follicular phase suggests congenital adrenal hyperplasia (CAH)
- Androgens (total testosterone, DHEA-S) - if androgen excess suspected
- Karyotype - if primary ovarian insufficiency (Turner syndrome 45,X)
- MRI pituitary - if hyperprolactinemia confirmed
- Pelvic/transvaginal ultrasound - ovarian morphology (PCOS), fibroids, polyps
- HSG (Hysterosalpingography) - tubal patency, uterine cavity
- Diagnostic laparoscopy - gold standard for endometriosis and pelvic adhesions
- Hysteroscopy - direct visualization of uterine cavity
Hypogonadotropic Hypogonadism in Females (Laboratory Pattern):
- Serum E2 <40 pg/mL
- LH <10 IU/L, FSH <10 IU/L
- No withdrawal bleeding on progestin challenge (thin endometrium)
- Causes: pituitary/hypothalamic failure, hyperprolactinemia, Kallmann syndrome
Hypergonadotropic Hypogonadism in Females:
- Elevated FSH and LH, low E2
- Causes: POI, gonadal dysgenesis, menopause, resistant ovary syndrome
PART 4: SEXUAL DYSFUNCTION
Definition & DSM-5 Framework
- Sexual dysfunction = persistent problem causing clinically significant distress
- Subtypes:
- Lifelong (since sexual debut) vs. Acquired (after period of normal function)
- Generalized (all situations) vs. Situational (specific contexts/partners)
- Severity: mild / moderate / severe
Factors to assess before diagnosing sexual dysfunction:
- Partner factors (partner's response, partner's involvement)
- Relationship factors (communication, emotional abuse)
- Individual vulnerability (body image, psychiatric comorbidity - depression, anxiety; life stressors)
- Cultural/religious factors
- Medical factors (physical disability, medications)
Female Sexual Dysfunction
A. Female Sexual Interest/Arousal Disorder (FSIAD)
- Most common female sexual problem - affects 4 in 10 women
- Diagnosed when lacking/reduced sexual interest for ≥6 months, with at least 3 of 6 criteria:
- Absent/reduced interest in sexual activity
- Absent/reduced sexual/erotic thoughts or fantasies
- No/reduced initiation; unreceptive to partner's initiation
- Absent/reduced sexual excitement/pleasure during activity
- Absent/reduced sexual interest in response to any erotic cues
- Absent/reduced genital/nongenital sensations during activity
B. Female Orgasmic Disorder
- Delay, infrequency, or absence of orgasm; reduced intensity
- SSRIs delay/inhibit orgasm in women
C. Genito-Pelvic Pain/Penetration Disorder
- Prevalence: 12-21% in the United States
- Persistent difficulty with penetration, pelvic/vaginal pain, fear/anxiety, pelvic floor tightening
- History: pain on tampon insertion before sexual activity is an important risk factor
- Exam: visible pelvic floor muscle contraction, anatomical abnormalities
D. Differential Diagnosis of Female Sexual Dysfunction
- Depression, anxiety disorders
- Relationship conflict
- History of sexual trauma/abuse (PTSD)
- Endocrine: hypothyroidism, hyperprolactinemia, menopause (low estrogen)
- Pelvic pathology: vulvodynia, vestibulodynia, endometriosis, vaginismus
- Neurological disease
- Medication-induced (SSRIs, antipsychotics, OCPs)
- Substance use (alcohol, opioids)
Male Sexual Dysfunction
A. Erectile Dysfunction (ED)
Definition: Inability to achieve or maintain an erect penis sufficient for satisfactory sexual activity
Pathophysiology:
- Parasympathetic stimulation → nitric oxide (NO) release → increases intracellular cGMP → cavernosal smooth muscle relaxation → rapid blood inflow → occlusion of emissary veins → erection
- PDE-5 degrades cGMP; PDE-5 inhibitors prolong erection
- Requires intact vascular, neurologic, endocrine, and psychological systems
Prevalence increases with age:
- 2% at ages 40-49
- 6% at ages 50-59
- 17% at 60+ years
B. Differential Diagnosis of ED
| Category | Examples |
|---|---|
| Vascular | Atherosclerosis, HTN, dyslipidemia, diabetes, smoking, obesity, peripheral vascular disease |
| Neurogenic | Diabetes (autonomic neuropathy), MS, Parkinson's, spinal cord injury, radical prostatectomy |
| Endocrine | Hypogonadism (low testosterone), hyperprolactinemia, hypothyroidism, Cushing syndrome |
| Psychogenic | Performance anxiety, depression, relationship conflict, stress |
| Drug-induced | See table below |
| Anatomic | Peyronie's disease (fibrous plaques of corpus cavernosum) |
"What is bad for the heart is bad for the penis" - vascular risk factors are the most common modifiable cause
C. Premature (Early) Ejaculation (PE)
- Defined as intravaginal ejaculatory latency of <1 minute
- Most common male sexual complaint
D. Differential Diagnosis of Male Sexual Dysfunction
Organic causes:
- Vascular disease (commonest)
- Diabetes mellitus
- Hypogonadism / low testosterone
- Hyperprolactinemia
- Neurological disorders
- Peyronie's disease
- Post-surgical (radical prostatectomy, pelvic surgery)
- Medications (see below)
Psychological causes:
- Anxiety, depression
- Performance anxiety
- Relationship problems
- Post-traumatic stress
Investigations for Sexual Dysfunction
Male Sexual Dysfunction Workup
History:
- Nature of ED (complete vs. partial, situational vs. generalized, morning erections present?)
- Cardiovascular risk factors (DM, HTN, dyslipidemia, smoking)
- Medications and substance use
- Psychiatric symptoms (depression, anxiety)
- Relationship/partner issues
Physical Examination:
- Peripheral pulses (carotid auscultation for bruits)
- Thyroid exam
- Genitourinary: penile shaft (Peyronie plaques), testicular size/atrophy
- Neurological: anal sphincter tone, perianal sensation, bulbocavernosus reflex
- Secondary sexual characteristics assessment
Laboratory Investigations:
- Fasting glucose / HbA1c - rule out diabetes
- Fasting lipid profile - vascular risk
- Total testosterone (morning sample) - hypogonadism
- LH and FSH - if testosterone low (distinguish primary vs. secondary)
- Prolactin - if hypogonadism or visual symptoms
- TSH - thyroid disease
- BUN and creatinine - renal disease
- Serum transaminases - hepatic disease
- PSA - before testosterone therapy
Specialized Investigations (as needed):
- Nocturnal penile tumescence (NPT) testing - differentiates psychogenic from organic ED (erections during sleep preserved in psychogenic ED)
- Penile Doppler ultrasound with intracavernous injection - assesses arterial flow and venous leak
- Pudendal nerve conduction studies - neurogenic ED
- Pituitary MRI - if hyperprolactinemia confirmed
Female Sexual Dysfunction Workup
History:
- Onset, context, and duration of symptoms
- Relationship and partner factors
- Prior sexual trauma or abuse
- Psychiatric history (depression, anxiety)
- Medications (especially SSRIs, antipsychotics, OCPs, anticonvulsants)
- Menopausal status and hormonal symptoms
- Pelvic pain history
Physical Examination:
- External genitalia, vaginal mucosa (atrophy = low estrogen)
- Pelvic floor tone and tenderness
- Evidence of infection, anatomical abnormalities (vaginal septa)
Laboratory/Investigations:
- TSH, FSH, LH, Estradiol - hormonal evaluation
- Prolactin - if galactorrhea or amenorrhea
- Androgens (total testosterone, DHEA-S) - androgen insufficiency
- Fasting glucose - if diabetes suspected
- Pelvic ultrasound - if anatomical cause suspected
- Psychological screening tools - PHQ-9 (depression), GAD-7 (anxiety)
Medications Affecting Sexual Function
| Drug Class | Examples |
|---|---|
| Antihypertensives | Beta-blockers (atenolol, metoprolol), thiazide diuretics, sympatholytics (clonidine, methyldopa), CCBs |
| Antidepressants | SSRIs, TCAs (25-80% incidence of sexual side effects) |
| Antipsychotics | (via hyperprolactinemia) |
| Anxiolytics | Benzodiazepines (alprazolam, diazepam) |
| Antiandrogens | Ketoconazole, spironolactone |
| 5α-Reductase inhibitors | Finasteride, dutasteride |
| GnRH agonists | Leuprolide, buserelin |
| H2-blockers | Cimetidine |
| Opioids | Chronic use lowers testosterone |
| Statins | Atorvastatin, rosuvastatin |
| Anticonvulsants | Most (except lamotrigine); gabapentin affects orgasm |
Safe alternatives: Bupropion and mirtazapine do not appear to cause sexual side effects
PART 5: SUMMARY TABLE - INVESTIGATIONS AT A GLANCE
| Condition | Key First-Line Tests | Second/Specialist Tests |
|---|---|---|
| Male infertility | Semen analysis x2 | Testosterone, LH, FSH, prolactin; karyotype; testicular biopsy; scrotal US |
| Female infertility | Ovulation confirmation (LH kit, progesterone); Day 3 FSH/E2; pelvic US | AMH, HSG, laparoscopy, hysteroscopy, karyotype, MRI pituitary |
| Erectile dysfunction | Fasting glucose, lipids, total testosterone, TSH | LH, FSH, prolactin, NPT testing, penile Doppler US, pituitary MRI |
| Female sexual dysfunction | TSH, FSH/LH/E2, prolactin, androgens | Pelvic US, psychological assessment |
PART 6: KEY TREATMENT HIGHLIGHTS
Male Infertility:
- Varicocelectomy improves sperm parameters
- Treat infections; avoid gonadotoxins
- IUI for mild factor; ICSI for severe factor
ED:
- PDE-5 inhibitors (sildenafil, tadalafil, vardenafil) = first-line (SOR: A)
- Sildenafil onset 30-60 min (3-5 hr effect); Tadalafil onset 16-30 min (24-72 hr effect)
- Prostaglandin E1 (intracavernous or intraurethral alprostadil) = second-line
- Vacuum erection devices (VEDs) = adjunct
- Testosterone replacement if hypogonadal (see routes in Table 42-5)
- Psychotherapy + sildenafil superior to sildenafil alone
Premature Ejaculation:
- SSRIs delay ejaculation (SOR: A); dapoxetine is the only SSRI approved specifically for PE
Female Sexual Dysfunction:
- Psychosocial interventions for FSIAD
- Vaginal dilators + pelvic floor physiotherapy for genito-pelvic pain
- If SSRI-induced: add bupropion (SOR: C) or switch to bupropion/mirtazapine
- Treat underlying hormonal causes (hypothyroidism, hyperprolactinemia)
Sources: Textbook of Family Medicine 9e (Rakel) | Tietz Textbook of Laboratory Medicine 7e | Berek & Novak's Gynecology | Smith and Tanagho's General Urology 19e | Campbell Walsh Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.