Teach me ecg from basic to advance with clinical symptoms and example of ecg strips that help me to differwntiate between dofferent condt
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG interpretation basics to advanced clinical guide 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content I need to write a comprehensive, well-illustrated ECG guide. Let me compose the full answer:
ECG (Electrocardiogram): Basic to Advanced - A Complete Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Medical Physiology (Boron & Boulpaep), Frameworks for Internal Medicine, Braunwald's Heart Disease, Tintinalli's Emergency Medicine
PART 1 - FOUNDATIONS
What is an ECG?
An ECG is a surface recording of the time-dependent electrical vector of the heart. It gives direct information about rate, rhythm, and conduction. Because different parts of the heart activate sequentially, each part of the tracing maps to a specific cardiac event:
| Wave/Interval | What it represents |
|---|---|
| P wave | Atrial depolarization |
| PR interval | AV nodal conduction (atria → ventricles) |
| QRS complex | Ventricular depolarization |
| ST segment | Early ventricular repolarization |
| T wave | Ventricular repolarization |
| U wave | Repolarization of Purkinje fibers (or papillary muscles) |
| QT interval | Total ventricular electrical systole |
The ECG Paper
- Small box = 1 mm = 0.04 seconds (horizontal) = 0.1 mV (vertical)
- Large box = 5 mm = 0.2 seconds = 0.5 mV
- 5 large boxes = 1.0 second
Calculating Heart Rate (Quick Method)
Count large boxes between two R waves and apply: Rate = 300 ÷ (number of large boxes)
| R-R large boxes | Heart Rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
PART 2 - THE 12 LEADS
Limb Leads (Frontal Plane)
- Standard (bipolar): I, II, III
- Augmented (unipolar): aVR, aVL, aVF
- Key rule: Lead II is parallel to the heart's electrical axis and gives the clearest P waves
Precordial Leads (Horizontal Plane)
V1-V6 are placed across the chest. Ventricular depolarization has two phases:
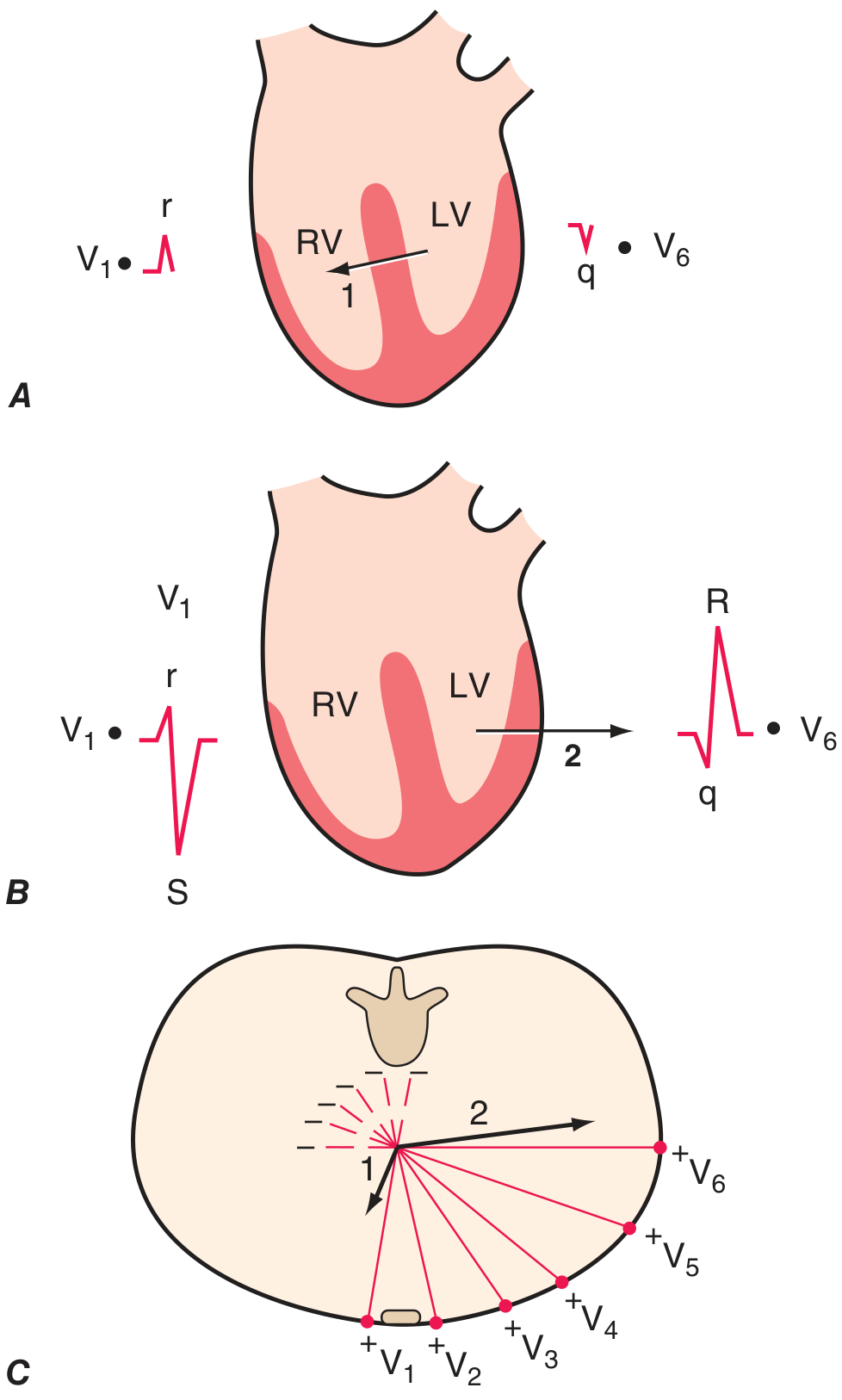
Phase 1: Septal depolarization (left → right) = small r in V1, small q in V6. Phase 2: Dominant LV depolarization (leftward/posterior) = deep S in V1, tall R in V6.
R-wave progression: R waves grow from V1 → V6. The transition (R = S) is normally at V3-V4. Poor R-wave progression (PRWP) suggests anterior MI or LVH.
PART 3 - NORMAL INTERVALS
| Measurement | Normal Range | Clinical significance of abnormality |
|---|---|---|
| PR interval | 0.12-0.20 s (3-5 small boxes) | Short = pre-excitation (WPW); Long = AV block |
| QRS duration | < 0.12 s (< 3 small boxes) | Wide = bundle branch block or ventricular beat |
| QT interval | < 0.44 s (corrected) | Long QT = risk of torsades de pointes |
| P wave | < 0.12 s duration, < 2.5 mm amplitude | Tall = RAE; wide/bifid = LAE |
PART 4 - SYSTEMATIC APPROACH (Harrison's 14-Step Method)
According to Harrison's, every ECG must be analyzed for these 14 parameters:
- Standardization/calibration and lead placement
- Rhythm
- Heart rate
- PR interval / AV conduction
- QRS interval
- QT/QTc interval
- Mean QRS electrical axis
- P waves
- QRS voltages
- Precordial R-wave progression
- Abnormal Q waves
- ST segments
- T waves
- U waves
Always compare with prior ECGs when available.
PART 5 - HEART RATE & RHYTHM DISORDERS
Normal Sinus Rhythm
- Rate 60-100 bpm
- Upright P before every QRS in II
- Regular P-P and R-R intervals
- PR 0.12-0.20 s
Sinus Tachycardia
- Rate > 100, normal morphology
- Clinical causes: fever, pain, anemia, hypovolemia, PE, hyperthyroidism, anxiety
- ECG: regular, normal P waves, rate typically 100-160
Sinus Bradycardia
- Rate < 60, normal morphology
- Clinical causes: athletes, hypothyroidism, inferior MI, vasovagal syncope, beta-blockers
- Usually benign; treat only if symptomatic
PART 6 - ATRIAL ARRHYTHMIAS
The image below from Braunwald's illustrates the key differences side by side:
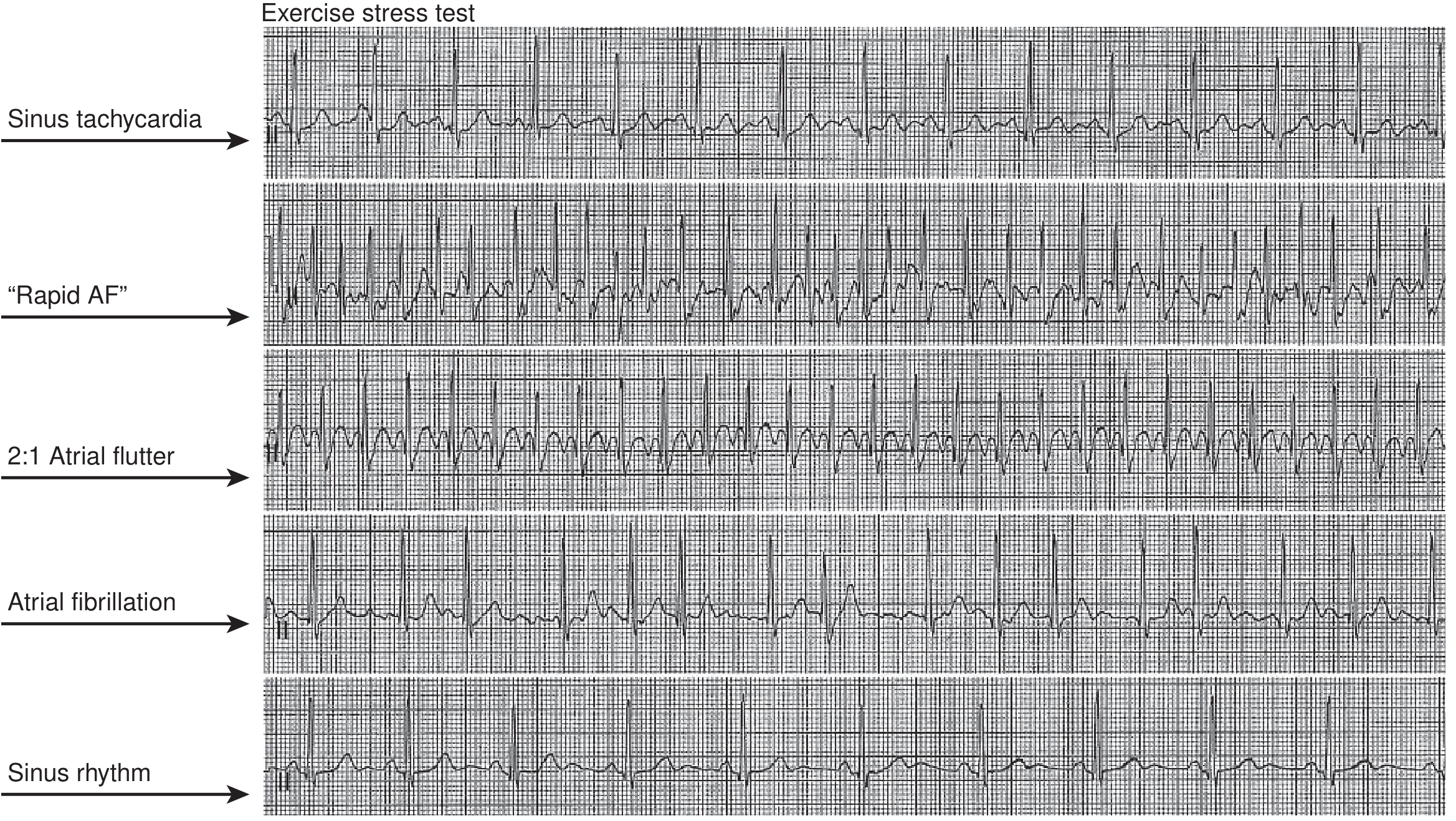
Atrial Fibrillation (AF)
- Mechanism: chaotic, disorganized atrial activity from multiple reentry circuits
- ECG features:
- No discrete P waves - replaced by irregular fibrillatory baseline
- Irregularly irregular R-R intervals (this is the key!)
- Normal QRS unless aberrant conduction
- Ventricular rate typically 100-180 bpm if uncontrolled
- Clinical: palpitations, dyspnea, fatigue, dizziness, stroke risk
- Causes: hypertension, valvular disease, HF, thyrotoxicosis, alcohol, post-cardiac surgery
Atrial Flutter
- Mechanism: single large reentry circuit in right atrium
- ECG features:
- Classic "sawtooth" flutter waves at 250-350/min (best seen in II, III, aVF)
- Usually 2:1 AV block → ventricular rate ~150 bpm (classic tip: any regular tachycardia at ~150 bpm = flutter until proven otherwise)
- Regular or regularly-irregular rhythm
- Clinical: palpitations, dyspnea; less embolic risk than AF but still warrants anticoagulation
Multifocal Atrial Tachycardia (MAT)
- Rate 100-180 bpm, irregularly irregular
- Key differentiator from AF: 3+ distinct P-wave morphologies, visible P waves before each QRS
- Clinical: almost exclusively associated with severe COPD, hypoxia, theophylline toxicity, hypomagnesemia
Quick Differentiation: AF vs. AFL vs. MAT
| Feature | AF | Atrial Flutter | MAT |
|---|---|---|---|
| P waves | None (fibrillatory) | Sawtooth flutter waves | 3+ morphologies |
| Rhythm | Irregularly irregular | Regular (or regularly irregular) | Irregularly irregular |
| Rate | Variable | ~150 (2:1 block) | 100-180 |
| Association | HTN, valvular dz, alcohol | Structural heart disease | COPD, hypomagnesemia |
PART 7 - AV CONDUCTION BLOCKS
First-Degree AV Block
- ECG: PR interval > 0.20 s (> 1 large box), every P followed by QRS
- Clinical: usually benign; seen with increased vagal tone, inferior MI, digoxin, beta-blockers
- No treatment needed
Second-Degree AV Block - Mobitz Type I (Wenckebach)
- ECG: Progressive PR lengthening → dropped QRS → cycle repeats
- Memory: "Longer, longer, longer... DROP. Then you have a Wenckebach"
- Site of block: Usually at AV node
- Clinical: Often benign, may be vagal (athletes), inferior MI; rarely needs pacing
Second-Degree AV Block - Mobitz Type II
- ECG: Constant PR interval, then sudden dropped QRS (no warning)
- Site of block: Below AV node (His-Purkinje system)
- Clinical: DANGEROUS - unpredictable, can progress to complete heart block; wide QRS common; pacemaker often indicated
- Associated with anterior MI, degenerative conduction disease
Third-Degree (Complete) AV Block
- ECG: Complete AV dissociation - P waves and QRS complexes march independently with no relationship
- P rate > QRS rate
- QRS may be narrow (junctional escape, ~40-60 bpm) or wide (ventricular escape, ~30-40 bpm)
- Clinical: Severe bradycardia, syncope (Stokes-Adams attacks), hemodynamic compromise
- EMERGENCY - requires temporary then permanent pacemaker
- Causes: inferior MI (often transient), anterior MI (often permanent), Lyme disease, digoxin toxicity, infiltrative disease
AV Block Comparison Table
| Block | PR interval | Dropped beats | Emergency? |
|---|---|---|---|
| 1st degree | Fixed, prolonged | Never | No |
| 2nd degree Mobitz I | Progressively lengthens | Yes, with pattern | No (usually) |
| 2nd degree Mobitz II | Fixed, then suddenly dropped | Yes, without warning | Yes |
| 3rd degree (complete) | Dissociated | All - complete AV dissociation | YES |
PART 8 - BUNDLE BRANCH BLOCKS
Key rule: QRS ≥ 0.12 s (3 small boxes) = bundle branch block
Right Bundle Branch Block (RBBB)
- ECG features:
- Wide QRS ≥ 0.12 s
- RSR' pattern ("bunny ears") in V1 - the second R is taller
- Wide, slurred S wave in I and V6
- Secondary ST-T changes in right precordial leads
- Mnemonic: MaRRoW - RBBB has M shape in V1, W shape in V6
- Clinical: May be normal variant; also RV strain (PE, pulmonary hypertension), anterior MI, myocarditis
Left Bundle Branch Block (LBBB)
- ECG features:
- Wide QRS ≥ 0.12 s
- Broad monophasic R in I, aVL, V5, V6 (no septal q waves)
- Deep QS or rS in V1
- Secondary ST-T changes opposite to QRS direction
- Mnemonic: WiLLiaM - LBBB has W in V1, M in V6
- Clinical: ALWAYS pathological - CAD, cardiomyopathy, severe LVH, aortic stenosis
- New LBBB with chest pain = STEMI equivalent, treat as ACS
RBBB vs. LBBB at a glance:
| Feature | RBBB | LBBB |
|---|---|---|
| V1 | RSR' (M shape) | QS or rS (W shape) |
| V6/I | Wide S wave | Broad R, no q waves |
| Significance | May be normal | Always abnormal |
| ST changes | In V1-V3 (discordant) | Diffuse discordant |
PART 9 - ISCHEMIA, INJURY & INFARCTION
The sequence of ECG changes in MI follows a classic progression:
Ischemia → Injury → Infarction
| Stage | ECG Finding | Time course |
|---|---|---|
| Hyperacute | Tall, peaked T waves (earliest sign) | Minutes |
| Injury (STEMI) | ST elevation ≥ 1 mm in 2 contiguous leads | Minutes-hours |
| Evolving | Q waves develop (pathological = ≥ 0.04 s wide, ≥ 25% QRS amplitude) | Hours-days |
| Subacute | T-wave inversions | Hours-days |
| Old MI | Persistent Q waves, T wave may normalize | Weeks-permanent |
ST Elevation - Localizing the Infarct
| Leads with ST elevation | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| V1-V2 | Septal | LAD (septal branches) |
| V3-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx |
| II, III, aVF | Inferior | RCA (80%) or LCx (20%) |
| V7-V9 (or reciprocal changes V1-V2) | Posterior | RCA or LCx |
Reciprocal changes: ST depression in leads opposite the infarct zone confirms STEMI and excludes pericarditis (which has diffuse ST elevation without reciprocal changes).
STEMI vs. Pericarditis vs. Early Repolarization
| Feature | STEMI | Pericarditis | Early Repolarization |
|---|---|---|---|
| ST shape | Convex/domed ("tombstone") | Concave ("saddle shape") | Concave with J-point notching |
| Distribution | Regional/contiguous | Diffuse (all leads except aVR) | Usually V2-V5 in young males |
| Reciprocal changes | Yes | No (PR depression instead) | No |
| Q waves | Develop | No | No |
| PR depression | No | YES (pathognomonic) | No |
The ECG strip of subarachnoid hemorrhage vs. normal - QT effects:
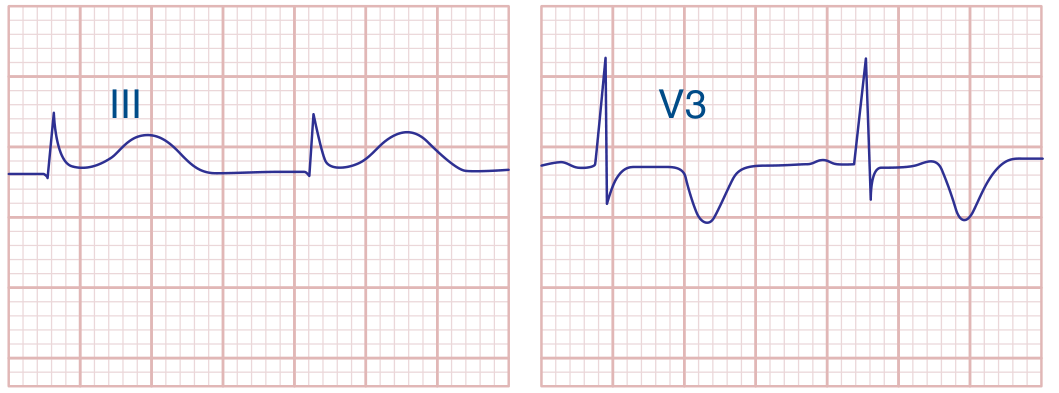
Lead III (left): Subarachnoid hemorrhage causing deep T-wave inversion and prolonged QT. V3 (right): Anterior MI with deep ST changes.
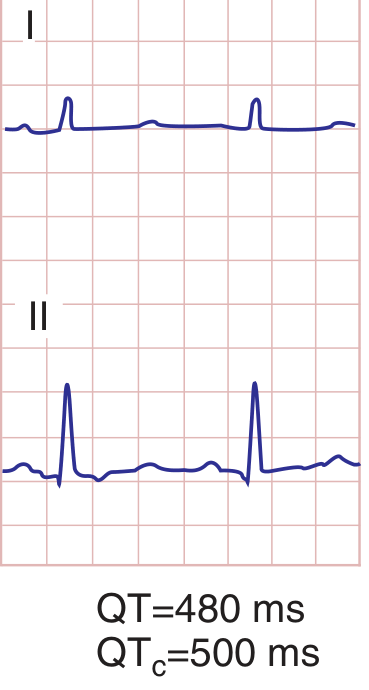
PART 10 - QT INTERVAL & DANGEROUS REPOLARIZATION
Corrected QT (QTc)
Use Bazett's formula: QTc = QT / √(R-R interval in seconds)
- Normal QTc: < 440 ms (men), < 460 ms (women)
- QTc > 500 ms = HIGH risk of torsades de pointes (TdP)
Causes of Long QT
| Category | Examples |
|---|---|
| Drugs | Antiarrhythmics (amiodarone, sotalol, quinidine), antibiotics (azithromycin, fluoroquinolones), antipsychotics (haloperidol, quetiapine), methadone |
| Electrolytes | Hypokalemia, hypomagnesemia, hypocalcemia |
| Congenital | Romano-Ward syndrome, Jervell and Lange-Nielsen syndrome |
| CNS disease | Subarachnoid hemorrhage, stroke, meningitis |
| Hypothyroidism, hypothermia |
Short QT
- Hypercalcemia shortens ST segment → short QT
- Digoxin toxicity: "scooped" ST with shortened QT (digitalis effect)
The Hypocalcemia vs. Hypercalcemia ECG:
Hypocalcemia: prolonged ST segment = long QT. Normal: standard QT. Hypercalcemia: abbreviated ST, short QT.
PART 11 - VENTRICULAR ARRHYTHMIAS
Premature Ventricular Complexes (PVCs)
- Wide QRS (> 0.12 s) with bizarre morphology, no preceding P wave
- Usually followed by compensatory pause
- Isolated PVCs are common and often benign
- Frequent PVCs (> 10% of beats) with symptoms or reduced EF need evaluation
Ventricular Tachycardia (VT)
- Definition: ≥ 3 consecutive wide complex beats at > 100 bpm
- ECG features:
- Wide, bizarre QRS complexes (> 0.12 s)
- AV dissociation (independent P waves - look for "marching" P waves)
- Fusion beats (sinus + VT = intermediate morphology) - pathognomonic
- Capture beats (sinus captures ventricle briefly - narrow QRS amid wide beats)
- Concordance (all chest leads positive or all negative)
- Clinical: Palpitations, syncope, hemodynamic collapse
- Rule: Wide complex tachycardia = VT until proven otherwise
Distinguishing VT from SVT with Aberrancy (Brugada Algorithm)
- No RS complex in any precordial lead? → VT
- RS interval > 100 ms in any precordial lead? → VT
- AV dissociation? → VT
- LBBB morphology with QRS negative in V1 and positive in V6, OR RBBB morphology with positive concordance? → VT
Ventricular Fibrillation (VF)
- ECG: Chaotic, irregular deflections with no identifiable QRS, ST, or T waves
- Clinical: No cardiac output = cardiac arrest
- Treatment: Immediate defibrillation + CPR
Torsades de Pointes (TdP)
- VT with QRS complexes that "twist" around the baseline (polymorphic VT)
- Occurs in setting of prolonged QT
- Treatment: IV magnesium sulfate, correct electrolytes, remove causative drugs; overdrive pacing
PART 12 - CARDIAC TAMPONADE
The classic tamponade triad on ECG (Beck's ECG triad):
- Sinus tachycardia
- Low QRS voltages (< 5 mm in limb leads, < 10 mm in precordial leads)
- Electrical alternans (alternating QRS amplitude due to swinging heart)
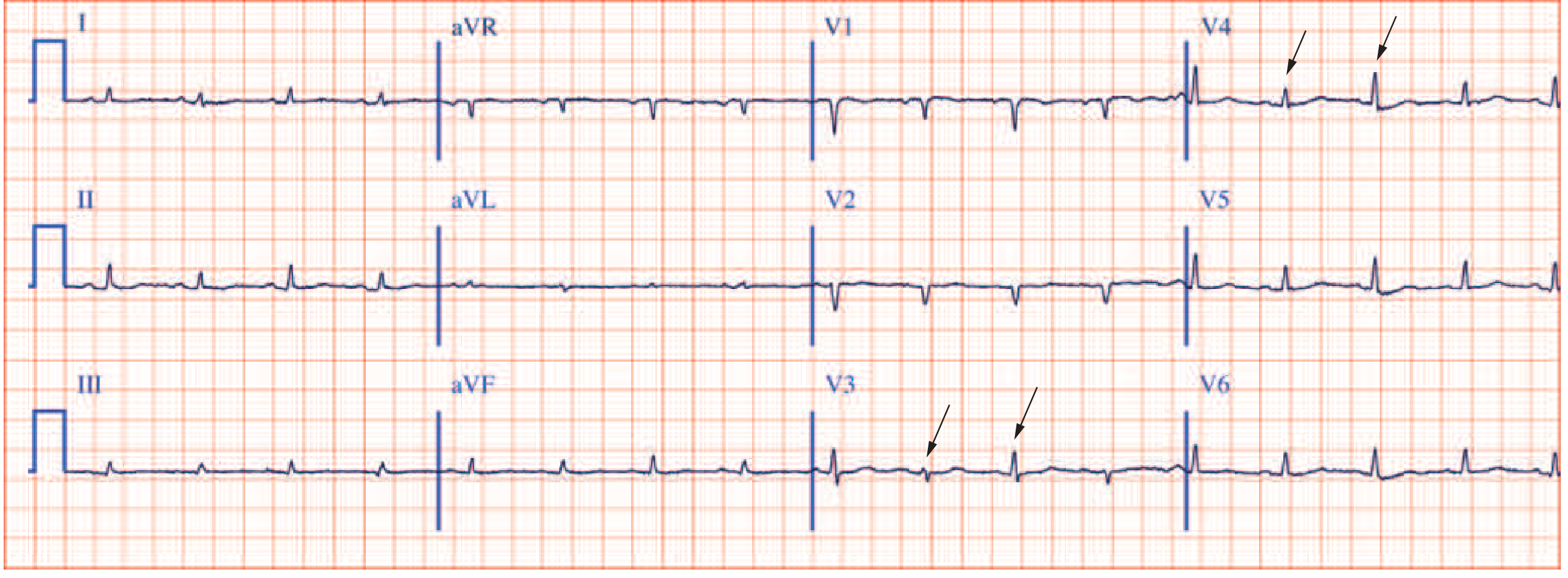
This 12-lead shows all three tamponade features: tachycardia, low voltages, and beat-to-beat QRS alternation (arrows in V3, V4).
PART 13 - ADVANCED PATTERNS
Wolf-Parkinson-White (WPW)
- ECG features:
- Short PR (< 0.12 s) - early ventricular activation via accessory pathway
- Delta wave - slurred upstroke of QRS
- Wide QRS, ST-T changes (discordant to delta wave)
- Clinical: Palpitations, SVT (usually narrow but can be wide if antidromic), risk of sudden death in AF
- DANGER: Do NOT give AV nodal blocking drugs (adenosine, beta-blockers, digoxin) in WPW with AF - can accelerate conduction via accessory pathway → VF
Brugada Syndrome
- ECG features: Coved-type (Type 1) ST elevation in V1-V2 with RBBB-like pattern, terminal negative T wave
- Clinical: Young males, Asian descent, sudden cardiac death during sleep/rest
- Type 1 (diagnostic): Coved ST elevation ≥ 2 mm descending to inverted T wave
Hyperkalemia (Progressive Changes with Increasing K+)
| K+ Level | ECG Change |
|---|---|
| 5.5-6.5 mEq/L | Peaked, narrow, symmetrical T waves |
| 6.5-7.5 mEq/L | PR prolongation, QRS widening, P-wave flattening |
| 7.5-8.0 mEq/L | P waves disappear, wide bizarre QRS ("sine wave") |
| > 8.0 mEq/L | VF or asystole |
Hypokalemia
- ST depression, T-wave flattening/inversion
- Prominent U waves (U > T wave = significant hypokalemia)
- QT(U) prolongation → risk of TdP
Digitalis Effect vs. Toxicity
- Effect (therapeutic): Scooped ST ("reverse tick" or "Salvador Dali mustache"), short QT, PR prolongation - expected finding
- Toxicity: PAT with block (rapid atrial tachycardia with AV block), PVCs, bidirectional VT, any arrhythmia + AV block
Pulmonary Embolism (PE)
- Most common: sinus tachycardia (most sensitive finding)
- Classic S1Q3T3 pattern (S wave in I, Q wave + T inversion in III) - specific but insensitive
- RBBB (acute or incomplete) from RV strain
- T-wave inversions V1-V4 (RV strain pattern)
- Right axis deviation
Hypothermia
- Osborn (J) wave: Positive deflection at J point (junction of QRS and ST segment), best seen in V4-V6 and II
- Bradycardia, prolonged intervals (PR, QRS, QT), muscle tremor artifact
PART 14 - MASTER DIFFERENTIATOR TABLE
| Condition | Key ECG Finding | Clinical Clue |
|---|---|---|
| Normal sinus rhythm | Regular, P before QRS, rate 60-100 | Asymptomatic |
| Sinus tachycardia | Rate >100, normal morphology | Fever, pain, hypovolemia |
| AF | Irregular irregular, no P waves | Palpitations, stroke risk |
| Atrial flutter | Sawtooth at 300/min, rate ~150 | Palpitations, regular |
| MAT | 3+ P morphologies, irregular | COPD, ICU patient |
| 1° AV block | Long PR (>0.20 s) | Benign, inferior MI |
| Mobitz I | PR lengthens then drops | Inferior MI, benign |
| Mobitz II | Fixed PR then sudden drop | Anterior MI, dangerous |
| Complete heart block | P and QRS dissociated | Syncope, emergency |
| RBBB | RSR' in V1, S in V6 | RV strain, PE, variant |
| LBBB | Wide R in V6, QS in V1 | Always pathological |
| Anterior STEMI | ST elevation V1-V4 | Chest pain, LAD occlusion |
| Inferior STEMI | ST elevation II, III, aVF | Chest pain, RCA occlusion |
| NSTEMI/UA | ST depression, T inversion | Chest pain, no ST elevation |
| Pericarditis | Diffuse ST elevation, PR depression | Pleuritic chest pain, fever |
| Tamponade | Low voltage + alternans + tachycardia | Beck's triad clinically |
| LVH | Tall R in V5/V6, deep S in V1 (Sokolow: SV1+RV5 >35 mm) | HTN, aortic stenosis |
| WPW | Short PR, delta wave | Young, SVT, sudden death risk |
| Hyperkalemia | Peaked T waves → sine wave | Renal failure, severe |
| Hypokalemia | ST depression, U waves | Diuretics, vomiting |
| Long QT | QTc > 440-460 ms | Drug effects, electrolytes |
| Brugada | Coved ST in V1-V2 | Young male, sleep arrest |
| PE | S1Q3T3 + tachycardia | Sudden dyspnea, pleuritic pain |
| Hypothermia | Osborn (J) wave | Cold exposure |
| SAH | Deep T inversion, long QT | Worst headache of life |
PART 15 - CLINICAL PEARLS
-
Wide complex tachycardia = VT until proven otherwise. Never give verapamil empirically - it can cause hemodynamic collapse in VT.
-
New LBBB + chest pain = treat as STEMI (Sgarbossa criteria can help if previous LBBB exists).
-
Any rate of ~150 bpm = think atrial flutter with 2:1 block first.
-
AV dissociation (P waves independent of QRS) = complete heart block OR VT - both are serious.
-
The first ECG change in STEMI is hyperacute T waves, not ST elevation. Do not miss this.
-
Reciprocal changes confirm STEMI and rule against pericarditis (pericarditis has no reciprocal changes but has PR depression).
-
Osborn waves + bradycardia = hypothermia until proven otherwise.
-
Peaked T waves in a dialysis patient = hyperkalemia emergency.
-
Electrical alternans = pericardial effusion/tamponade until proven otherwise.
-
Short PR + delta wave + wide QRS = WPW - do NOT use digoxin or AV nodal blockers if they develop AF.
For Further Practice
The best online free ECG library is LITFL ECG Library - it has hundreds of annotated strips organized by diagnosis. ECG Made Simple offers free interactive video tutorials. Harvard's ECG Wave-Maven provides case-based self-assessment.
- Harrison's Principles of Internal Medicine 22E, Chapter 247
- Medical Physiology (Boron & Boulpaep), Chapter 21, Box 21-2
- Braunwald's Heart Disease, 12th Ed - Chapter 12
- Frameworks for Internal Medicine - AV Block and Arrhythmia chapters
- Tintinalli's Emergency Medicine - Chapter 18
This is a shared conversation. Sign in to Orris to start your own chat.