DIC
Reading File
Finding Sources
Searching PubMed
"disseminated intravascular coagulation" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Disseminated Intravascular Coagulation (DIC)
Definition
DIC is an acquired clinicopathologic syndrome in which systemic activation of both coagulation and fibrinolysis occurs simultaneously, resulting in widespread microvascular thrombosis, consumption of clotting factors and platelets, and secondary fibrinolytic activation. The paradoxical result is concurrent bleeding AND thrombosis - Robbins & Kumar Basic Pathology describes it as probably causing bleeding more commonly than all congenital coagulation disorders combined.
Pathophysiology
The diagram below summarizes the mechanism:
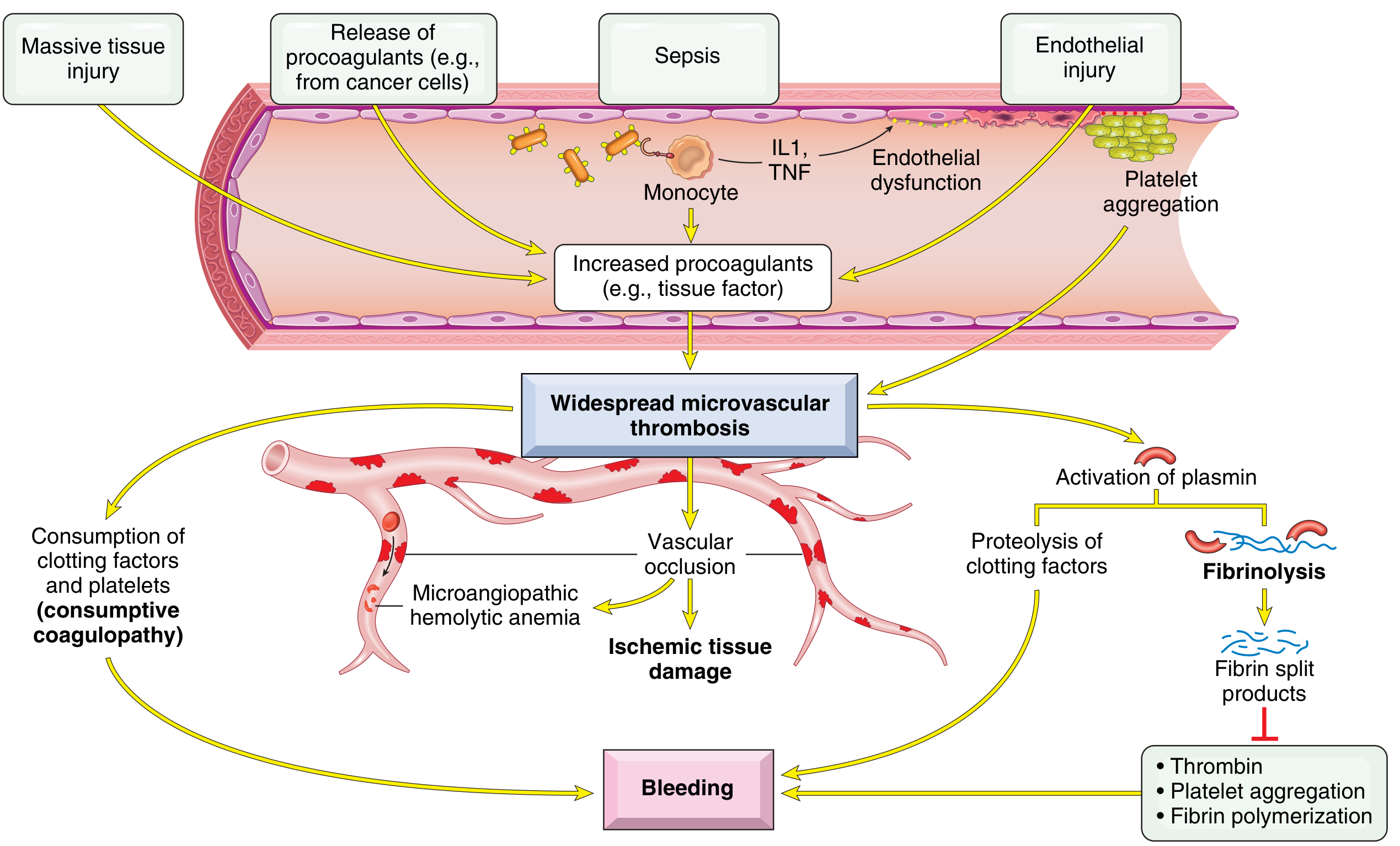
Fig. 10.30 - Robbins & Kumar Basic Pathology
DIC is triggered by two main mechanisms:
1. Release of tissue factor (thromboplastin) into circulation
- Obstetric complications (placenta, amniotic fluid)
- Cancer cells (especially acute promyelocytic leukemia, adenocarcinoma)
- Massive tissue injury releasing thromboplastic material
2. Widespread endothelial cell damage
- In bacterial sepsis: endotoxins/exotoxins stimulate tissue factor expression on monocytes. Activated monocytes release IL-1 and TNF, which simultaneously stimulate tissue factor expression on endothelial cells AND downregulate thrombomodulin (which activates protein C, an anticoagulant)
- Antigen-antibody complex deposition (e.g., SLE)
- Temperature extremes (heat stroke, burns)
- Meningococci, rickettsiae
Once thrombin is generated and overwhelms its inhibitor system, it:
- Deposits fibrin in small vessels of multiple organs
- Consumes platelets and clotting factors (especially fibrinogen, factors V, VIII, XIII) - consumptive coagulopathy
- Activates plasminogen activators - secondary fibrinolysis
Plasmin then:
- Cleaves fibrin and factors V and VIII
- Produces fibrin degradation products (FDPs/D-dimers) that: inhibit platelet aggregation, exert anti-thrombin activity, and impair fibrin polymerization - all worsening bleeding
The result: microangiopathic hemolytic anemia (RBCs shredded on fibrin strands) + ischemic tissue damage + bleeding diathesis
Causes / Triggers
| Category | Examples |
|---|---|
| Obstetric | Abruptio placentae, amniotic fluid embolism, retained dead fetus (prothrombotic DIC), septic abortion, eclampsia, HELLP syndrome |
| Infections | Sepsis (gram-negative > gram-positive), meningococcemia, Rocky Mountain spotted fever, fungemia, malaria |
| Malignancy | Acute promyelocytic leukemia (APL), pancreatic/prostate/lung/gastric carcinoma |
| Massive tissue injury | Trauma (especially brain), burns, extensive surgery, aortic surgery with hypothermia |
| Miscellaneous | Acute intravascular hemolysis, snakebite, giant hemangioma, heat stroke, shock, liver disease, vasculitis, aortic aneurysm |
Note: Retained dead fetus causes a prothrombotic (not hemorrhagic) DIC - normal to shortened APTT (elevated FVIII as acute-phase reactant), mildly reduced platelets, normal/elevated fibrinogen, but elevated D-dimers.
Clinical Features
Bleeding manifestations:
- Oozing from venipuncture sites, wounds, surgical incisions
- Mucosal bleeding (gums, GI tract)
- Petechiae and ecchymoses
- In severe cases: major hemorrhage
Thrombotic manifestations:
- Purpura fulminans (skin necrosis from dermal vessel thrombosis)
- Acral ischemia / digit gangrene
- Renal failure (glomerular fibrin thrombi)
- Altered mental status, focal neurological deficits
- Adrenal hemorrhage (Waterhouse-Friderichsen in meningococcemia)
Microangiopathic hemolytic anemia (MAHA)
Morphology (Autopsy Findings)
Microthrombi are most often found in:
- Kidneys - glomerular fibrin thrombi, cortical necrosis in severe cases
- Adrenals - bilateral hemorrhagic infarction
- Brain - microinfarcts
- Heart - subendocardial microthrombi
- No organ is spared
(Robbins & Kumar Basic Pathology, p. 427)
Laboratory Diagnosis
The ISTH Overt DIC Score (used when an underlying disorder is confirmed):
| Test | Findings | Score |
|---|---|---|
| Platelet count | >100k = 0; <100k = 1; <50k = 2 | 0-2 |
| D-dimer (fibrin marker) | <0.4 µg/mL = 0; 0.4-4.0 = 2; >4.0 = 3 | 0-3 |
| PT prolongation | <3 sec = 0; 3-6 sec = 1; >6 sec = 2 | 0-2 |
| Fibrinogen | >100 mg/dL = 0; <100 mg/dL = 1 | 0-1 |
- Score ≥5 = compatible with overt DIC (repeat daily)
- Score <5 = suggestive of non-overt DIC (repeat in 1-2 days)
Lab profile table (from Rosen's Emergency Medicine):
| Test | Finding | Mechanism |
|---|---|---|
| Peripheral smear | Low platelets, schistocytes, RBC fragments | RBC fragmentation on fibrin strands |
| Platelet count | Low (usually <100,000/mm³) | Consumed in clotting |
| PT | Prolonged | Factors II and IV consumed |
| PTT | Prolonged | Factors II, V, VIII consumed |
| Thrombin time | Prolonged | Decreased fibrinogen; in vivo fibrinolysis |
| Fibrinogen | Low (but may be deceptively normal as acute-phase reactant) | Consumed |
| D-dimer/FDPs | Elevated | Secondary fibrinolysis |
| Creatinine/UA | May be abnormal | Renal microvascular fibrin deposition |
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Severe liver disease | Clinical jaundice, splenomegaly; factor VIII is normal (not synthesized by liver, so not low in liver failure); no fibrinolysis |
| Primary fibrinolysis | Rare; affects fibrinogen and fibrin but generally preserves platelets, factor V, and factor VIII in low-normal range |
| TTP/HUS | Thrombocytopenia + MAHA but coagulation tests (PT, PTT) usually normal |
| HELLP syndrome | Overlaps with DIC; if not resolved by day 3 postpartum, consider TTP |
Management
Step 1: Treat the underlying cause (always first)
Many episodes are self-limited (e.g., transfusion reaction) or compensated (tumor-associated). Treating the trigger alone resolves DIC in many cases.
Step 2: Specific intervention based on clinical picture
Active bleeding / risk of bleeding with invasive procedure:
- Fresh frozen plasma (FFP) - corrects multiple factor deficiencies
- Cryoprecipitate - maintain fibrinogen >100 mg/dL
- Platelet transfusion - maintain count >20 × 10⁹/L
- Monitor: slowing of bleeding, falling FDPs, rising platelet count and fibrinogen
- Note: In non-bleeding patients with only lab DIC, do not give blood products - this can "add fuel to the fire" by exacerbating microthrombus formation
Thrombosis-predominant DIC (fibrin deposition > bleeding):
- Heparin (unfractionated or LMWH) is indicated
- Specific indications: purpura fulminans, retained dead fetus, giant hemangioma, APL
- Low-dose UFH (3-5 IU/kg/hour) in non-bleeding patients with lab DIC can help neutralize thrombin
- Heparin is not beneficial in: meningococcemia, abruptio placentae, severe liver disease, trauma
Other agents evaluated but not proven to improve outcomes:
- Antithrombin III concentrate
- Prothrombin complex concentrate (PCC)
- Recombinant factor VIIa
- Activated protein C
Monitoring
- Repeat ISTH DIC score daily (in overt DIC)
- Track: fibrinogen, platelet count, PT/aPTT, D-dimers
- Normalization of clotting times occurs later in the course - less useful as an early monitor
- Also track renal function (common early organ impact)
Recent Evidence (2025)
A 2025 ISTH meta-analysis (PMID 40383152) systematically characterized DIC mortality, diagnosis, and etiology across studies - confirming sepsis and malignancy as the leading triggers with high associated mortality. Japan's 2024 clinical practice guidelines (PMID 39674834) provide updated DIC management recommendations specifically for hematologic malignancy.
Key Sources:
- Robbins & Kumar Basic Pathology, p. 427
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 954
- Rosen's Emergency Medicine, Chapter 111
This is a shared conversation. Sign in to Orris to start your own chat.