Psoas abcess as 10 marks question for postgraduate
Reading File
Finding Sources
Finding Sources
Searching PubMed
"psoas abscess" diagnosis management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete postgraduate-level 10-mark answer.
Psoas Abscess - Postgraduate 10 Marks Answer
Definition
A psoas (iliopsoas) abscess is a purulent collection within the psoas muscle or its fascial sheath, located entirely within the retroperitoneal compartment. It may involve the iliacus muscle as well, forming an "iliopsoas abscess."
Anatomy - Why It Matters
The psoas major originates from the transverse processes and lateral bodies of T12-L5 vertebrae, descends along the lateral aspect of the spine, passes beneath the inguinal ligament, and inserts into the lesser trochanter of the femur after joining the iliacus (forming the iliopsoas). The muscle is enclosed in a fascial sheath that communicates:
- Superiorly with the posterior mediastinum (via aortic hiatus)
- Inferiorly with the femoral triangle (via subinguinal space)
- Medially with the vertebral column and adjacent retroperitoneal structures
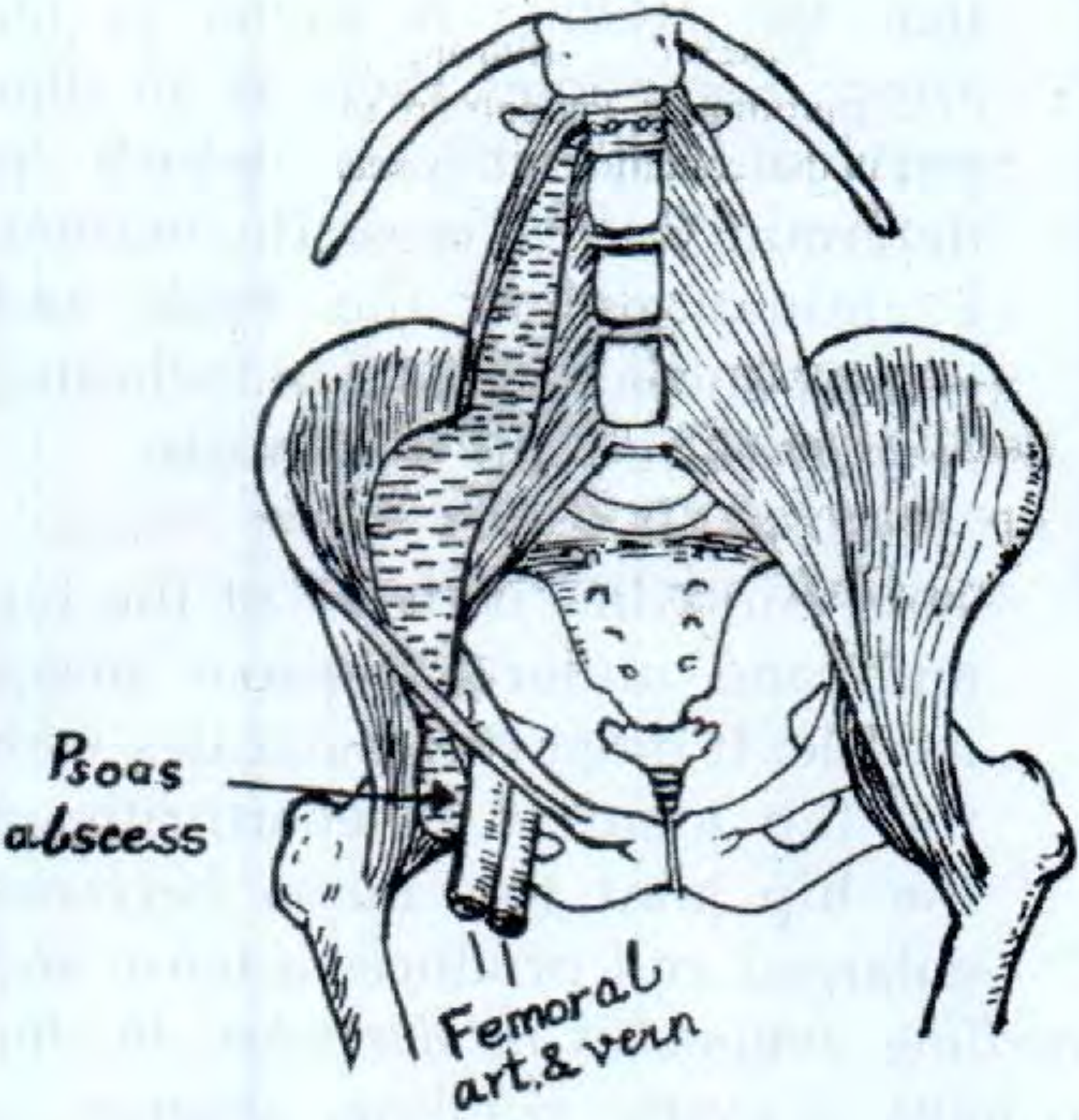
This sheath allows pus to track from spinal disease down to the groin (or even the adductor region of the thigh), forming the classic "cold abscess pointing in the groin."
Classification
| Type | Description |
|---|---|
| Primary | Haematogenous spread from an occult source; no identifiable adjacent focus; seen in immunocompromised, IV drug users, diabetics; commonest organism: Staphylococcus aureus |
| Secondary | Direct spread from contiguous structures - most common type overall |
Aetiology / Causes
Secondary Sources (most common today):
- Spinal / vertebral column - Pott's disease (TB spondylitis, historically the #1 cause), pyogenic vertebral osteomyelitis, discitis
- Gastrointestinal - Crohn's disease (most common GI cause today), appendicitis with perforation, diverticulitis, carcinoma colon, sigmoid abscess
- Urinary - Perinephric abscess, renal stone with infection, pyelonephritis
- Gynaecological - Pelvic inflammatory disease, tubo-ovarian abscess, septic abortion, infected caesarean haematoma
- Vascular - Infected aortic aneurysm or graft, infected retroperitoneal haematoma
Microbiology:
- Primary abscess: S. aureus (most common, including MRSA)
- Secondary abscess (spinal/skeletal origin): S. aureus, Mycobacterium tuberculosis
- Secondary abscess (GI/GU origin): Mixed enteric organisms - aerobic and anaerobic gram-negative bacilli (E. coli, Bacteroides, Streptococcus milleri group, Klebsiella)
(Harrison's Principles of Internal Medicine, 22E)
Pathogenesis
In Pott's disease, the TB bacillus seeds the cancellous bone of the vertebral body near the intervertebral disc. Bone destruction progresses; the infected disc material extrudes anteriorly into the psoas muscle sheath. Pus then tracks distally within the fascial sheath, passes beneath the inguinal ligament, and points as a fluctuant swelling in the femoral triangle lateral to the femoral vessels. (Gray's Anatomy for Students)
In secondary GI disease (e.g., Crohn's), transmural inflammation leads to direct fistulation into the psoas sheath.
Clinical Features
Symptoms:
- Back/loin pain (most common) - lumbar or lower thoracic in location
- Fever - usually low-grade in TB (cold abscess); high spiking fever in pyogenic abscess
- Groin swelling - the pathognomonic feature when pus has tracked down
- Hip pain - referred to the hip or knee
- Weight loss, anorexia (especially TB)
Signs:
- Flexion deformity of the hip - the patient lies with the thigh flexed to relax the psoas (Thomas's test positive)
- Psoas sign - pain on passive extension of the hip (stretches the muscle over the abscess)
- Fluctuant groin swelling - lateral to the femoral artery and vein (differentiates from femoral hernia, which is medial to femoral vein)
- Reducible swelling with cough impulse in cold abscess
- Cross-fluctuation between iliac fossa mass and groin swelling (when large)
- Signs of primary pathology - spinal tenderness, kyphosis, restricted spinal movements (TB); abdominal mass/tenderness (Crohn's)
The "classic triad" of psoas abscess:
Back pain + Fever + Limp (hip flexion)
Differential Diagnosis of Groin Swelling (from psoas abscess)
- Inguinal hernia (medial to ASIS, above and medial to pubic tubercle)
- Femoral hernia (medial to femoral vein)
- Femoral artery aneurysm (pulsatile, expansile)
- Enlarged inguinal lymph nodes (multiple, firm)
- Saphena varix (impulse on coughing, empties on lying)
- Psoas bursa enlargement (Bailey & Love, 28th Ed)
Key point: Psoas abscess points lateral to the femoral vessels; femoral hernia lies medial to them.
Investigations
Bloods:
- FBC: leukocytosis (pyogenic), lymphocytosis (TB)
- ESR, CRP elevated
- Blood cultures (positive in ~50% of pyogenic cases)
- Mantoux/IGRA test (if TB suspected)
Imaging:
| Investigation | Findings |
|---|---|
| X-ray spine/pelvis | Vertebral body destruction, disc space narrowing, loss of psoas shadow, paraspinal shadow |
| Ultrasound | Initial screening; shows a hypoechoic/anechoic mass in the psoas; useful for guiding aspiration |
| CT abdomen/pelvis (Gold Standard) | Defines the extent precisely, identifies source, guides percutaneous drainage; shows hypodense mass within or adjacent to psoas, may show gas, adjacent vertebral erosion |
| MRI | Best for soft tissue detail and spinal cord involvement; superior for Pott's disease |

Microbiological:
- Aspiration of pus for Gram stain, culture & sensitivity (aerobic + anaerobic)
- AFB smear and culture, PCR for TB
- Histopathology of tissue if TB or malignancy suspected
Treatment
1. Antibiotic Therapy
- Empirical antibiotics directed at likely organisms, then tailored to culture results
- Pyogenic (primary/S. aureus): Anti-staphylococcal antibiotics (flucloxacillin; vancomycin if MRSA suspected); IV initially, then oral for total 4-6 weeks
- GI source: Broad spectrum covering gram-negatives and anaerobes (piperacillin-tazobactam, or carbapenems in severe sepsis)
- TB: Standard anti-tuberculous therapy (HRZE for 2 months then HR for 4-7 months minimum)
2. Drainage of the Abscess (mandatory)
Primary treatment is drainage + antibiotics.
(a) Percutaneous CT/Ultrasound-Guided Drainage
- Preferred first-line approach for most patients
- CT-guided aspiration or drain placement
- Safe, minimally invasive, can be repeated
- Success rate ~80-90% for pyogenic abscesses
(b) Surgical Drainage - indicated when:
- Percutaneous drainage fails
- Multilocular abscess
- Underlying pathology requiring surgery (e.g., bowel resection for Crohn's, debridement for TB spondylitis)
- Abscess pointing superficially in the thigh
Surgical approaches:
| Approach | Details |
|---|---|
| Posterior (Petit triangle approach) | 7.5 cm incision 2.5 cm above posterior iliac crest; blunt dissection through obliquus internus into the abscess. Postop: Buck traction for flexion contracture correction |
| Lateral (iliac crest) approach | 10 cm incision along the middle third of the iliac crest; puncture abscess on inner surface of iliac wing |
| Anterior (subinguinal) | When abscess points under Poupart's ligament into the groin |
| Ludloff incision | When abscess points subcutaneously in the adductor region of the thigh |
(Campbell's Operative Orthopaedics, 15th Ed 2026)
Postoperative care: Buck traction is applied postoperatively to correct flexion contracture of the hip and relax the spastic psoas muscle until full extension is restored.
3. Treatment of the Primary Cause
- Spinal TB: anti-tuberculous therapy; surgery (decompression/stabilisation) if neurological deficit
- Crohn's disease: medical therapy, bowel resection if necessary
- GI perforation/diverticulitis: appropriate surgical management
- Renal source: treat underlying cause (nephrolithiasis, perinephric abscess)
Complications
- Untreated: septicaemia, multi-organ failure, death
- Hip joint infection (due to proximity of iliopsoas to the hip capsule)
- Femoral nerve palsy (pressure neuropathy - femoral neuropathy more common with iliacus abscess, as the iliacus fascia is less distensible)
- Flexion contracture of the hip
- Fistula formation (enterocutaneous, spino-cutaneous)
- Recurrence if underlying cause not treated
Prognosis
With prompt CT-guided drainage and appropriate antibiotic therapy, the prognosis is generally good. Mortality was historically high (>90% untreated) but is now <5% with modern management. Delayed diagnosis remains the major determinant of poor outcome. TB psoas abscess has an excellent outcome with ATT, though the cavities may persist radiologically.
Summary Points for Exam
| Feature | Cold (TB) Psoas Abscess | Hot (Pyogenic) Psoas Abscess |
|---|---|---|
| Cause | Pott's disease (TB spine) | S. aureus, enteric organisms |
| Onset | Insidious, months | Acute |
| Fever | Low grade | High, spiking |
| Pain | Mild | Severe |
| X-ray | Vertebral erosion, paraspinal shadow | May show gas in abscess |
| Treatment | ATT + drainage | Antibiotics + drainage |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed | Harrison's Principles of Internal Medicine 22E | Campbell's Operative Orthopaedics 15th Ed 2026 | Gray's Anatomy for Students | S Das Manual of Clinical Surgery 13th Ed | Rheumatology 2-Volume Set (Elsevier 2022)
Recent evidence: Armenta-Flores et al. (2026) - Iliopsoas Abscess Narrative Review in World J Surg confirms CT-guided percutaneous drainage as first-line, with surgical drainage reserved for failures. Al-Khafaji et al. (2024) systematic review supports CT as the gold standard imaging modality for diagnosis and drainage guidance.
This is a shared conversation. Sign in to Orris to start your own chat.