Explain me ecg and 10 common clinical cases
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content needed to write a thorough, well-illustrated answer. Here is the full response:
Electrocardiogram (ECG): A Complete Guide
What is an ECG?
An ECG (electrocardiogram) is a graphical recording of the electrical activity of the heart over time. It captures the voltage differences generated by cardiac depolarization and repolarization, detected by electrodes placed on the skin surface. It is the single most important noninvasive test in cardiology - cheap, fast, and enormously informative.
Part 1: ECG Basics
The ECG Paper
ECG paper has a standard grid:
- Horizontal axis = time: each small box = 0.04 s (40 ms); each large box (5 mm) = 0.2 s
- Vertical axis = voltage: each small box = 0.1 mV; each large box = 0.5 mV
Heart rate calculation: Rate = 300 ÷ (number of large boxes between consecutive R waves). For example, 4 large boxes apart = 75 bpm.
The Normal ECG Waveform

Figure: Basic ECG waveforms and intervals (Harrison's Principles of Internal Medicine, 22E)
| Component | Origin | Normal Duration |
|---|---|---|
| P wave | Atrial depolarization (SA node → atria) | <120 ms; positive in II, negative in aVR |
| PR interval | Atrial depol + AV node delay | 120-200 ms |
| QRS complex | Ventricular depolarization | ≤100-110 ms |
| ST segment | Between ventricular depol & repol | Isoelectric (at baseline) |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | Total ventricular electrical activity | <450 ms (men), <460 ms (women) |
| U wave | Purkinje fiber repolarization | Small, follows T wave |
The 12 Leads
The 12 leads "look" at the heart from different angles - like 12 cameras filming the same event.
6 Limb (frontal plane) leads: I, II, III, aVR, aVL, aVF
- Look at the heart from the front (superior-inferior, left-right axis)
- Normal QRS axis: -30° to +90°
6 Precordial (horizontal plane) leads: V1-V6
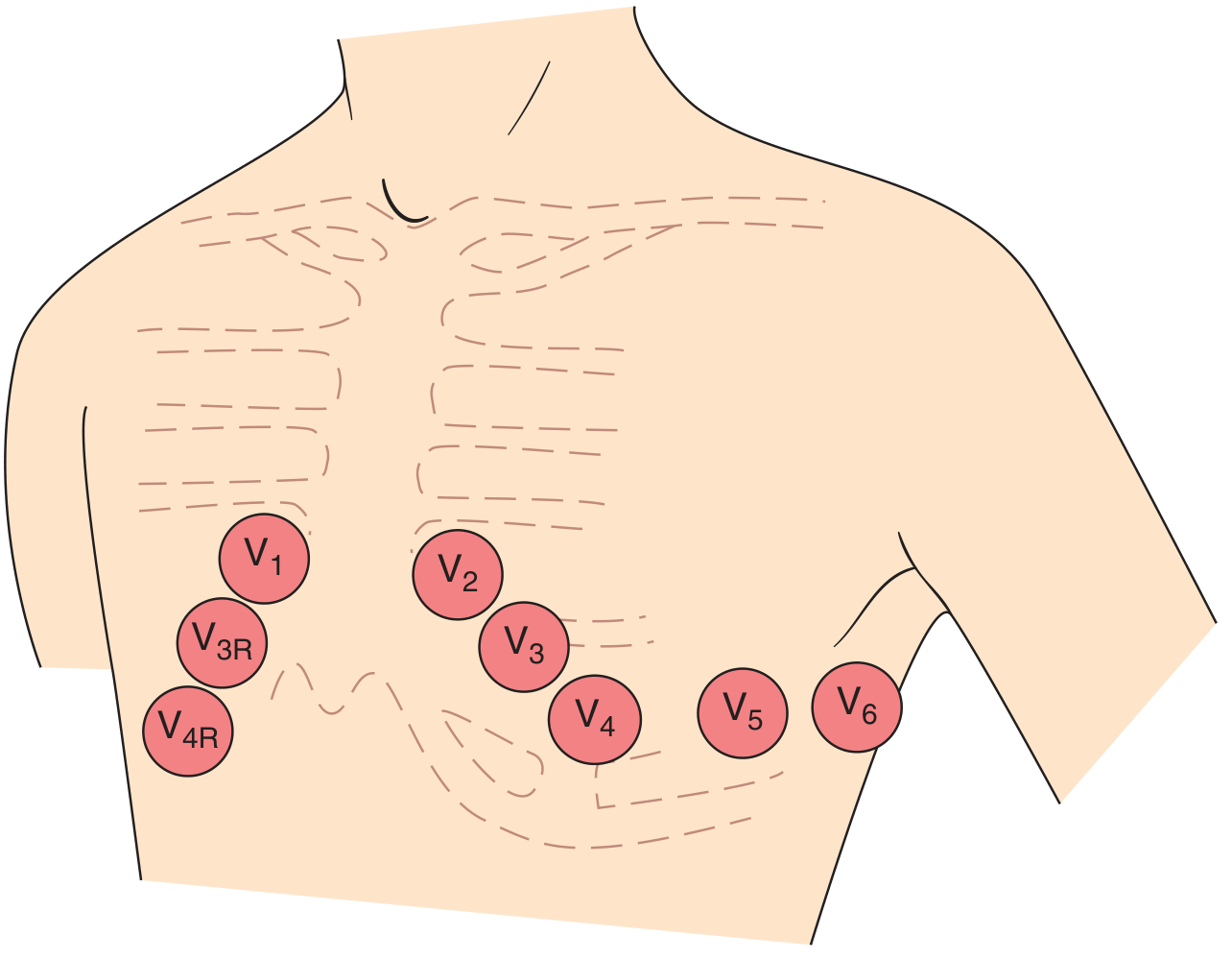
Figure: Standard precordial lead electrode positions (Harrison's, 22E)
| Lead | Position | What it sees |
|---|---|---|
| V1 | 4th intercostal space, right sternal border | RV, septum |
| V2 | 4th intercostal space, left sternal border | Septum |
| V3 | Between V2 and V4 | Anterior wall |
| V4 | 5th intercostal space, midclavicular line | Anterior-lateral LV |
| V5 | Anterior axillary line, same level as V4 | Lateral LV |
| V6 | Midaxillary line, same level as V4 | Lateral LV |
Ventricular Depolarization (QRS Formation)
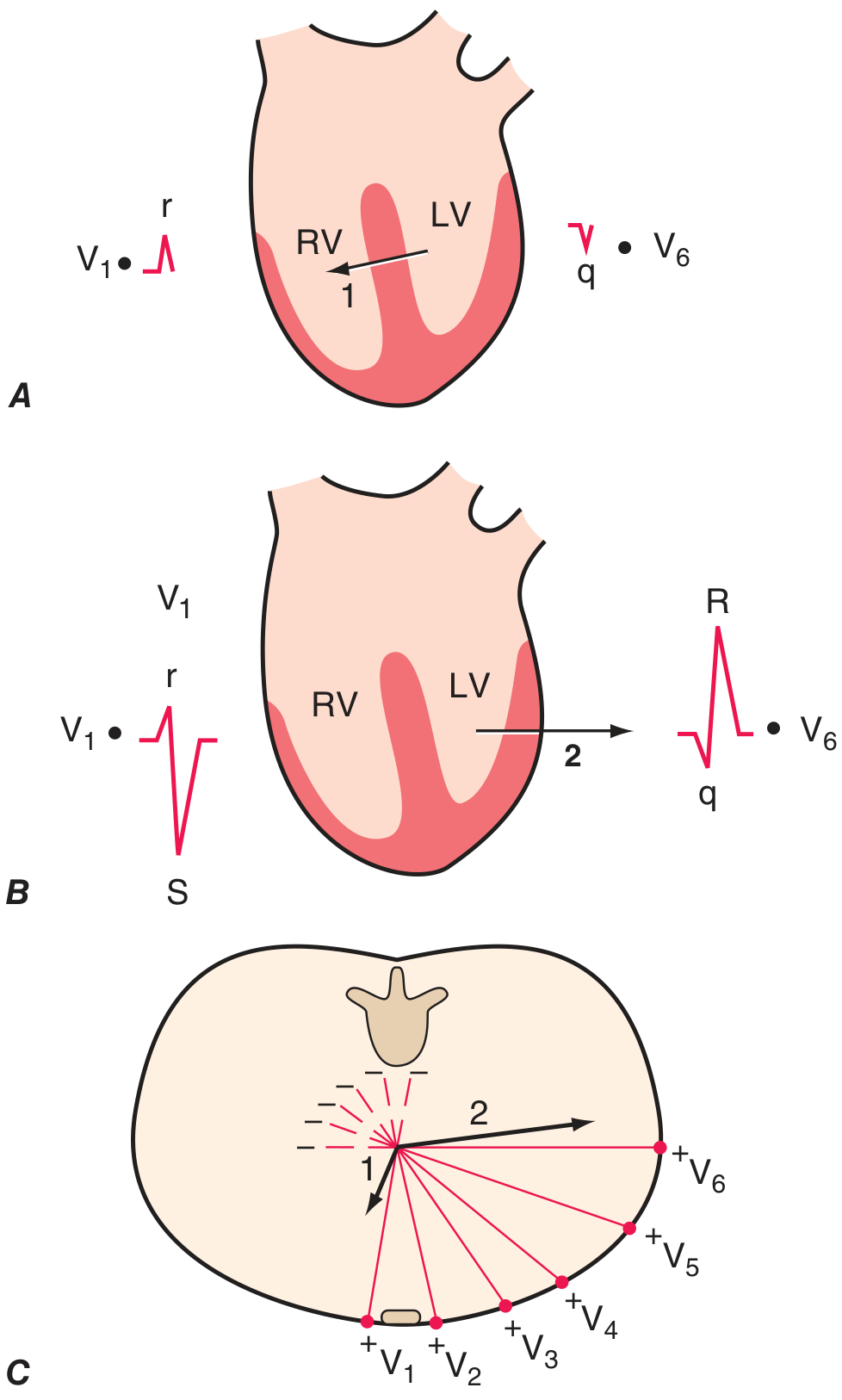
Figure: Ventricular depolarization phases (Harrison's, 22E, adapted from Goldberger's Clinical Electrocardiography)
- Phase 1: Septal depolarization, left → right → small r in V1, small q in V6
- Phase 2: Main LV depolarization, left/posterior dominant → rS in V1, tall R in V6
- R-wave "progression" from V1 (small r) to V6 (tall R) is a key normal finding
The 14-Step Systematic Approach to ECG Interpretation
Per Harrison's Principles of Internal Medicine (22E), every ECG should be analyzed for:
- Standardization and technical quality (calibration, lead placement, artifacts)
- Rhythm (sinus vs. other)
- Heart rate
- PR interval / AV conduction
- QRS interval
- QT / QTc interval
- Mean QRS electrical axis
- P waves (morphology, relation to QRS)
- QRS voltages (high or low)
- Precordial R-wave progression (V1 → V6)
- Abnormal Q waves
- ST segments
- T waves
- U waves
Part 2: 10 Common Clinical ECG Cases
Case 1: Normal Sinus Rhythm
Presentation: 35-year-old for a pre-employment physical. No symptoms.
ECG findings:
- Regular rhythm, rate 60-100 bpm
- Upright P wave in II before every QRS; negative P in aVR
- PR interval 120-200 ms
- Narrow QRS (<110 ms)
- Normal R-wave progression V1→V6
Teaching point: Confirm sinus rhythm by finding a P wave that is positive in lead II and negative in aVR before every QRS. This confirms the SA node is the pacemaker.
Case 2: ST-Elevation Myocardial Infarction (STEMI)
Presentation: 58-year-old man with crushing central chest pain radiating to the left arm for 45 minutes. Diaphoretic. BP 100/70.
ECG findings:
- Hyperacute T waves (early): tall, peaked T waves in the territory
- ST elevation ≥1 mm in two or more contiguous leads
- Q wave formation (pathological, >40 ms wide or >25% of R height) in later stages
- Reciprocal ST depression in opposite leads
Territories:
| Territory | Leads | Culprit Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA (or LCx) |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | V1-V2 ST depression + tall R | RCA/LCx |
| Right ventricular | V1, V4R | Proximal RCA |
Teaching point: ST elevation in II, III, aVF with reciprocal depression in I/aVL = inferior STEMI until proven otherwise. Always get right-sided leads (V3R, V4R) to rule out RV infarction.
(Harrison's, 22E - "Profound ST elevation or depression in multiple leads usually indicates very severe ischemia.")
Case 3: Atrial Fibrillation (AF)
Presentation: 72-year-old woman with palpitations and mild dyspnea. Pulse is "irregularly irregular."
ECG findings:
- Absent P waves - replaced by irregular fibrillatory baseline (f waves, 350-600/min)
- Irregularly irregular RR intervals (the hallmark)
- Narrow QRS (unless aberrant conduction)
- Rate typically 100-160 bpm if uncontrolled
Teaching point: If you see an irregular rhythm with no clear P waves, it is AF until proven otherwise. Use CHA₂DS₂-VASc score to assess stroke risk and decide on anticoagulation. Rate control target <110 bpm at rest.
Case 4: Atrial Flutter
Presentation: 65-year-old post-cardiac surgery with palpitations. Ventricular rate exactly 150 bpm.
ECG findings:
- "Sawtooth" flutter waves at 300/min in inferior leads (II, III, aVF)
- Regular atrial rate ~300/min with 2:1 AV block → ventricular rate ~150 bpm
- Can be 3:1 or 4:1 block (rate 100 or 75 bpm)
- No true isoelectric baseline between flutter waves
Teaching point: When you see a regular tachycardia at exactly 150 bpm, think flutter with 2:1 block. Carotid sinus massage or adenosine can slow the ventricular rate transiently, revealing the sawtooth flutter waves.
Case 5: First-Degree AV Block
Presentation: 68-year-old asymptomatic man. Incidental finding on screening ECG. On metoprolol for hypertension.
ECG findings:
- PR interval >200 ms (one large box)
- Every P wave is followed by a QRS (1:1 conduction)
- Otherwise normal
Teaching point: This is a benign finding in most cases. Common causes include increased vagal tone, AV node disease, digoxin, beta-blockers, calcium channel blockers. No treatment required in isolation.
Case 6: Complete (Third-Degree) AV Block
Presentation: 78-year-old with syncope and bradycardia (HR 35 bpm). BP 85/60.
ECG findings:
- AV dissociation: P waves and QRS complexes march independently at their own rates
- P rate > QRS rate (e.g., P at 80/min, QRS at 35/min)
- QRS may be wide (ventricular escape rhythm from below the Bundle of His) or narrow (junctional escape)
- No consistent PR interval
Teaching point: This is a medical emergency. The atria and ventricles are completely disconnected. Immediate transcutaneous pacing, then transvenous pacing, and ultimately permanent pacemaker implantation. IV atropine may be used as a bridge.
Case 7: Left Bundle Branch Block (LBBB)
Presentation: 55-year-old with newly diagnosed heart failure and ECG showing wide QRS.
ECG findings:
- Wide QRS ≥120 ms
- Broad, notched ("M-shaped") R wave in lateral leads (I, aVL, V5, V6) - the classic "W" on the right (V1) and "M" on the left
- Deep S or QS pattern in V1
- No septal q waves in lateral leads (since septal activation is reversed)
- ST and T wave changes in the opposite direction to the QRS (discordant)
Teaching point: New LBBB in the setting of chest pain is treated as a STEMI equivalent (Sgarbossa criteria can help identify true STEMI on top of LBBB). Isolated chronic LBBB usually indicates structural heart disease (cardiomyopathy, hypertension).
Case 8: Ventricular Tachycardia (VT)
Presentation: 62-year-old with known ischemic cardiomyopathy presenting with palpitations, near-syncope, BP 85/60.
ECG findings:
- Wide QRS tachycardia (QRS >120 ms) at rate 150-250 bpm
- AV dissociation (P waves visible, independent from QRS) - pathognomonic of VT
- Fusion beats or capture beats - also diagnostic
- Positive or negative concordance across precordial leads (all pointing same direction)
- Axis deviation
Teaching point: Wide complex tachycardia in a patient with structural heart disease = VT until proven otherwise. Do not give verapamil (can cause cardiovascular collapse). AV dissociation clinches the diagnosis. Hemodynamically unstable: immediate DC cardioversion.
(Goldman-Cecil Medicine: "For wide-QRS complex tachycardias, the 12-lead ECG is useful in distinguishing SVT with aberrancy from VT. The presence of fusion beats or AV dissociation during a wide-QRS complex tachycardia strongly supports VT.")
Case 9: Wolff-Parkinson-White (WPW) Syndrome
Presentation: 22-year-old with recurrent episodes of rapid palpitations since adolescence.
ECG findings (in sinus rhythm):
- Short PR interval (<120 ms) - bypasses AV node delay
- Delta wave - slurred upstroke of the QRS (pre-excitation via accessory pathway)
- Wide QRS (>120 ms) - QRS is widened by the delta wave
- Secondary ST-T changes (discordant with QRS)
ECG findings during tachycardia (orthodromic AVRT - most common):
- Narrow QRS tachycardia, 160-220 bpm
- Retrograde P waves often visible after QRS
Teaching point: If AF develops in WPW, the accessory pathway can conduct very rapidly to the ventricles → potentially fatal ventricular fibrillation. NEVER give adenosine, verapamil, or digoxin in AF+WPW (they block the AV node but not the accessory pathway, increasing conduction down the accessory pathway). Use procainamide or DC cardioversion.
Case 10: Long QT Syndrome and Torsades de Pointes
Presentation: 45-year-old woman on cisapride (or fluconazole + azithromycin) presenting with recurrent syncope. ECG shows QTc 520 ms.
ECG findings:
- Prolonged QTc: >450 ms in men, >460 ms in women (markedly prolonged if >500 ms)
- T wave abnormalities: notched, broad, or biphasic T waves
- Torsades de Pointes (TdP): the arrhythmia that results from long QT
- Polymorphic VT where QRS complexes appear to "twist" around the isoelectric baseline
- Rate 200-250 bpm, often self-terminating but can degenerate into VF
Common causes of acquired long QT:
- Drugs: antiarrhythmics (sotalol, amiodarone), antibiotics (azithromycin), antifungals (fluconazole), antipsychotics (haloperidol), cisapride
- Electrolytes: hypokalemia, hypomagnesemia, hypocalcemia
- Congenital: Romano-Ward syndrome, Jervell-Lange-Nielsen syndrome
Teaching point: Correct electrolytes. Stop offending drugs. For TdP: IV magnesium sulfate 2g is the treatment of choice. Temporary pacing or isoproterenol can also "overdrive" suppress TdP by shortening the QT interval.
(Harrison's, 22E - "Prolongation of the QT interval (ST-segment portion) is typical of hypocalcaemia. Hypercalcaemia may cause abbreviation of the ST segment with relative or absolute shortening of the QT interval.")
Quick-Reference Summary Table
| # | Condition | Key ECG Feature | Rate | Rhythm |
|---|---|---|---|---|
| 1 | Normal Sinus Rhythm | P before every QRS, narrow | 60-100 | Regular |
| 2 | STEMI | ST elevation ≥1 mm, 2+ contiguous leads | Variable | Usually regular |
| 3 | Atrial Fibrillation | No P waves, irregular RR | Variable | Irregularly irregular |
| 4 | Atrial Flutter | Sawtooth waves, 2:1 AV block | 150 (2:1) | Regular |
| 5 | 1° AV Block | PR >200 ms, normal conduction | Normal | Regular |
| 6 | Complete Heart Block | P and QRS independent (AV dissociation) | 30-45 | Regular (slow) |
| 7 | LBBB | Wide QRS, M-pattern V5-V6, W in V1 | Normal | Regular |
| 8 | Ventricular Tachycardia | Wide complex, AV dissociation, fusion beats | 150-250 | Regular |
| 9 | WPW | Short PR, delta wave, wide QRS | Variable | Variable |
| 10 | Long QT / Torsades | QTc >460-500 ms; twisting QRS in TdP | 200-250 (TdP) | Irregular (TdP) |
Sources
- Harrison's Principles of Internal Medicine, 22E (2025), Chapter 247: Electrocardiography
- Medical Physiology (Boron & Boulpaep), Box 21-2: Basic Interpretation of the Electrocardiogram
- Goldman-Cecil Medicine, International Edition
- Tintinalli's Emergency Medicine, 9E
- Goldberger's Clinical Electrocardiography: A Simplified Approach, 10th ed. (2024)
This is a shared conversation. Sign in to Orris to start your own chat.