make notes on acute aortic syndrom - blunt trauma aorta with pictures and all from standard sources mch ctvs level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the key content and images. Let me compile the comprehensive MCh/CTVS-level notes.
Acute Aortic Syndrome & Blunt Traumatic Aortic Injury
MCh / CTVS Level Notes
Sources: Grainger & Allison's Diagnostic Radiology (9780323760751), Miller's Anesthesia 10e (9780323935920), Braunwald's Heart Disease (9780323722193)
PART 1: ACUTE AORTIC SYNDROME (AAS)
Definition
Acute aortic syndrome is an umbrella term for three distinct but pathologically inter-related aortic emergencies that share similar clinical presentations:
- Aortic Dissection (AD)
- Intramural Haematoma (IMH)
- Penetrating Atherosclerotic Ulcer (PAU)
The key link: all three involve disruption of the aortic media. They are interconvertible - PAU can cause IMH, IMH can progress to dissection, and a thrombosed false lumen of dissection may look identical to IMH.
Pathological Relationships
| Entity | Initiating Event | Mechanism |
|---|---|---|
| Aortic Dissection | Intimal tear (shear stress) OR vasa vasorum haemorrhage | Blood enters and tracks through medial dissection plane |
| IMH | Spontaneous vasa vasorum rupture OR microscopic intimal tear | Haemorrhage confined within media, no communication with lumen |
| PAU | Ulcerating atherosclerotic plaque erodes into media | Penetration can extend to adventitia, causing IMH or focal dissection |
Three-quarters of AAS presentations are aortic dissection; 10-20% are IMH; a small proportion are PAU.
- Grainger & Allison, p.2061
Clinical Presentation of AAS
- Classic: Abrupt onset severe tearing or ripping chest pain, often interscapular
- Pain may be anterior, abdominal, or migratory
- A small proportion have clinically silent dissection
Complications / Associated Features:
- Cerebrovascular accident (arch vessel occlusion)
- Renal failure
- Acute bowel or limb ischaemia (branch vessel occlusion - malperfusion syndrome)
- Myocardial infarction (coronary ostial involvement)
- Acute aortic regurgitation (aortic root involvement)
- Pericardial tamponade
- Massive haemothorax with shock (rupture)
- Progression to aneurysm
AAS Classification: Stanford / DeBakey
| Stanford | DeBakey | Involves | Frequency | Management |
|---|---|---|---|---|
| Type A | I, II | Ascending aorta ± arch | 75% | Emergency surgery |
| Type B | III | Descending aorta only (distal to L. subclavian) | 25% | Medical / TEVAR |
Temporal classification:
- Acute: < 14 days
- Subacute: 14 days - 2 months
- Chronic: > 2 months
1A. Aortic Dissection
Epidemiology:
- Incidence: 5-10 per 100,000/year, increasing with ageing population
- Risk factors: Hypertension (most common), Marfan syndrome, Ehlers-Danlos, bicuspid aortic valve, pre-existing TAA, vasculitides
Prognosis (untreated):
- 20% die before reaching hospital
- Type A: ~1-3% mortality per hour for first 48 hours; 30-day mortality ~50% with medical therapy, ~17% with surgery
- Type B (uncomplicated): 30-day mortality ~10%; complications occur in 30% (20% mortality at 48 h, 30% at 30 days)
Medical Management (all types - initial):
- High-dependency environment, invasive monitoring
- Heart rate target: <60 bpm
- Systolic BP target: <120 mmHg
- IV β-blockade (e.g. esmolol, labetalol) + IV nitrates
- Pain control
Type A: Emergency Surgery
- Indicated in all patients - immediate surgical repair
- Fatal complications if delayed: aortic rupture, cardiac tamponade, acute AR, AMI
- Arch vessel involvement: high neurological complication risk
- Requires CPB with or without DHCA
Type B: Complication-Specific Approach
- Uncomplicated: Medical therapy alone OR TEVAR + medical (INSTEAD trial: TEVAR improves 5-year aorta-specific survival and delays disease progression)
- Complicated type B: Urgent intervention (TEVAR preferred)
Indications for urgent treatment of Type B dissection:
| Indication | Status |
|---|---|
| Rupture (blood outside vessel wall) | Absolute |
| Major vessel occlusion / malperfusion | Absolute |
| Rapid expansion to total aortic diameter ≥4.5 cm | Absolute |
| Uncontrolled pain | Relative |
| Worsening radiological findings | Relative |
Prognostic factors favoring treatment in uncomplicated Type B:
- False lumen expansion rate >1 cm/year
- False lumen diameter >2.2 cm
- Early combined diameter >4 cm
- Entry tear diameter >1 cm
- Partial false lumen thrombosis
TEVAR technique for Type B dissection:
- Coverage of the main proximal entry tear with a stent-graft to depressurise the false lumen (FL) and allow true lumen (TL) re-expansion
- Goal: complete FL collapse or thrombosis (protects against rupture and aneurysm)
- Adjunctive branch stenting or fenestration for static vessel occlusion
TEVAR outcomes vs surgery:
- In-hospital mortality: 4% (TEVAR) vs 40% (open surgery) vs 33% (medical)
- Survival at 5 years: 79% (TEVAR) vs 44% (surgery/medical)
- Grainger & Allison, p.2062-2063
CT Imaging of Aortic Dissection
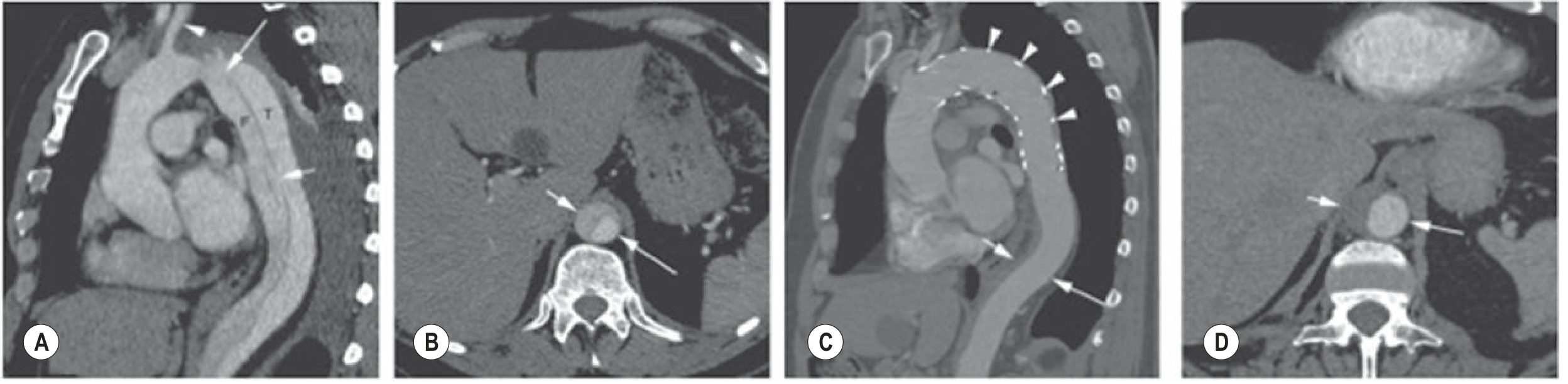
Fig. 79.18: Acute type B dissection with TEVAR - false lumen thrombosis and collapse
Branch Vessel Occlusion in Dissection
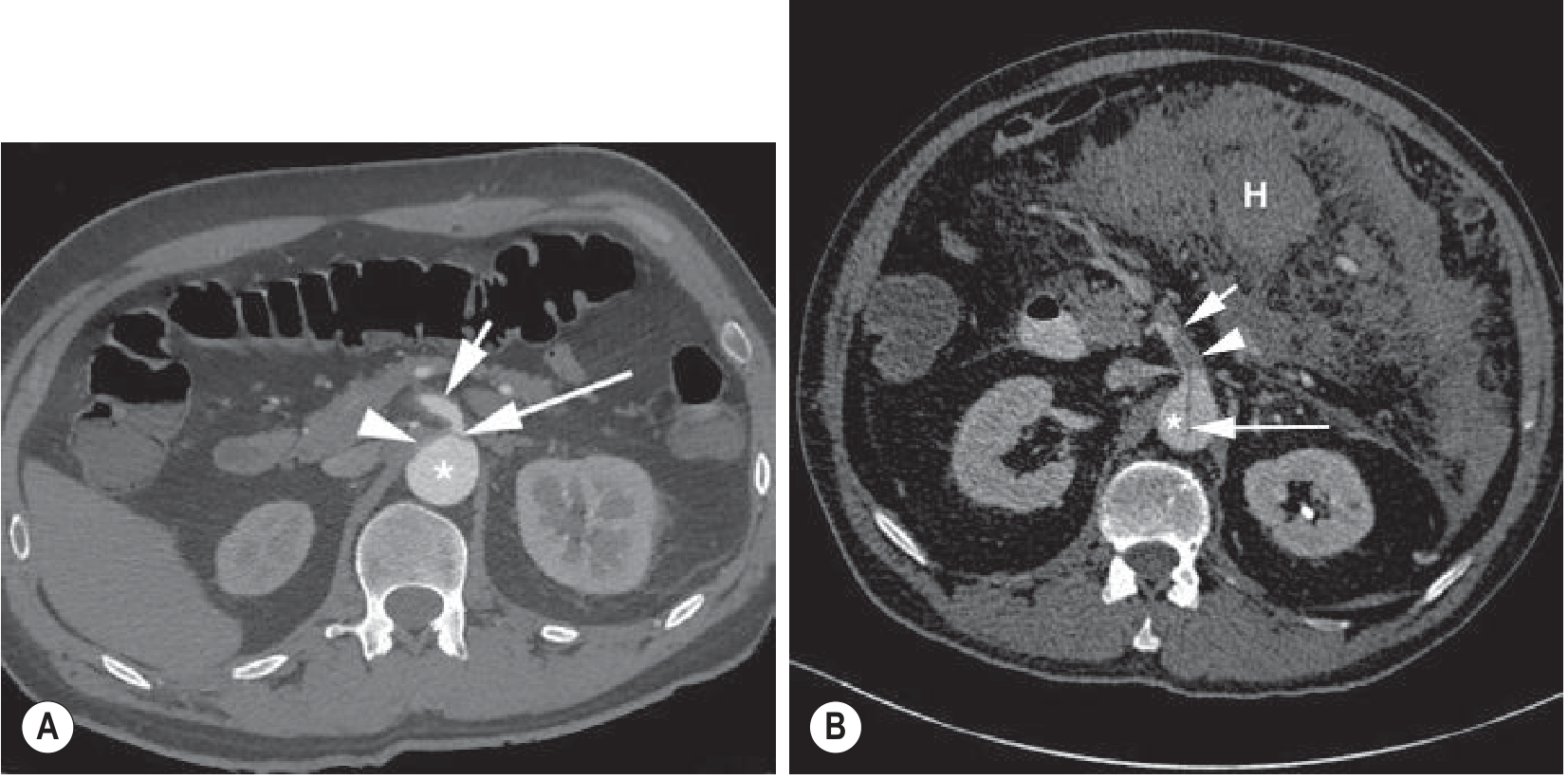
Fig. 79.17: Dynamic (left) vs static (right) branch vessel occlusion
- Dynamic occlusion: Flap prolapses across ostium - treated by FL depressurisation (TEVAR covers entry tear)
- Static occlusion: Dissection extends into branch vessel - requires additional branch stenting or fenestration
1B. Intramural Haematoma (IMH)
- Definition: Intramural haemorrhage from vasa vasorum (no intimal tear identifiable)
- More commonly involves descending thoracic aorta; older patients
- CT appearance: Crescent-shaped high-density thickening of aortic wall (no contrast in haematoma)
- Can evolve: IMH → PAU (develops over days-weeks) → dissection or rupture
- Management: Broadly similar to dissection by Stanford type
- Type A IMH: Surgery
- Type B IMH (complicated): TEVAR covering involved segment
- Grainger & Allison, p.2061
1C. Penetrating Atherosclerotic Ulcer (PAU)
- Definition: Ulcerating atheromatous plaque eroding through intima into media
- Usually in markedly atheromatous segments, most commonly descending thoracic aorta
- CT: Eccentric outpouching with adjacent wall hyperdensity (IMH)
- Risk: More prone to rupture than dissection (penetrates deeper layers)
- Management: Treat PAU as the "entry tear" - short stent-grafts; acute persistent pain is an indication for treatment
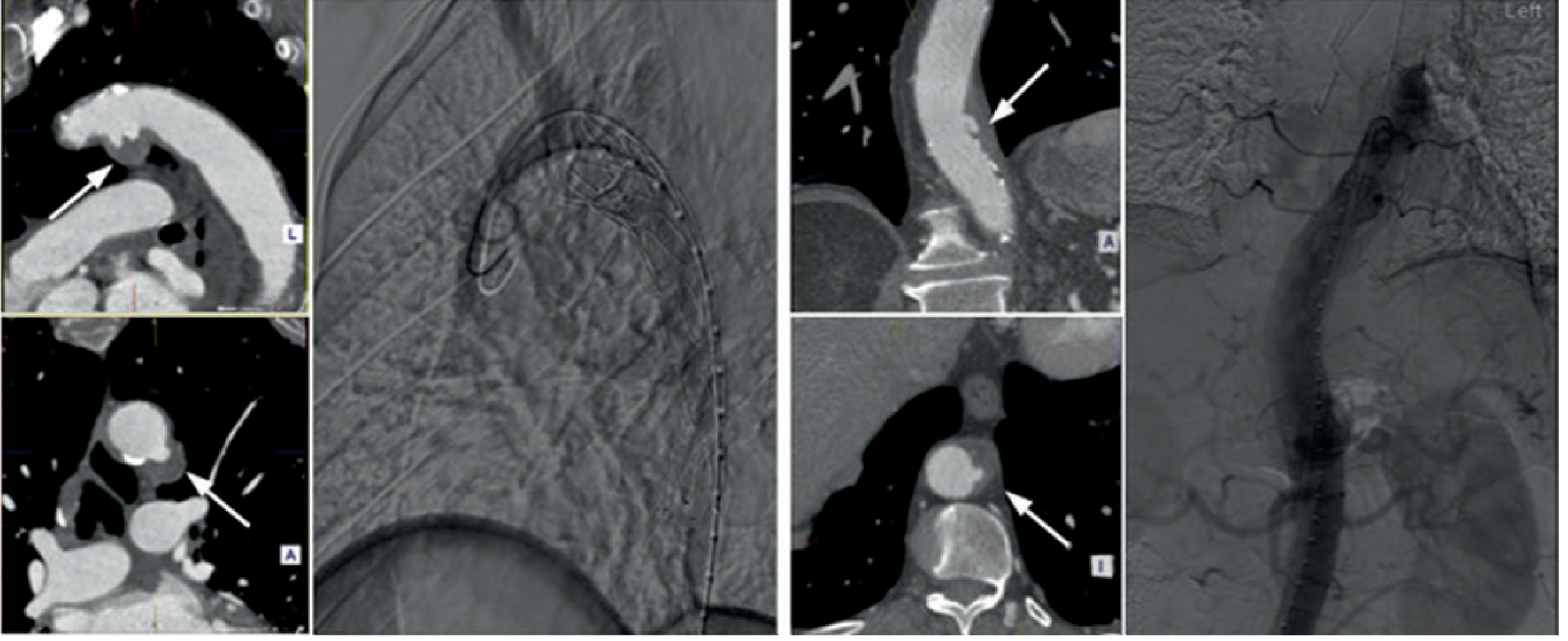
Fig. 79.16: PAU in the arch (left pair) and descending aorta (right pair)
AAS - Diagnostic Imaging
Chest X-ray:
- Normal CXR does NOT exclude AAS
- May show widened mediastinum, aortic knob abnormality, pleural effusion
- Useful to confirm alternative diagnosis in low-risk patients
CT Aortography (primary modality):
- Demonstrates dissection flap, true/false lumen, entry/re-entry tears
- Identifies complications: branch vessel occlusion, pericardial effusion, haemothorax
- Essential for treatment planning
Echocardiography (TTE/TOE):
- TOE: excellent for proximal aorta, intraoperative guidance
- Rapid, bedside - suited to unstable patients
- Can show IMH as crescentic wall thickening, dissection flap, pericardial effusion, AR
MRI:
- Best for IMH dating and characterisation
- Limited access in emergency
PART 2: BLUNT TRAUMATIC AORTIC INJURY (TAI)
Epidemiology
- Blunt aortic injury is the second most common cause of death from blunt trauma (after head injury)
- In USA: ~40,000 motor vehicle deaths/year; 20% caused by aortic rupture
- In UK: ~15% of road traffic accident fatalities involve thoracic aorta
- On arrival to hospital: only 25% of patients with blunt TAI are alive
- Prognosis of untreated survivors:
- 30% die within 6 hours
- 50% die within 24 hours
- 90% die within 4 months
- Miller's Anesthesia, p.7775; Grainger & Allison, p.2063
Mechanism of Injury
Primary mechanism - Sudden deceleration (most important):
- Especially at speeds >30 mph
- Rapid traction on the relatively immobile aortic isthmus (fixed by ligamentum arteriosum)
- Isthmus = distal to L. subclavian artery, proximal to 3rd intercostal artery
- Ligamentum arteriosum acts as a hinge for arch movement → maximum shearing force at isthmus
- 50-70% of traumatic ruptures occur at the isthmus
Secondary mechanisms:
- Torsion from heart displacement leftwards during AP compression (ascending aorta near innominate; from vertical falls >10 ft)
- "Osseous pinch" - compression between sternum and vertebral column (transverse force through full aortic wall thickness)
Distribution of injury sites:
- Isthmus: 50-70% (90% in some series)
- Ascending aorta / arch: 18%
- Distal thoracic aorta: 14%
Spectrum of injury (from intimal to full thickness):
- Subintimal haemorrhage (intimal tear only)
- IMH confined to media
- Traumatic dissection
- False aneurysm / pseudoaneurysm (laceration into adventitia - which is the only remaining intact layer)
- Complete transection → exsanguination at scene
In 80-90% there is complete aortic rupture with death at the scene. Survivors have partial-thickness injuries with at least the adventitia intact; periaortic haemorrhage is almost always present.
- Grainger & Allison, p.2063
CT Grading of TAI (Presley Trauma Center System)
| Grade | Subgrade | CT Findings |
|---|---|---|
| Grade I - Normal | Ia | Normal aorta; no mediastinal haematoma |
| Ib | Normal aorta; mediastinal (para-aortic) haematoma | |
| Grade II - Minimal | IIa | Small (<1 cm) pseudoaneurysm or intimal flap/thrombus; no mediastinal haematoma |
| IIb | Small (<1 cm) pseudoaneurysm or intimal flap/thrombus; with mediastinal haematoma | |
| Grade III - Confined | IIIa | >1-cm regular, well-defined pseudoaneurysm; no ascending/arch involvement |
| IIIb | >1-cm pseudoaneurysm; ascending/arch/great vessel involvement | |
| Grade IV - Total disruption | IV | Irregular, poorly defined pseudoaneurysm; mediastinal haematoma; intimal flap |
Modified from Gavant ML, Radiographics (1999)
Clinical Diagnosis
- Often difficult due to lack of specific symptoms (obtunded from head injury, confounding injuries)
- Symptoms when present: anterior chest pain, interscapular pain, dyspnoea, hoarseness (haematoma compression of recurrent laryngeal nerve), dysphagia
Imaging of TAI
Chest X-ray (initial screening)
- Sensitivity 80-90% for mediastinal haemorrhage - useful screening tool
- Signs of TAI on CXR:
- Widened superior mediastinum (M/C ratio >0.25 or >8 cm absolute)
- Deviation of trachea to the right of midline
- Widened right paratracheal stripe
- Loss / obscuring of aortic knuckle contour
- Displacement of nasogastric tube by haematoma (most specific indirect sign)
- Left pleural effusion / apical cap
- Important: Normal CXR does NOT exclude significant TAI
- Supine position makes mediastinal width interpretation unreliable, especially in obese patients
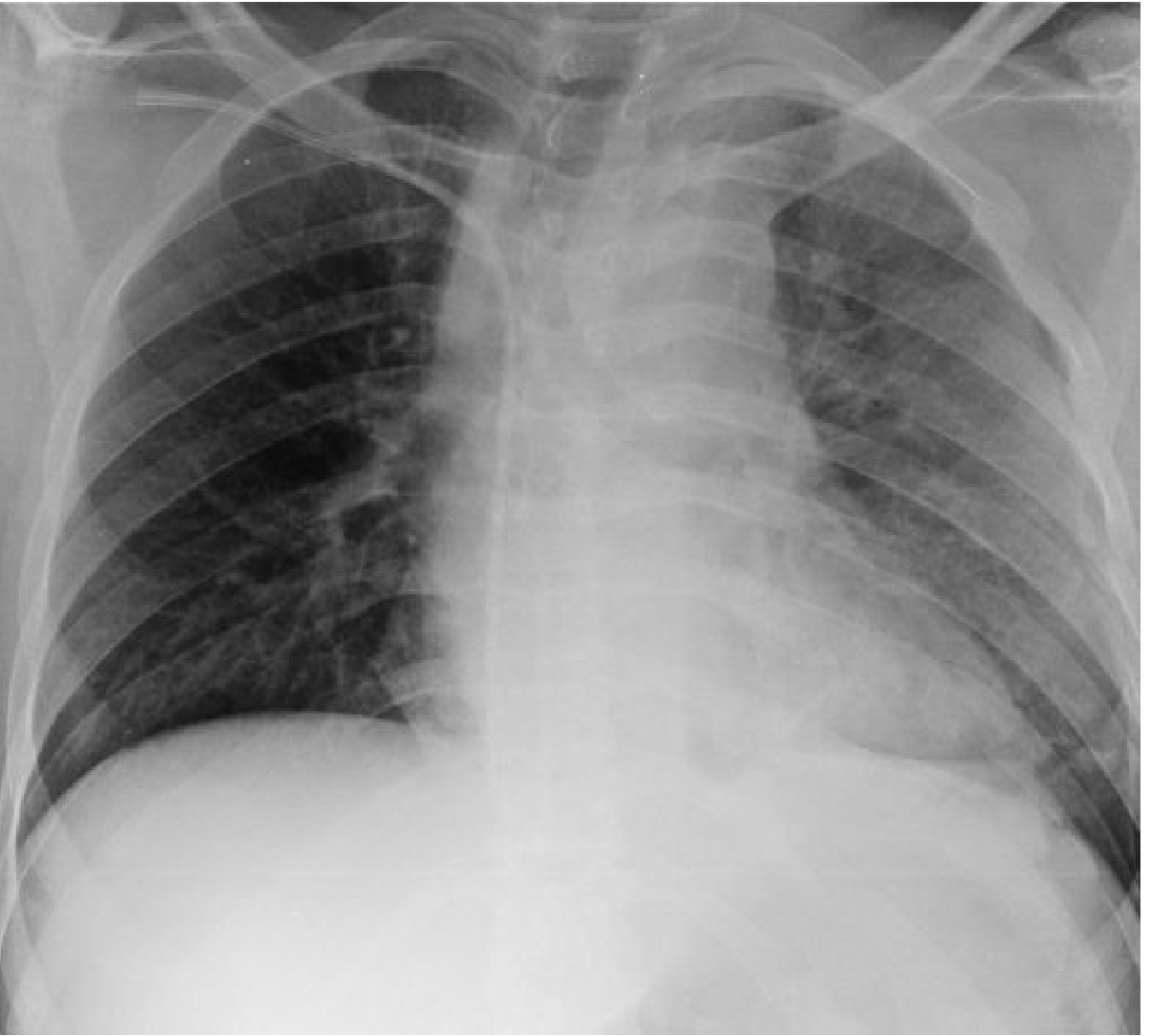
Fig. 17.20: CXR signs of TAI - widened mediastinum, deviated trachea, obscured aortic knuckle
CT Aortography (investigation of choice)
- Diagnostic accuracy approaches 100%
- First-line investigation in all patients stable enough to transfer
- Allows assessment of entire thorax, abdomen and head in single examination
- Direct CT signs of TAI:
- Contrast extravasation
- Defined pseudoaneurysm (most common finding)
- Dissection flap
- Focal aortic calibre change
- Small aortic contour abnormality (intimal/medial disruption)
- IMH
- Indirect signs:
- Periaortic mediastinal haematoma
- Haemothorax
- False positives: ductus diverticulum, severe atherosclerosis, double density from overlapping vessels, superior intercostal vein, bronchial artery infundibulum, motion artefacts
- Equivocal cases: IVUS can resolve (aortography adds little)
TOE (Trans-Oesophageal Echocardiography)
- Sensitivity 91%, specificity 98% for isthmic injuries
- Can be performed bedside in 15-20 minutes in unstable patients
- Identifies: intimal flap, mural thickening, periaortic blood
- Gap >7 mm between probe and aorta at proximal descending thoracic level + pleural blood = strongly suggests aortic disruption
- Contraindications: severe facial injuries, unstable cervical spine fractures
- Limitations: entire aortic circumference not visualised in ~30%; aortic arch poorly seen
- Role: screening in unstable patients; intraoperative guidance for stent-graft deployment
Aortography (largely historical)
- Sensitivity 84-96%; specificity imperfect
- Replaced by CT; no longer preferred; no additional benefit over CT
MRI
- Accuracy approaching 100%; can date IMH
- Limited by availability and time constraints in trauma settings
TAI CT + TEVAR Images
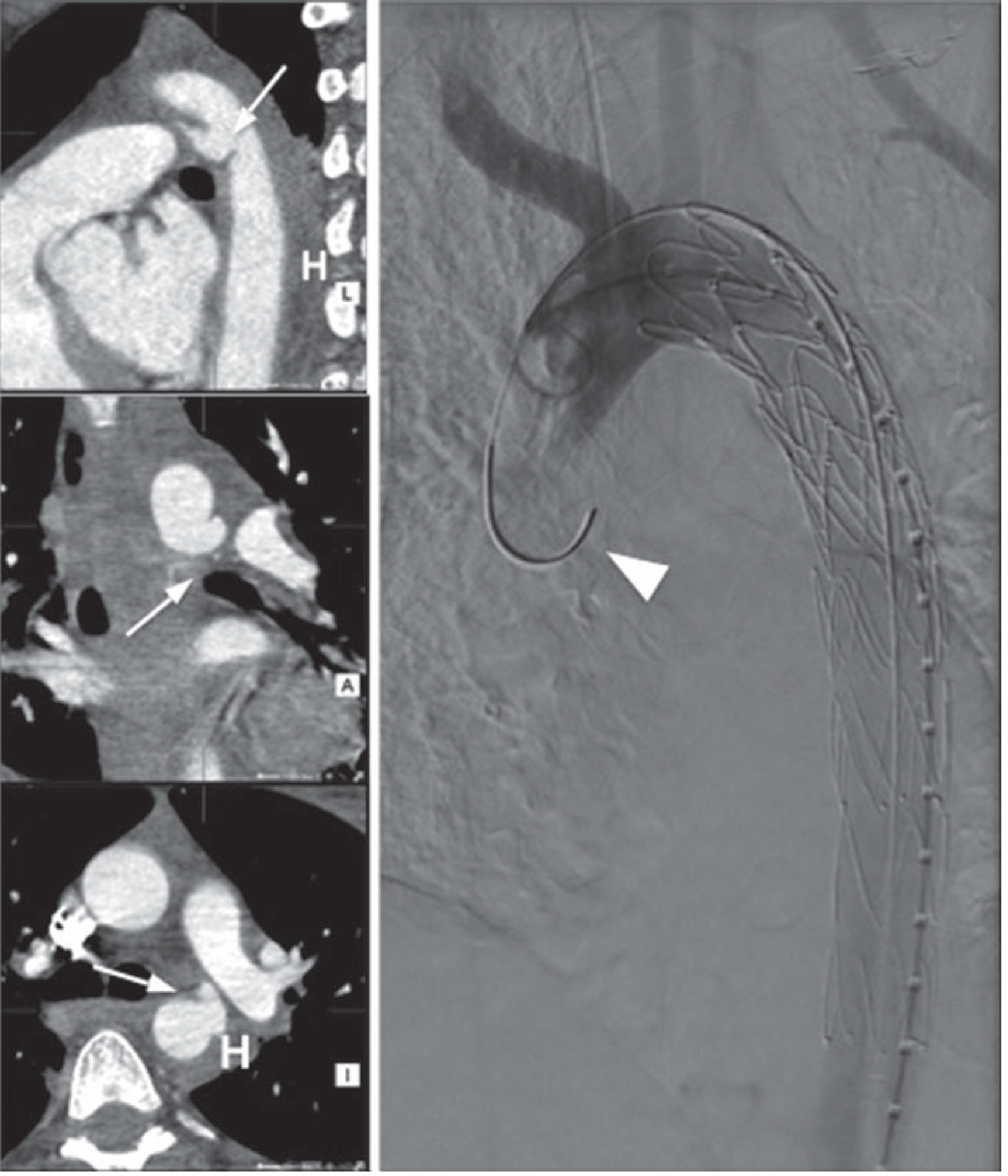
Fig. 79.20: CT diagnosis and TEVAR repair of blunt TAI at the isthmus
Management of TAI
Pre-operative / Initial Resuscitation
- ATLS principles - manage other life-threatening injuries first (TAI rarely requires immediate repair if the adventitia is intact)
- Aggressive blood pressure and heart rate control (mandatory to prevent complete rupture):
- Systolic BP <100 mmHg (Miller) / <120 mmHg (Grainger)
- HR <100 bpm
- β-Blockers (esmolol, labetalol) - reduce dP/dt (rate of pressure rise)
- IV nitroglycerin or sodium nitroprusside infusion
- Allow time to manage: haemorrhage, sepsis, hypothermia, coagulopathy, acidosis
- Controlled hypotension allows elective scheduling of definitive repair (days to weeks later)
Emergency TEVAR for TAI is now the exception, not the rule.
- Grainger & Allison, p.2063
Definitive Management
TEVAR (Thoracic Endovascular Aortic Repair) - Current Gold Standard:
- STS Class I recommendation; Level of Evidence B
- Preferred over open surgery whenever technically feasible
- Requires minimum 15 mm proximal landing zone (normal aorta) distal to last great vessel
- Left subclavian artery (LSA) frequently covered to extend landing zone:
- Most patients tolerate this (adequate collaterals via circle of Willis + left vertebral artery)
- Carotid-to-subclavian bypass not routinely required
- Risk of adverse central neurological events after LSA coverage without revascularisation: ~10%
TEVAR outcomes vs open surgery for TAI:
| Outcome | TEVAR | Open Surgery |
|---|---|---|
| Mortality | 7% | 15% |
| Paraplegia | 0% | 6% |
| Stroke | 1% | 5% |
| Technical success | Equal | Equal |
Grainger & Allison, p.2063
Open Surgical Repair:
- Ascending aorta or arch injuries: CPB ± DHCA required
- Descending thoracic aorta: Open repair of short segment; partial left heart bypass (PLHB) for spinal cord and visceral protection without full heparinisation
- Reserved for cases not amenable to TEVAR or endovascular failure
Anaesthetic / Intraoperative Considerations (Miller's Anesthesia)
- Full stomach precautions
- Monitoring: arterial line, CVP, large-bore IV access
- TEE for intraoperative guidance
- Avoid wide swings in BP during induction and laryngoscopy - prepare esmolol and nitroglycerin in advance
- Controlled postoperative ventilation with ICU transfer
Associated Injuries to Consider
Given the mechanism of injury (high-velocity deceleration), always evaluate:
- Head injury (CT head)
- Pneumothorax / haemothorax
- Pulmonary contusion
- Rib fractures, flail chest
- Cardiac contusion (ECG, troponin)
- Diaphragmatic injury
- Intra-abdominal solid organ injury
SUMMARY TABLE: AAS vs Blunt TAI
| Feature | AAS (Dissection/IMH/PAU) | Blunt TAI |
|---|---|---|
| Cause | Hypertension, connective tissue disease, atherosclerosis | High-velocity trauma (MVA, falls) |
| Site | Type A: ascending ± arch; Type B: descending | Aortic isthmus (50-70%) |
| Mechanism | Shear stress on intima; vasa vasorum haemorrhage | Sudden deceleration; torsion; osseous pinch |
| Imaging (1st line) | CT Aortography | CT Aortography |
| Bedside test | TOE | TOE (if unstable) |
| Initial medical Rx | β-blockers + nitrates; HR <60, sBP <120 | β-blockers + nitrates; sBP <100, HR <100 |
| Definitive Rx (Type A/ascending) | Emergency open surgery (CPB ± DHCA) | Emergency surgery (CPB ± DHCA) |
| Definitive Rx (Type B/descending) | TEVAR or medical (INSTEAD trial) | TEVAR (elective scheduling) |
| Surgical mortality | Type A: ~17%; Type B (TEVAR): ~4% | TEVAR ~7%; Open ~15% |
| Paraplegia risk (TEVAR) | Low (<1%) | ~0% |
KEY SUMMARY BOX: Acute Aortic Syndrome
Aortic dissection - intimal disruption allowing blood to track through medial dissection plane
Intramural haematoma - intramural haemorrhage from vasa vasorum or bleeding at base of PAU (similar appearance to thrombosed false lumen)
Penetrating aortic ulcer - ulcerating atherosclerotic lesion penetrating into the media
Diagnosis is usually by cross-sectional imaging. Three-quarters of AAS is dissection; 10-20% is IMH; small proportion is PAU. Dissection involves ascending aorta and arch in three-quarters of cases. IMH more commonly involves descending thoracic aorta. PAU usually in markedly atheromatous segments (descending thoracic aorta).
- Grainger & Allison, p.2061
Sources:
- Grainger & Allison's Diagnostic Radiology, Chapters 17 and 79 (pp. 431-432, 443, 2061-2063)
- Miller's Anesthesia 10e, Chapter (pp. 7774-7777)
- Braunwald's Heart Disease (pp. 841-845, 3469-3472)
This is a shared conversation. Sign in to Orris to start your own chat.