ECG
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching Images
ECG waveform interpretation P QRS T wave
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need for a comprehensive guide. Here is a complete, systematic approach to ECG interpretation.
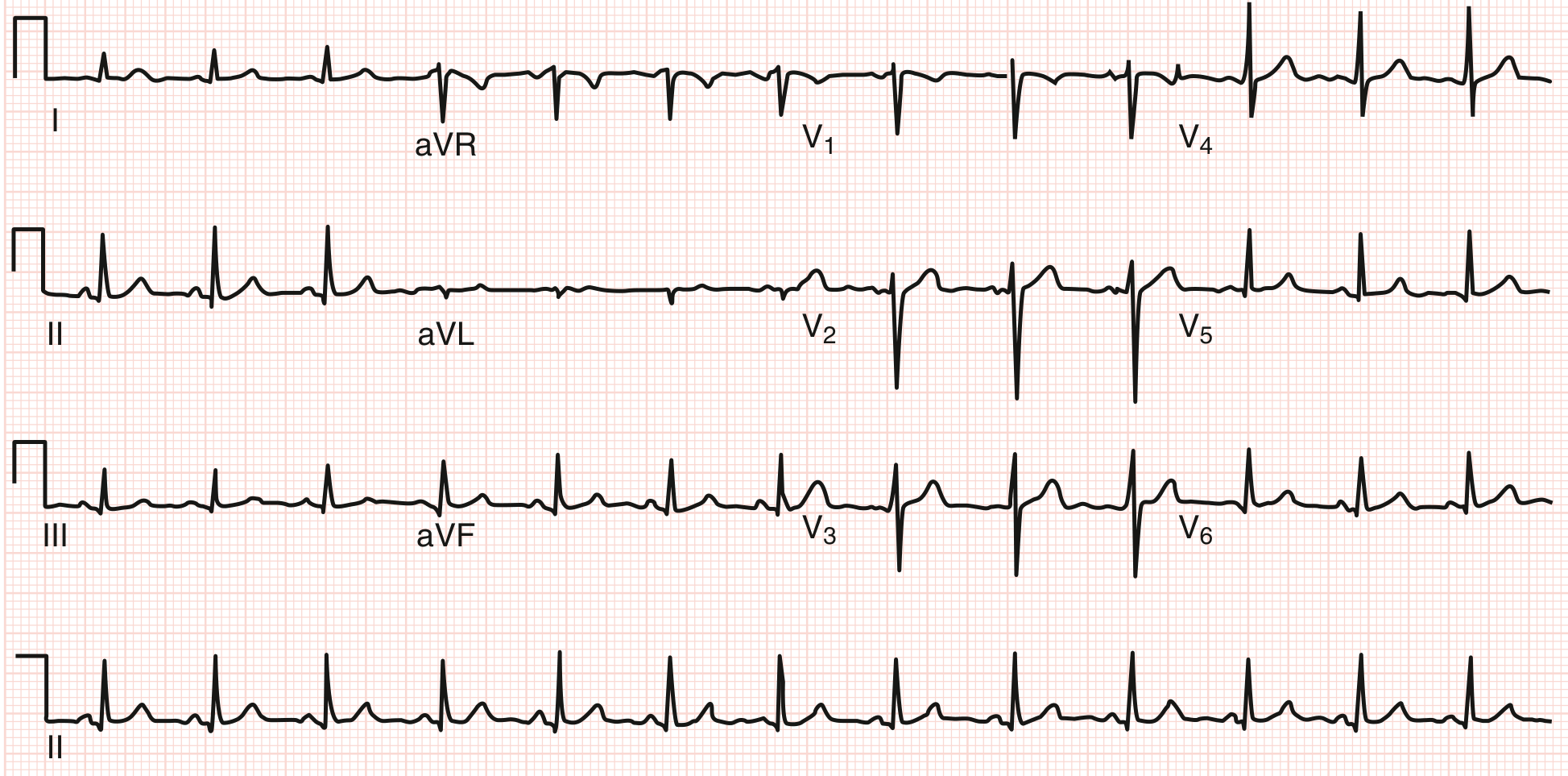
How to Read an ECG: A Systematic Approach
A standard 12-lead ECG records 10 seconds of cardiac electrical activity at a paper speed of 25 mm/sec. Each small box = 0.04 sec (40 ms), each large box = 0.2 sec (200 ms). Voltage is 10 mm = 1 mV at standard calibration. Always use a stepwise approach — most errors are errors of omission.
The 12 Leads at a Glance
| Lead Group | Leads | Anatomic View |
|---|---|---|
| Inferior | II, III, aVF | Inferior wall (RCA territory) |
| Lateral | I, aVL, V5, V6 | Lateral wall (LCx territory) |
| Anterior/Septal | V1–V4 | Anterior wall (LAD territory) |
| Right-facing | aVR | Right side (always inverted in normal) |
Step 1 — Rate
Formula: HR = 60,000 ÷ RR interval (in ms)
Quick method (regular rhythm): Count large boxes between two R waves → divide 300 by that number.
- 1 box = 300 bpm, 2 = 150, 3 = 100, 4 = 75, 5 = 60, 6 = 50
Normal resting rate: 50–100 bpm (physiologic range 50–90 bpm)
Step 2 — Rhythm
- Is it regular or irregular? (Compare R–R intervals)
- Are P waves present? Is every P followed by a QRS?
- What is the P wave axis? (Upright in II, inverted in aVR = sinus origin)
- Are there premature beats or pauses?
Normal sinus rhythm = regular rhythm, upright P in II, P before every QRS, rate 60–100 bpm.
Step 3 — Intervals
Normal ECG Intervals (Goldman-Cecil Medicine, Table 42-1)
| Parameter | Normal Range |
|---|---|
| Heart rate | 50–100 bpm |
| P wave duration | < 120 ms (< 3 small boxes) |
| PR interval | 90–200 ms (2.25–5 small boxes) |
| QRS duration | 75–110 ms (< 3 small boxes) |
| QTc (males) | 390–450 ms |
| QTc (females) | 390–460 ms |
| QRS axis | −30° to +90° |
PR interval: onset of P → onset of QRS. Prolonged (>200 ms) = 1st degree AV block. Short with delta wave = WPW preexcitation.
QRS duration: Prolonged >110 ms = intraventricular conduction delay; ≥120 ms = bundle branch block.
QT/QTc: Measure Q onset → T wave end. Correct using Bazett's formula: QTc = QT ÷ √RR. Prolonged QTc raises risk of torsades de pointes.
Step 4 — Axis
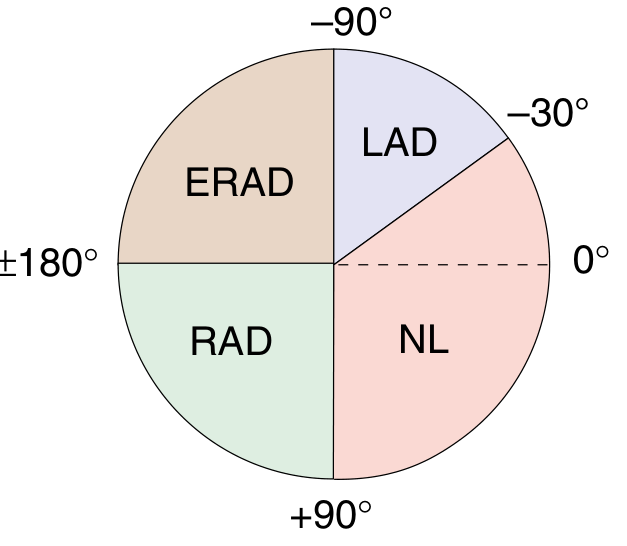
| Axis | Degrees | Causes |
|---|---|---|
| Normal (NL) | −30° to +90° | — |
| Left axis deviation (LAD) | −30° to −90° | LBBB, LAFB, inferior MI |
| Right axis deviation (RAD) | +90° to +180° | RVH, RBBB, lateral MI, normal variant in young |
| Extreme RAD (ERAD) | −90° to ±180° | Severe pathology |
Quick axis check: If QRS is positive in both Lead I and Lead II → normal axis. If positive I, negative II → LAD. If negative I, positive II → RAD.
Step 5 — P Waves
- Normal: Upright in I, II, aVF, V4–V6; inverted in aVR; biphasic in V1
- Duration < 120 ms; amplitude < 2.5 mm in II
- Broad, notched P (P mitrale) → left atrial enlargement
- Tall, peaked P (P pulmonale, >2.5 mm in II) → right atrial enlargement
- Absent P waves → AF, junctional rhythm, hyperkalemia
Step 6 — QRS Morphology
Naming convention:
- Capital letters (Q, R, S) = amplitude ≥ 5 mm
- Lowercase (q, r, s) = amplitude < 5 mm
- QS = entirely negative deflection
R-wave progression (precordial leads V1→V6):
- V1: small r, deep S (rS pattern)
- V3–V4: transition zone — R amplitude begins to exceed S
- V6: large R, small or no S
- Poor R-wave progression (transition delayed to V5/V6) suggests anterior MI or RVH
Pathological Q waves:
- Width > 40 ms (1 small box) OR depth > 25% of the R wave in the same lead
- Present in a regional distribution → prior transmural infarction
- Septal q waves in V5–V6 and small q in inferior leads = normal variant
Step 7 — ST Segments
Measured from the J point (where QRS meets ST segment) to the onset of the T wave.
| Finding | Significance |
|---|---|
| ST elevation ≥ 1 mm (limb leads) or ≥ 2 mm (precordial) in ≥ 2 contiguous leads | STEMI, pericarditis (diffuse saddle-shaped elevation), early repolarization |
| ST depression ≥ 1 mm | NSTEMI/UA, posterior MI (V1–V3), digoxin effect (scooped), strain |
| Diffuse saddle-shaped ST elevation + PR depression | Pericarditis |
Step 8 — T Waves
- Normal: Upright in I, II, V3–V6; inverted in aVR; variable in III and V1
- Peaked, symmetric T waves → hyperkalemia, hyperacute STEMI
- Deep, symmetric T wave inversions → ischemia, Wellens syndrome (V2–V3)
- Asymmetric inversions → right/left ventricular strain, normal variant in lateral leads
Step 9 — U Waves
- Small deflection after the T wave, best seen in V2–V3
- Prominent U waves → hypokalemia, bradycardia, drug effects (quinidine, amiodarone)
- Inverted U waves → may indicate ischemia or LV volume overload
The Harrison's 14-Point Checklist (complete systematic read)
- Standardization and technical features (calibration, lead placement, artifacts)
- Rhythm
- Heart rate
- PR interval / AV conduction
- QRS interval
- QT / QTc
- Mean QRS electrical axis
- P waves
- QRS voltages
- Precordial R-wave progression
- Abnormal Q waves
- ST segments
- T waves
- U waves
Always compare with prior ECGs — this is invaluable. — Harrison's Principles of Internal Medicine, 22E
Common Patterns to Recognize
| Pattern | Key Features |
|---|---|
| STEMI | ST elevation in ≥2 contiguous leads, reciprocal ST depression |
| LBBB | QRS ≥120 ms, broad notched R in I/V6, QS in V1 |
| RBBB | QRS ≥120 ms, rSR' (bunny ear) in V1, wide S in I/V6 |
| 1st° AV block | PR >200 ms, 1:1 P:QRS |
| 2nd° AV block (Mobitz I) | Progressive PR lengthening → dropped QRS |
| 2nd° AV block (Mobitz II) | Fixed PR, sudden dropped QRS |
| 3rd° AV block | P waves & QRS completely dissociated |
| Atrial fibrillation | Irregularly irregular, absent P waves, fibrillatory baseline |
| Atrial flutter | Sawtooth flutter waves ~300 bpm, regular ventricular response |
| WPW | Short PR, delta wave, wide QRS |
| Hyperkalemia | Peaked T → widened QRS → sine wave |
| Hypokalemia | Flattened T, prominent U waves |
Sources: Goldman-Cecil Medicine (International Ed.), Table 42-1/42-2; Harrison's Principles of Internal Medicine 22E, Chapter 247
This is a shared conversation. Sign in to Orris to start your own chat.