Pilonidal sinus
Reading File
Finding Sources
Searching PubMed
"pilonidal sinus" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have excellent, comprehensive content from multiple authoritative surgical textbooks plus clinical images. Let me compile the full answer.
Pilonidal Sinus
Definition
A pilonidal sinus is a condition found in the natal cleft overlying the coccyx, consisting of one or more midline openings communicating with a fibrous track lined by granulation tissue and containing loosely lying hair within the lumen. The name comes from Latin: pilus (hair) + nidus (nest).
- Bailey and Love's Short Practice of Surgery, p. 1444
- Sabiston Textbook of Surgery, p. 2170
Epidemiology
- Affects approximately 70,000 patients annually in the United States
- Typically presents in young adults in their mid-to-late 20s
- Much more common in men than women (men tend to be more hirsute)
- More prevalent in white individuals; rare in Black or Asian patients
- Associated with: obesity, sedentary occupation, local trauma/irritation, dark coarse hair
- Age of onset: after puberty, before the fourth decade
- Can occasionally occur in barbers/hairdressers (interdigital pilonidal sinus - an occupational disease)
Aetiology & Pathogenesis
Two theories have been proposed:
1. Congenital theory (largely discredited): epidermal rests with hair embedded below the dermis in the midline from failure of fusion.
2. Acquired theory (now favoured): Evidence supporting acquired origin includes:
- Interdigital pilonidal sinus is an occupational disease of hairdressers
- Age of appearance is older than expected for a congenital lesion
- Hair follicles are rarely present in the walls of the sinus
- Pointed hair ends are directed towards the blind end of the sinus
- Recurrence is common even after adequate excision
The mechanism: shed hair collects in the natal cleft. Buttock friction and shearing forces, combined with a vacuum/suction effect from buttock movement, drill loose hair through the midline skin via small sebaceous or hair follicles. Infection in relation to a hair follicle allows further hair entry. The foreign body reaction from trapped hair leads to local inflammation, which may become superinfected forming a hair-filled abscess cavity.
- Fischer's Mastery of Surgery, p. 4292
- Bailey and Love's, p. 1444
Clinical Features

Hallmark finding: one or more pits strictly in the midline between the sacrococcygeal joint and the tip of the coccyx, with sinus openings.
Presentations:
- Asymptomatic - incidental midline pits without inflammation (no treatment required)
- Chronic/intermittent - pain, swelling, and discharge at the base of the spine; history of repeated abscesses that have burst or been incised; usually away from midline; broken hairs visible exuding from midline pits
- Acute abscess - hot, tender, fluctuant swelling lateral to midline over the sacrum; may exude pus through midline pit or spontaneously discharge
Course of sinus tracts: Most sinuses run cephalad. Secondary tracks may spread laterally, emerging as granulation tissue-lined discharging openings. The location is distinctly different from a perirectal abscess (which is near the anus).
Differential Diagnosis
If no primary pits are seen, or if the sinus drains lateral to the sacrum or appears caudal to the primary pits, consider:
- Hidradenitis suppurativa (HS)
- Complex anal fistula
- Osteomyelitis with draining skin sinuses
- Tuberculosis or actinomycosis
- Perianal Crohn disease
Histopathology
Excisional specimens reveal:
- Sinus tract extending into the dermis and subcutaneous tissue
- Surrounded by chronic inflammation and foreign body granuloma
- Tufts of hair found in sinuses in three-quarters of cases
- Granulation tissue and fibrosis within the cyst/track walls
- Hair follicles are rarely found in the actual sinus walls (distinguishing acquired from congenital origin)
Carcinoma arising in chronic pilonidal disease is exceedingly rare but described.
- Dermatology 2-Volume Set 5e, p. 2836
Bacteriology
Bacterial colonisation ranges from 50% to 70%. Typical isolates:
- Staphylococcus aureus
- Anaerobes such as Bacteroides
Treatment
Treatment is tailored to the severity and stage of disease.
1. Conservative (Minimal Disease)
- Regular hair removal from the natal cleft: trimming, shaving, waxing, or laser depilation - shown to decrease recurrence rates
- Strict hygiene and exfoliation
- Silver nitrate or laser cauterisation of tracks for less complex disease
2. Acute Abscess
- Incision and drainage (I&D) in the emergency room - the only treatment needed acutely
- Off-midline incision over the most fluctuant portion (lateral to the midline wherever possible) - this facilitates wound healing
- Thorough curettage removing all embedded hair and devitalized tissue
- Antibiotics as adjunct (given bacterial colonisation rates)
3. Chronic / Recurrent Disease (Surgical Options)
There is no single universally superior technique. Choice depends on recurrence rates, time off work, and surgeon preference:
| Procedure | Principle | Notes |
|---|---|---|
| Lay open (unroofing) ± marsupialisation | Wide excision left open | Slower healing, lower recurrence |
| Wide excision + primary closure (midline) | Complete excision, closed | Faster healing, higher recurrence |
| Gips procedure (pit-picking) | Excision of pits + curettage of sinus, minimally invasive | Less invasive option |
| Karydakis procedure | Off-midline incision around sinus; contralateral flap mobilized for tension-free off-midline closure | Lower recurrence than midline closure |
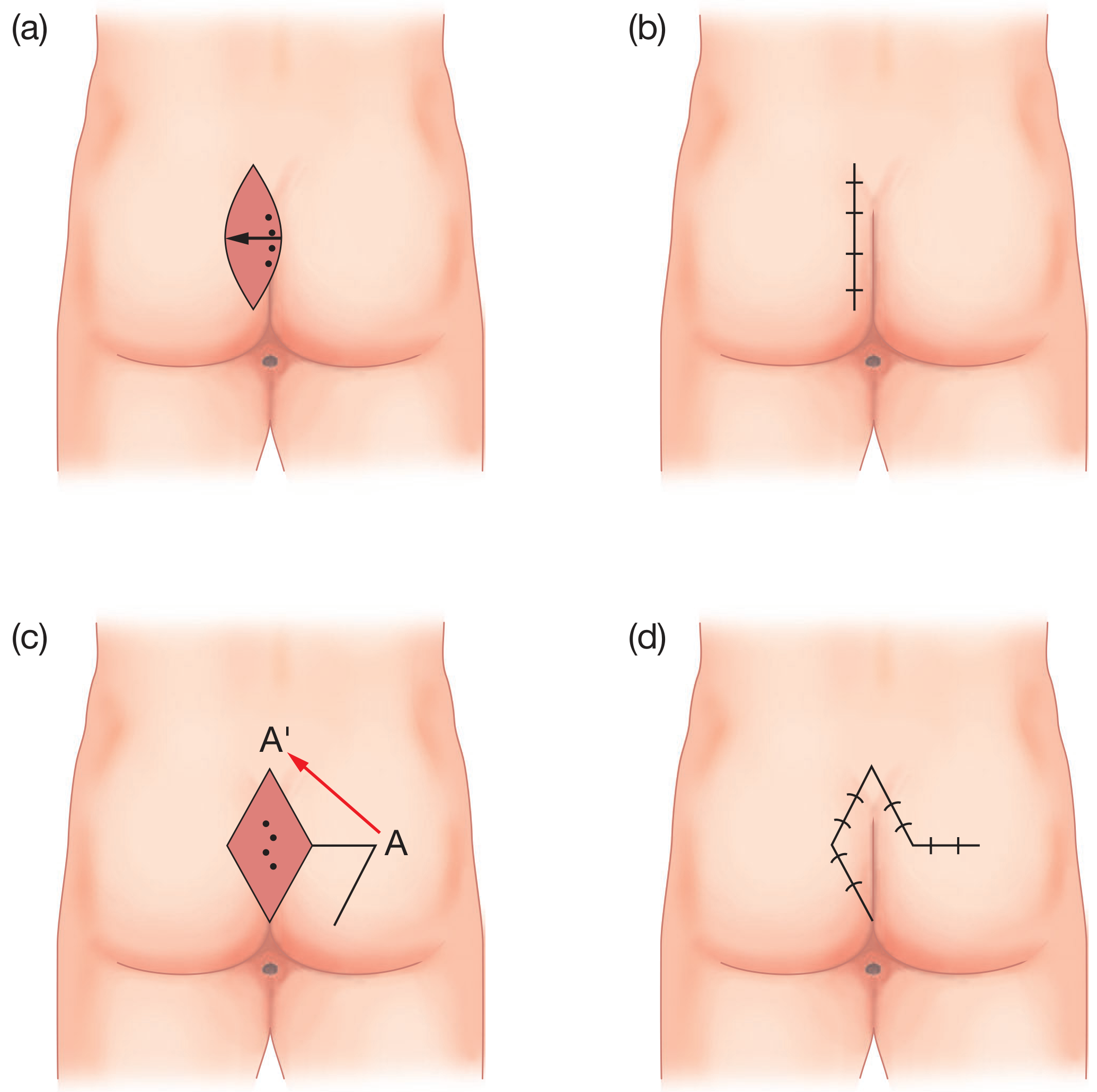
| Limberg (rhomboid) flap | Rhomboid excision + rotation flap | Off-midline closure; good outcomes |
| Bascom's procedure | Lateral incision to clear cavity, excision/closure of midline pits; lateral wound heals secondarily | Preserves natal cleft |
| Bascom cleft lift | Eccentric ellipse excision flattening the natal cleft; staple line out of cleft | For failure/recurrence; flattens the cleft |
| Z-plasty | Excision + Z-shaped flap closure | Off-midline closure |
| EPSiT/SiLaC (endoscopic/laser) | Minimally invasive endoscopic or laser ablation | Growing evidence base, especially in paediatrics |
Key principles of wound healing:
- Open healing = lower recurrence, but slower healing time
- Off-midline primary closure = lower recurrence AND faster healing vs. midline closure
- Post-operative hair removal from the wound is the cornerstone of aftercare
Surgical Technique Illustrations
Recent Evidence (2023-2026)
Recent systematic reviews and meta-analyses update the surgical evidence:
- A 2023 systematic review/meta-analysis (Wu et al., PMID 37158142) reviewed surgical treatment progress for sacrococcygeal pilonidal sinus, comparing techniques.
- A 2024 meta-analysis (Gan et al., PMID 37419810) compared phenol treatment vs surgical excision, finding phenol to be a viable minimally invasive option.
- A 2024 meta-analysis (Xie et al., PMID 38776547) confirmed the efficacy of laser treatment (SiLaC) in pilonidal disease with acceptable recurrence rates.
- A 2024 systematic review (Mentessidou et al., PMID 37494954) supported endoscopic pilonidal sinus treatment (EPSiT) as safe and effective in the paediatric population.
Special Note: Interdigital Pilonidal Sinus
An occupational variant seen in barbers, hairdressers, and dog groomers. Short hairs penetrate interdigital web spaces of the hands (or feet when wearing sandals). Causes a foreign body granuloma. Usually self-limited but may require surgical excision if repeatedly infected. Histologically: an epidermis-lined sinus tract containing one or several hairs with a deeper foreign body reaction.
- Dermatology 2-Volume Set 5e, p. 2834
This is a shared conversation. Sign in to Orris to start your own chat.