Cardiovascular system examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Now I have everything I need for a thorough, well-organized answer. Let me compose it.
Cardiovascular System Examination
A systematic cardiovascular exam proceeds through general inspection → vital signs → jugular venous pressure → arterial pulse → precordial examination → auscultation. Each step provides distinct hemodynamic information that cannot be replaced by technology alone.
1. General Inspection
Look for signs that suggest underlying cardiac disease before touching the patient:
- Dyspnoea at rest, orthopnoea - raised JVP, left heart failure
- Malar flush - mitral stenosis
- Cyanosis - central (lips, tongue) vs. peripheral (fingertips)
- Clubbing - congenital cyanotic heart disease, infective endocarditis
- Splinter haemorrhages, Osler nodes, Janeway lesions - infective endocarditis
- Xanthelasma / corneal arcus - hyperlipidaemia
- Marfanoid habitus - aortic root dilatation, mitral valve prolapse
- Raised BMI, cushingoid features - hypertension risk
2. Blood Pressure
Accurate measurement requires: seated position, arm at heart level, feet flat, 5-10 min rest, appropriately sized cuff (bladder length 80%, width 40% of arm circumference). Inflate 30 mmHg above expected systolic; release at 2-3 mmHg/s. Systolic = first Korotkoff sound (K1); diastolic = disappearance (K5).
Common errors: using a small cuff overestimates BP; a large cuff underestimates it.
Measure both arms. A difference >15 mmHg between arms suggests subclavian stenosis or aortic dissection.
Special patterns:
| Pattern | Significance |
|---|---|
| Wide pulse pressure | Chronic severe AR, hyperthyroidism, anaemia |
| Narrow pulse pressure | Severe AS, tamponade, severe LV dysfunction |
| Orthostatic drop (>20/10 mmHg) | Volume depletion, autonomic neuropathy |
3. Jugular Venous Pressure (JVP)
The JVP is the single most important bedside measurement for estimating volume status. The internal jugular vein is preferred (directly in line with SVC and right atrium; the external jugular is valved).
Technique: Position patient at 30-45°; identify the double waveform of the internal jugular. Measure the vertical distance from the sternal angle (angle of Louis) to the top of the pulsation. A distance >4.5 cm at 30° is abnormal. Note: bedside estimates are in cmH₂O - convert to mmHg (1.36 cmH₂O = 1 mmHg).
When elevated JVP is suspected, sit the patient upright with legs dangling - venous pulsation above the clavicle in this position is clearly abnormal.
JVP vs. Carotid:
| Feature | JVP | Carotid |
|---|---|---|
| Waveform | Biphasic (sinus rhythm) | Monophasic |
| Compressible | Yes (obliterated by pressure) | No |
| Varies with posture/inspiration | Yes | No |
JVP Waveform Components
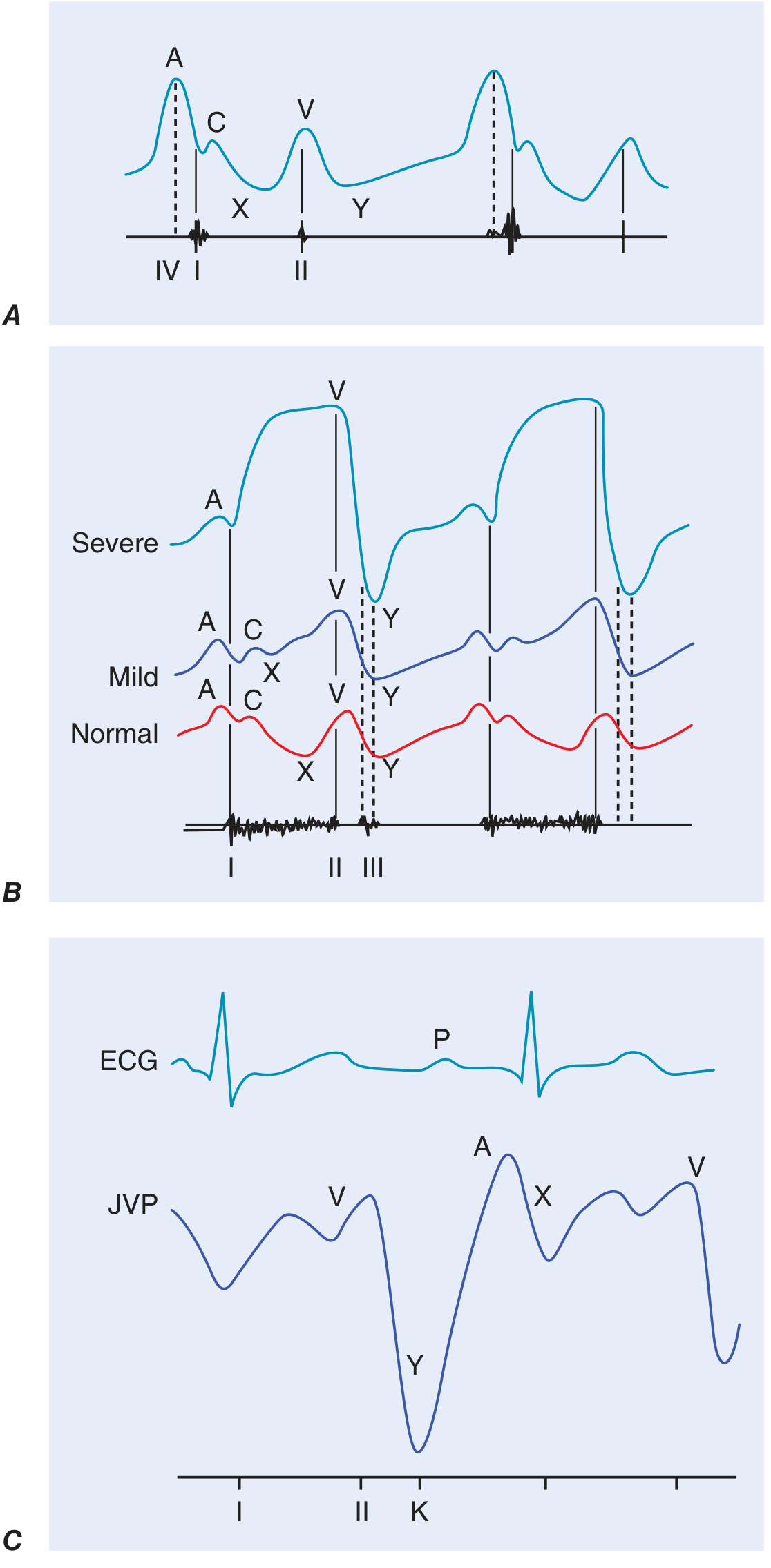
| Wave/Descent | Timing | Mechanism | Abnormality |
|---|---|---|---|
| a wave | Pre-systole (after P wave, before S1) | Right atrial contraction | Prominent in reduced RV compliance (PS, pulmonary HTN); absent in AF |
| c wave | Early systole | Tricuspid valve pushed into RA during RV contraction | Usually not visible clinically |
| x descent | Systole | RA relaxation + tricuspid valve moves toward RV apex | Attenuated/abolished in tricuspid regurgitation |
| v wave | Late systole | RA filling while tricuspid valve is closed | Giant v wave in tricuspid regurgitation |
| y descent | Early diastole | Tricuspid valve opens; RA empties | Rapid/sharp y descent in constrictive pericarditis (+ pericardial knock) |
Cannon a waves (giant a waves) - seen when RA contracts against a closed tricuspid valve - hallmark of AV dissociation (ventricular tachycardia, complete heart block).
Kussmaul's sign - paradoxical rise (or failure to fall) of JVP on inspiration - seen in constrictive pericarditis, restrictive cardiomyopathy, right heart failure.
Abdominojugular reflux (hepatojugular reflux) - sustained JVP rise >3 cm with 10 s of firm abdominal pressure - positive in elevated right or left heart filling pressures.
An elevated JVP (RA pressure >10 mmHg) has an 88% positive predictive value for a pulmonary artery wedge pressure >22 mmHg, and carries independent prognostic significance in heart failure.
4. Arterial Pulse
Assess the radial pulse first (rate, rhythm, volume, character), then the carotid for character/waveform (never compress both simultaneously), then peripheral pulses systematically.
Rate: Normal 60-100 bpm. Bradycardia <60; tachycardia >100.
Rhythm: Regular vs. irregularly irregular (AF) vs. regularly irregular (2nd-degree AV block, bigeminy).
Pulse character (best felt at the carotid):
| Pulse | Character | Causes |
|---|---|---|
| Normal | Smooth upstroke, single peak | - |
| Pulsus parvus et tardus (small/slow rising) | Weak, delayed, prolonged upstroke; anacrotie notch may be felt | Severe aortic stenosis |
| Collapsing (Corrigan's / water-hammer) | Sharp rise, rapid collapse | Chronic severe AR, PDA, hyperdynamic states |
| Bisferiens | Two systolic peaks | Severe AR (±AS), HOCM |
| Pulsus paradoxus | Systolic BP falls >10 mmHg on inspiration | Cardiac tamponade, massive PE, severe obstructive lung disease |
| Pulsus alternans | Beat-to-beat variation in amplitude, regular rhythm | Severe LV systolic dysfunction |
Pulsus paradoxus measurement: inflate cuff above systolic; lower slowly; note the pressure at which Korotkoff sounds first appear (expiration only) and the pressure at which they are heard throughout the cycle. Difference >10 mmHg = positive.
5. Precordial Examination
Inspection
- Visible apex beat - hyperdynamic states, LV enlargement
- Visible pulsations - right parasternal (RV hypertrophy or ascending aortic aneurysm), pulmonary area (pulmonary HTN)
- Chest wall deformities - pectus excavatum, scoliosis
Palpation
Apex beat:
- Normal location: 5th intercostal space, midclavicular line
- Displaced laterally and/or inferiorly - LV dilation
- Hyperdynamic/thrusting - volume overload (AR, MR, VSD)
- Heaving/sustained - pressure overload (AS, hypertension)
- Tapping - palpable S1 in mitral stenosis
- Double impulse - HOCM (palpable S4)
Right ventricular heave (parasternal lift): left parasternal area lifts the palm - RV hypertrophy or RV volume overload.
Thrills: palpable murmurs (grade ≥4/6). Systolic thrill at the right upper sternal border = AS or sub-AS; thrill at the left lower sternal border = VSD; apical systolic thrill = MR.
Palpable heart sounds:
- Palpable P2 at pulmonary area = pulmonary hypertension
- Palpable S4 at apex = reduced LV compliance
6. Auscultation
Position the patient supine initially; roll to left lateral decubitus for mitral sounds; sit forward, exhale for aortic sounds. Use the diaphragm (high frequencies) and bell lightly applied (low frequencies - S3, S4, MS rumble).
Auscultate in sequence: aortic area (2nd right ICS), pulmonary area (2nd left ICS), tricuspid area (lower left sternal border), mitral area (apex).
Heart Sounds
S1 (first heart sound)
- Closure of mitral (M1) then tricuspid (T1) valves
- Loud S1: tachycardia, mitral stenosis (pliable valve), short PR interval, hyperdynamic states
- Soft S1: long PR interval, severe MR, calcified immobile mitral valve, poor LV function
- Variable S1: AF (variable RR), complete heart block (PR changes)
S2 (second heart sound)
- Closure of aortic (A2) then pulmonary (P2) valves
- Physiological splitting: increases on inspiration (delayed P2 as RV stroke volume increases)
- Wide fixed splitting: ASD (fixed), RBBB (delayed P2), pulmonary stenosis
- Wide splitting with respiratory variation: RBBB, RV failure
- Paradoxical (reversed) splitting: A2 delayed, splits on expiration - LBBB, severe AS, HOCM
- Loud P2: pulmonary hypertension
- Soft A2: severe AS
S3 (third heart sound / ventricular gallop)
- Low-pitched; heard with bell at apex (left-sided) or LLSB (right-sided)
- Timing: early diastole, just after S2 - rapid filling phase
- Pathological in adults - indicates elevated filling pressures, reduced LV compliance; seen in HF, dilated cardiomyopathy, MR, VSD
- Physiological in children, young adults, pregnancy, athletes
S4 (fourth heart sound / atrial gallop)
- Low-pitched; heard just before S1
- Produced by atrial contraction into a stiff, non-compliant ventricle
- Seen in: LVH (hypertension, HCM, AS), ischaemia, acute MI
- Never heard in AF (no organized atrial contraction)
Additional sounds:
| Sound | Timing | Cause |
|---|---|---|
| Ejection click | Early systole, just after S1 | Bicuspid aortic valve (aortic EC), pulmonary stenosis (pulmonary EC, decreases on inspiration) |
| Mid-systolic click | Mid-late systole | Mitral valve prolapse (moves earlier on standing) |
| Opening snap (OS) | Early diastole, after S2 | Mitral stenosis (pliable valve). Short A2-OS interval = more severe MS |
| Pericardial knock | Early diastole | Constrictive pericarditis (coincides with rapid y descent of JVP) |
| Pericardial rub | Systolic + diastolic (three-component) | Pericarditis (best heard leaning forward, end-expiration) |
| Prosthetic valve sounds | Metallic opening/closing clicks | Mechanical prostheses |
Murmurs
Characterise each murmur by: timing - location - radiation - intensity (Levine grade) - quality - pitch - response to manoeuvres.
Levine grading:
| Grade | Description |
|---|---|
| 1/6 | Heard only with special effort |
| 2/6 | Soft but heard immediately |
| 3/6 | Moderately loud, no thrill |
| 4/6 | Loud + thrill |
| 5/6 | Heard with stethoscope barely on chest |
| 6/6 | Heard without stethoscope |
Systolic Murmurs
| Murmur | Timing | Location/Radiation | Quality | Key Features |
|---|---|---|---|---|
| Aortic stenosis | Ejection (mid-systolic) | RUSB → carotid | Harsh, crescendo-decrescendo | Soft/absent A2; slow-rising pulse; Gallavardin phenomenon (musical quality at apex) |
| HOCM | Ejection (mid-systolic) | LLSB (no carotid radiation) | Harsh | Increases with Valsalva/standing; decreases with squatting |
| Pulmonary stenosis | Ejection (mid-systolic) | LUSB | Harsh | Ejection click; wide splitting of S2; louder on inspiration |
| Mitral regurgitation | Holosystolic | Apex → axilla | Blowing | Soft S1; often S3; radiates to axilla |
| Tricuspid regurgitation | Holosystolic | LLSB | Blowing | Louder on inspiration (Carvallo's sign); giant v wave in JVP |
| VSD | Holosystolic | LLSB | Harsh | Thrill common; small VSD louder (maladie de Roger) |
| MVP | Late systolic | Apex | Mid-systolic click + late systolic murmur; click moves earlier with standing |
Diastolic Murmurs (always pathological)
| Murmur | Timing | Location | Quality | Key Features |
|---|---|---|---|---|
| Aortic regurgitation | Early diastolic (decrescendo) | Left sternal edge | Blowing, high-pitched | Heard best leaning forward, exhaling; wide pulse pressure; collapsing pulse |
| Pulmonary regurgitation | Early diastolic | LUSB | Graham Steell murmur (pulmonary HTN-associated) | |
| Mitral stenosis | Mid-diastolic (rumble) + presystolic accentuation | Apex (LLD position, bell) | Low-pitched rumble | Opening snap precedes; presystolic accentuation disappears in AF |
| Tricuspid stenosis | Mid-diastolic | LLSB | Low-pitched | Accentuated by inspiration |
Continuous Murmurs
- Patent ductus arteriosus (PDA): machinery murmur, peaks at S2, heard at left infraclavicular area
- Arteriovenous fistula, venous hum (children; abolished by jugular compression)
Dynamic Auscultation - Manoeuvres
| Manoeuvre | Haemodynamic effect | Increases | Decreases |
|---|---|---|---|
| Valsalva (straining phase) | Decreased venous return, decreased LV size | HOCM, MVP click (earlier) | Most other murmurs |
| Squatting | Increased venous return + afterload | Most murmurs | HOCM, MVP |
| Standing | Decreased venous return | HOCM, MVP (earlier click) | Most murmurs |
| Inspiration | Increased right heart filling | Right-sided murmurs (TR, PS, TS) | Left-sided murmurs |
| Handgrip | Increased afterload | MR, AR, VSD | HOCM, AS |
| Passive leg raise | Increased venous return | Most murmurs | HOCM |
| Amyl nitrite | Decreased afterload, tachycardia | AS, HOCM, PS, TS | MR, AR, VSD |
7. Peripheral Signs of Specific Conditions
| Sign | Condition |
|---|---|
| Corrigan's pulse (carotid) | Severe AR |
| De Musset's sign (head nodding) | Severe AR |
| Quincke's sign (capillary pulsation in nails) | Severe AR |
| Duroziez's sign (femoral bruit) | Severe AR |
| Hill's sign (popliteal systolic BP >20 mmHg above brachial) | Severe AR |
| Ankle oedema | Right heart failure, venous insufficiency |
| Sacral oedema | Right heart failure (bed-bound patients) |
| Hepatomegaly (pulsatile) | Tricuspid regurgitation |
| Splenomegaly | Infective endocarditis, congestive cardiac failure |
Summary: Systematic Approach
- General inspection - habitus, signs of syndromes, peripheral stigmata
- Vital signs - HR, BP (both arms), SpO₂, respiratory rate
- Hands - clubbing, splinter haemorrhages, peripheral cyanosis, radial pulse
- Face/neck - malar flush, corneal arcus, xanthelasma, JVP
- Carotid pulse - character and volume
- Precordium - inspect, palpate (apex beat, heaves, thrills), percuss (cardiac dullness)
- Auscultation - S1, S2, added sounds, murmurs (all areas; dynamic manoeuvres as needed)
- Lung bases - bibasal crepitations (pulmonary oedema)
- Abdomen - hepatomegaly, splenomegaly, pulsatile aorta, ascites
- Lower limbs - peripheral pulses, oedema, signs of peripheral arterial disease
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025), pp. 1904-1908 | Fuster and Hurst's The Heart, 15th ed., Ch. 3
This is a shared conversation. Sign in to Orris to start your own chat.