Explain How to Approach Migraine
Reading File
Finding Sources
Searching PubMed
"migraine" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
migraine pathophysiology phases cortical spreading depression
I now have comprehensive content. Let me compile the full clinical answer.
Approach to Migraine
1. Understanding the Condition
Definition & Epidemiology
Migraine (from Greek hemikranios, "half head") is a primary headache disorder affecting ~12% of the general population — 18% of women and 6% of men. It ranks among the WHO's most disabling medical conditions worldwide, with lifetime prevalence of 33% in women and 13% in men. Peak prevalence is in the 4th decade. Attacks occur 1–4 times/month in most patients (episodic migraine); 2% of the population has chronic migraine (≥15 headache days/month, ≥8 fulfilling migraine criteria).
(Bradley and Daroff's Neurology in Clinical Practice)
2. The Four Phases of a Migraine Attack
| Phase | Timing | Features |
|---|---|---|
| Premonitory | Hours–days before | Fatigue, mood changes, yawning, food cravings, neck stiffness |
| Aura | ~1 hr before headache | Visual (scintillating scotoma, zigzag lines), sensory (marching paresthesias), motor, speech |
| Headache | 4–72 hours | Unilateral, pulsating, moderate–severe; photophobia, phonophobia, nausea/vomiting |
| Postdrome | After headache | Fatigue, cognitive fog, mood changes — may last 24–48 hrs |
Osmophobia, though not part of formal IHS criteria, is highly specific for migraine when present.
3. Diagnostic Criteria (ICHD-3)
Migraine Without Aura — at least 5 attacks meeting:
- Duration 4–72 hours
- ≥2 of: unilateral, pulsating, moderate/severe intensity, aggravated by routine activity
- During headache ≥1 of: nausea/vomiting or photophobia + phonophobia
Migraine With Aura — same criteria plus fully reversible aura with ≥3 of: ≥1 aura symptom spreading gradually, each symptom lasting 5–60 min, at least one unilateral aura symptom, positive symptom (flickering lights) or negative (scotoma), onset within 60 min of headache.
Special subtypes to recognize:
- Basilar-type migraine — aura from brainstem/bilateral hemispheres: dysarthria, vertigo, tinnitus, diplopia, bilateral paresthesias
- Hemiplegic migraine — reversible hemiplegia during aura (linked to CACNA1A, ATP1A2, SCN1A gene mutations)
- Chronic migraine — ≥15 headache days/month for >3 months
- Status migrainosus — continuous migraine >72 hours
4. Pathophysiology
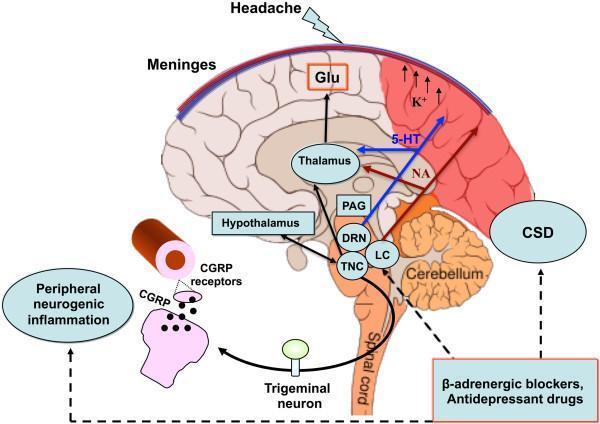
The trigeminovascular system is central to migraine pain:
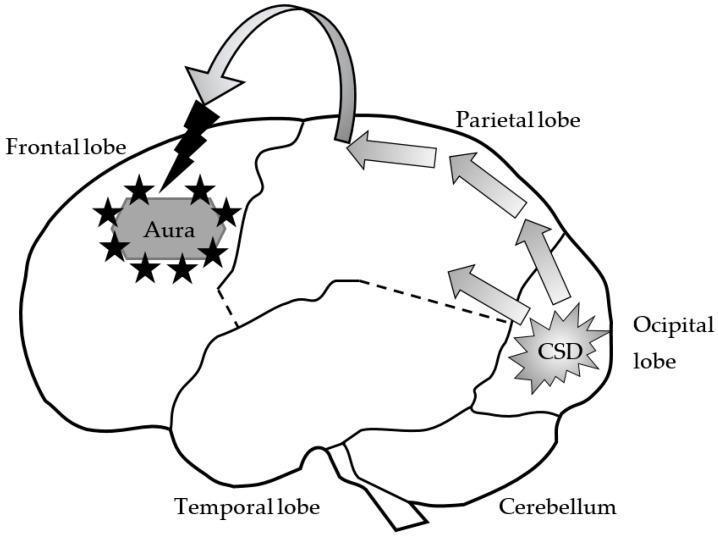
- Cortical Spreading Depression (CSD) — a slowly propagating wave of neuronal/glial depolarization (~3–5 mm/min, moving anteriorly from the occipital lobe) underlies the aura and triggers trigeminal activation.
- Activation of trigeminal nerve terminals around meningeal vessels causes release of CGRP (calcitonin gene-related peptide), substance P, and neurokinin A → neurogenic inflammation of dural vessels → pain signal transmitted via the trigeminal nucleus caudalis (TNC) → thalamus → cortex.
- Serotonin (5-HT) from the dorsal raphe nucleus and norepinephrine from the locus coeruleus modulate pain processing and descending pain inhibition.
- Central sensitization (allodynia — pain from normally non-painful stimuli like brushing hair or light touch) develops during prolonged attacks, reflecting activation of second- and third-order trigeminal neurons.
- Genetics: Familial hemiplegic migraine is autosomal dominant; common migraine is polygenic with ~44 susceptibility loci identified by GWAS, enriched in smooth/vascular tissue and synaptic regulation genes.
5. Diagnostic Workup
Most patients do NOT need testing — migraine is a clinical diagnosis.
Red flags requiring imaging/workup (secondary headache exclusion):
- Thunderclap onset ("worst headache of life") → SAH
- New headache after age 50
- Progressive/worsening pattern
- Neurological deficits not typical of known aura
- Fever, meningismus
- Headache with Valsalva, exertion, or positional change
When indicated:
- MRI brain (preferred over CT for most non-acute settings)
- Blood tests: TSH, ESR/CRP (to exclude temporal arteritis)
- LP if SAH suspected and CT negative
- MR angiography/venography if vascular cause suspected
6. Management
A. Non-Pharmacological (Always First-Line)
- Identify and avoid triggers: alcohol, caffeine (or withdrawal), hormonal contraceptives, nitrates, aged cheese, chocolate, missed meals, sleep disruption, strong odors, weather changes, stress
- Maintain regular sleep, meals, exercise, hydration
- Stress management (CBT, biofeedback, relaxation training)
- Headache diary — essential for tracking frequency, triggers, medication use
B. Acute (Abortive) Pharmacotherapy
The choice of abortive agent is based on attack severity:
Mild–Moderate Attacks:
| Drug | Dose | Notes |
|---|---|---|
| Aspirin 900 mg + metoclopramide | At onset | First-line; antiemetic improves absorption |
| Ibuprofen 400–600 mg | At onset | Effective, widely available |
| Naproxen sodium 500–825 mg | At onset | Longer-acting NSAID |
| Acetaminophen 1000 mg | At onset | Less effective alone; useful in pregnancy |
Moderate–Severe Attacks — Triptans (5-HT1B/1D agonists):
| Triptan | Dose | Route |
|---|---|---|
| Sumatriptan | 25–100 mg PO / 6 mg SC / 20 mg intranasal | Gold standard; SC fastest onset |
| Rizatriptan | 10 mg PO | Faster onset than sumatriptan PO |
| Zolmitriptan | 2.5–5 mg PO or nasal | Good efficacy |
| Eletriptan | 20–40 mg PO | Longer half-life; fewer recurrences |
| Naratriptan | 2.5 mg PO | Slower onset; lower recurrence rate |
Triptans are contraindicated in: hemiplegic migraine, basilar migraine, ischaemic heart disease, uncontrolled hypertension, prior stroke/TIA.
CGRP Receptor Antagonists (Gepants) — newer class:
- Ubrogepant, rimegepant — oral, effective without vasoconstrictive side effects; useful when triptans are contraindicated or poorly tolerated
Antiemetics (also enhance analgesia):
- Metoclopramide 10 mg IV/IM, prochlorperazine 10 mg IV — first-line in ED; also have direct antimigraine effect
- Domperidone 10 mg — useful for nausea + enhances oral drug absorption
For severe/refractory attacks (ED setting):
- IV prochlorperazine or metoclopramide + diphenhydramine (reduce akathisia)
- IV ketorolac 30 mg
- IV valproate sodium
- Dexamethasone 10 mg IV (reduces recurrence)
- Avoid opioids — risk of medication overuse headache and hyperalgesia
Status Migrainosus (>72 hrs):
- IV dihydroergotamine (DHE) + antiemetic — highly effective
- Short course IV methylprednisolone
- Inpatient admission often required
C. Preventive (Prophylactic) Pharmacotherapy
Indications for initiating prophylaxis:
- ≥4 migraine days/month with significant disability
- ≥8 headache days/month (regardless of disability)
- Attacks unresponsive to acute therapy
- Contraindications to acute medications
- Medication overuse headache (>10–15 days/month of analgesic use)
- Special subtypes (hemiplegic, basilar, or migrainous infarction)
First-line agents:
| Drug Class | Examples | Target |
|---|---|---|
| Beta-blockers | Propranolol 40–240 mg, metoprolol | Reduces attack frequency 50%+; first-line |
| Tricyclic antidepressants | Amitriptyline 10–75 mg | Useful with comorbid depression/insomnia |
| Anticonvulsants | Topiramate 25–100 mg, valproate 500–1500 mg | FDA-approved; topiramate also causes weight loss |
| Calcium channel blockers | Verapamil, flunarizine | Useful in menstrual migraine |
| CGRP pathway mAbs (monoclonal antibodies) | Erenumab, fremanezumab, galcanezumab, eptinezumab | SC/IV monthly or quarterly; FDA-approved; highly effective for chronic/refractory migraine |
CGRP monoclonal antibodies represent the most significant advance in migraine prevention in decades — they target CGRP or its receptor directly and are well-tolerated with minimal systemic side effects.
- Allow 2–3 months to assess efficacy before changing prophylaxis
- Continue for at least 6–12 months before considering tapering
D. Non-Pharmacological Preventive Measures
- Biofeedback + relaxation training — Level A evidence, comparable to pharmacotherapy
- Cognitive behavioral therapy (CBT) — especially effective combined with medications
- Transcranial magnetic stimulation (TMS) — FDA-cleared for acute and preventive use
- Neuromodulation devices — CEFALY (supraorbital nerve stimulation) approved for prevention
- Acupuncture — evidence supports modestly; equivalent to prophylactic drugs in some trials
- Magnesium supplementation 400–600 mg/day — particularly for menstrual migraine
- Riboflavin (Vitamin B2) 400 mg/day — well-tolerated, modest benefit
- Coenzyme Q10 100 mg TID
7. Special Situations
Menstrual Migraine:
- Often more severe and refractory
- Perimenstrual prophylaxis: naproxen sodium 550 mg twice daily starting 2 days before expected menses, or triptan mini-prophylaxis (frovatriptan 2.5 mg BD for 6 days)
Migraine in Pregnancy:
- Triptans and ergotamines generally avoided (limited safety data)
- Acetaminophen ± metoclopramide — safest acute options
- Magnesium IV (1–2 g) — safe and effective
- Prophylaxis: low-dose amitriptyline, metoprolol (with obstetric guidance)
Pediatric Migraine:
- Affects 4–10% of school-age children
- Ibuprofen 10 mg/kg and paracetamol are first-line
- Sumatriptan nasal spray approved ≥12 years
- Prophylaxis: amitriptyline, topiramate (FDA-approved in adolescents)
Medication Overuse Headache (MOH):
- Occurs with analgesic/triptan use >10–15 days/month for >3 months
- Treatment: withdraw the overused medication (may require bridging with naproxen or prednisolone), then establish preventive therapy
- Patient education is critical to prevent recurrence
8. When to Refer
- Uncertain diagnosis
- Frequent (≥4/month) or disabling migraine unresponsive to 2–3 preventive agents
- Suspected MOH requiring structured withdrawal
- Hemiplegic or basilar migraine
- Consideration for CGRP biologics or neuromodulation
Recent Evidence
A 2025 evidence-based guideline in Cephalalgia (Ornello et al., PMID 40277319) consolidates pharmacological recommendations and confirms CGRP-targeting therapies (both gepants for acute treatment and mAbs for prevention) as first-tier options in appropriate patients. A 2024 network meta-analysis in the BMJ (Karlsson et al., PMID 39293828) found that triptans combined with NSAIDs ranked highest for acute migraine relief, and gepants offer a viable alternative with fewer cardiovascular contraindications.
Key takeaway: Migraine management is individualized. The cornerstone is: (1) confirming the diagnosis, (2) identifying and modifying triggers, (3) stratified acute therapy based on severity, and (4) preventive therapy for frequent/disabling attacks — with CGRP-targeting agents now transforming the landscape for refractory cases.
Sources: Bradley and Daroff's Neurology in Clinical Practice; Textbook of Family Medicine 9e; Cummings Otolaryngology; BMJ 2024; Cephalalgia 2025
This is a shared conversation. Sign in to Orris to start your own chat.