Detailed explanation ECG FOR NORCET NURSING EXAM S
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG interpretation NORCET nursing exam important topics 2024 2025
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from authoritative medical textbooks and rich ECG images. Let me compile a thorough NORCET-focused ECG guide.
📋 ECG Interpretation — Complete NORCET Nursing Exam Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Miller's Anesthesia, Morgan & Mikhail's Clinical Anesthesiology, Goldman-Cecil Medicine — Medical Textbook Library
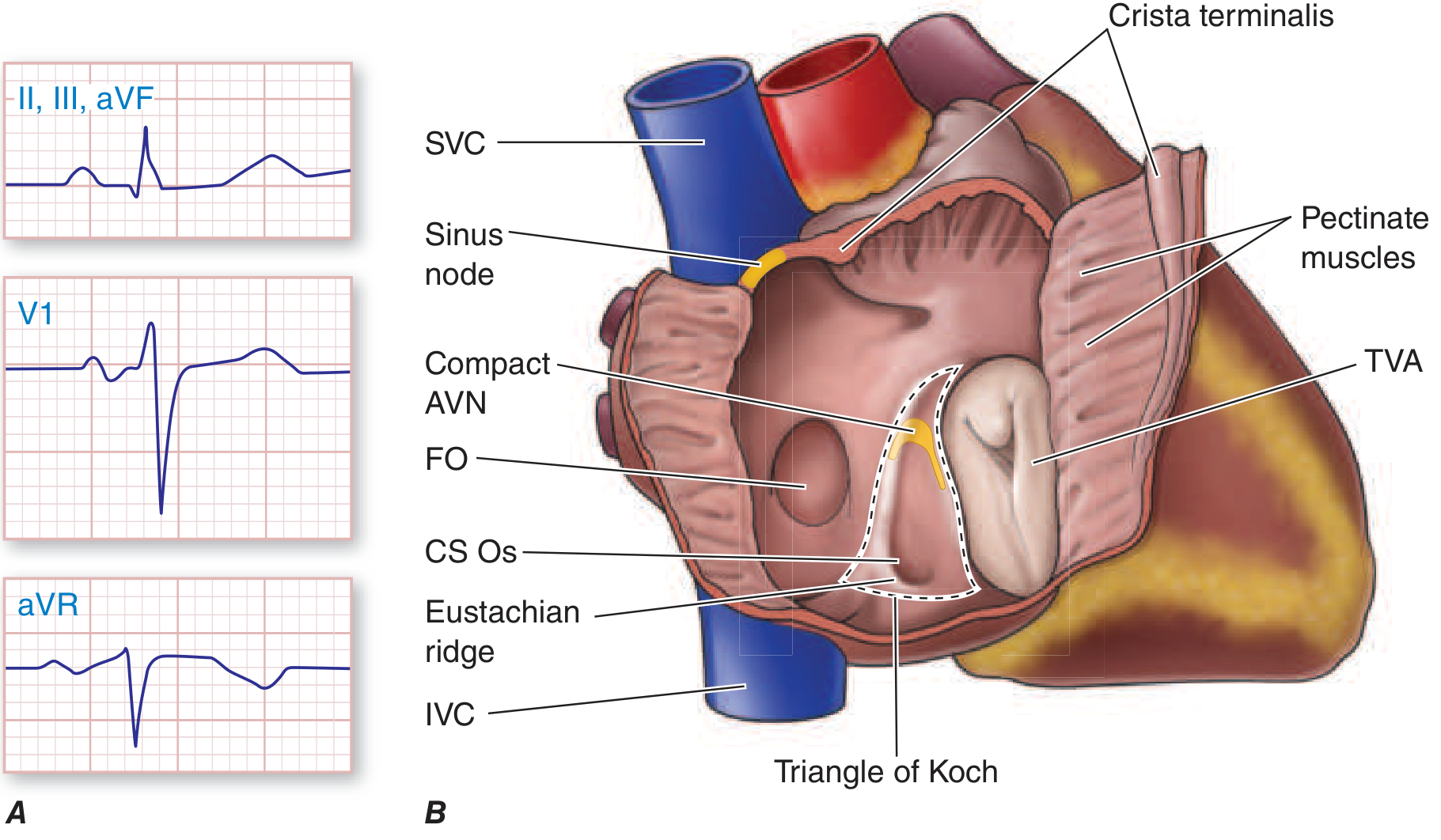
1. ECG BASICS: THE CARDIAC CONDUCTION SYSTEM
The ECG records electrical potential differences generated by the heart at the body surface.

Conduction Pathway (Must Memorize for NORCET):
SA Node → Atria → AV Node → Bundle of His →
Left & Right Bundle Branches → Purkinje Fibers → Ventricular myocardium
2. ECG PAPER & MEASUREMENTS
| Parameter | Small Box | Large Box |
|---|---|---|
| Time (horizontal) | 0.04 sec | 0.20 sec |
| Voltage (vertical) | 0.1 mV | 0.5 mV |
ECG Lead Placement (12-Lead):
- Limb leads: I, II, III, aVR, aVL, aVF (frontal plane)
- Precordial leads: V1–V6 (horizontal plane)
3. NORMAL ECG WAVEFORMS — NORCET HIGH-YIELD
P Wave
- Represents atrial depolarization (SA node → atria)
- Normal: upright in lead II, inverted in aVR
- Duration: ≤ 0.12 sec (3 small boxes)
- Amplitude: ≤ 2.5 mm
PR Interval
- From start of P to start of QRS
- Represents AV node conduction delay
- Normal: 0.12–0.20 sec (3–5 small boxes)
-
0.20 sec = 1st degree AV block
QRS Complex
- Represents ventricular depolarization
- Normal duration: 0.06–0.10 sec (< 3 small boxes)
-
0.12 sec = bundle branch block
- Q wave: first negative deflection
- R wave: first positive deflection
- S wave: negative deflection after R
ST Segment
- Represents plateau phase of ventricular action potential
- Should be isoelectric (flat/at baseline)
- Elevation = acute MI / pericarditis
- Depression = ischemia / NSTEMI
T Wave
- Represents ventricular repolarization
- Normally upright in most leads, inverted in aVR
- Tall peaked T = hyperkalemia (early sign)
- Flattened/inverted T = ischemia, hypokalemia
QT Interval
- From start of QRS to end of T wave
- Represents total ventricular electrical activity
- Normal: 0.36–0.44 sec
- Prolonged QT → risk of Torsades de Pointes
- Prolonged by: hypocalcemia, hypokalemia, hypomagnesemia, quinidine, amiodarone
- Shortened by: hypercalcemia
U Wave
- Small positive deflection after T wave
- Prominent U wave = hypokalemia (classic sign)
4. HEART RATE CALCULATION
Quick Method (NORCET Favorite):
Rate = 300 ÷ number of large boxes between R waves
| Boxes Between R waves | Heart Rate |
|---|---|
| 1 | 300 |
| 2 | 150 |
| 3 | 100 |
| 4 | 75 |
| 5 | 60 |
| 6 | 50 |
Normal heart rate: 60–100 bpm
Bradycardia: < 60 bpm | Tachycardia: > 100 bpm
Bradycardia: < 60 bpm | Tachycardia: > 100 bpm
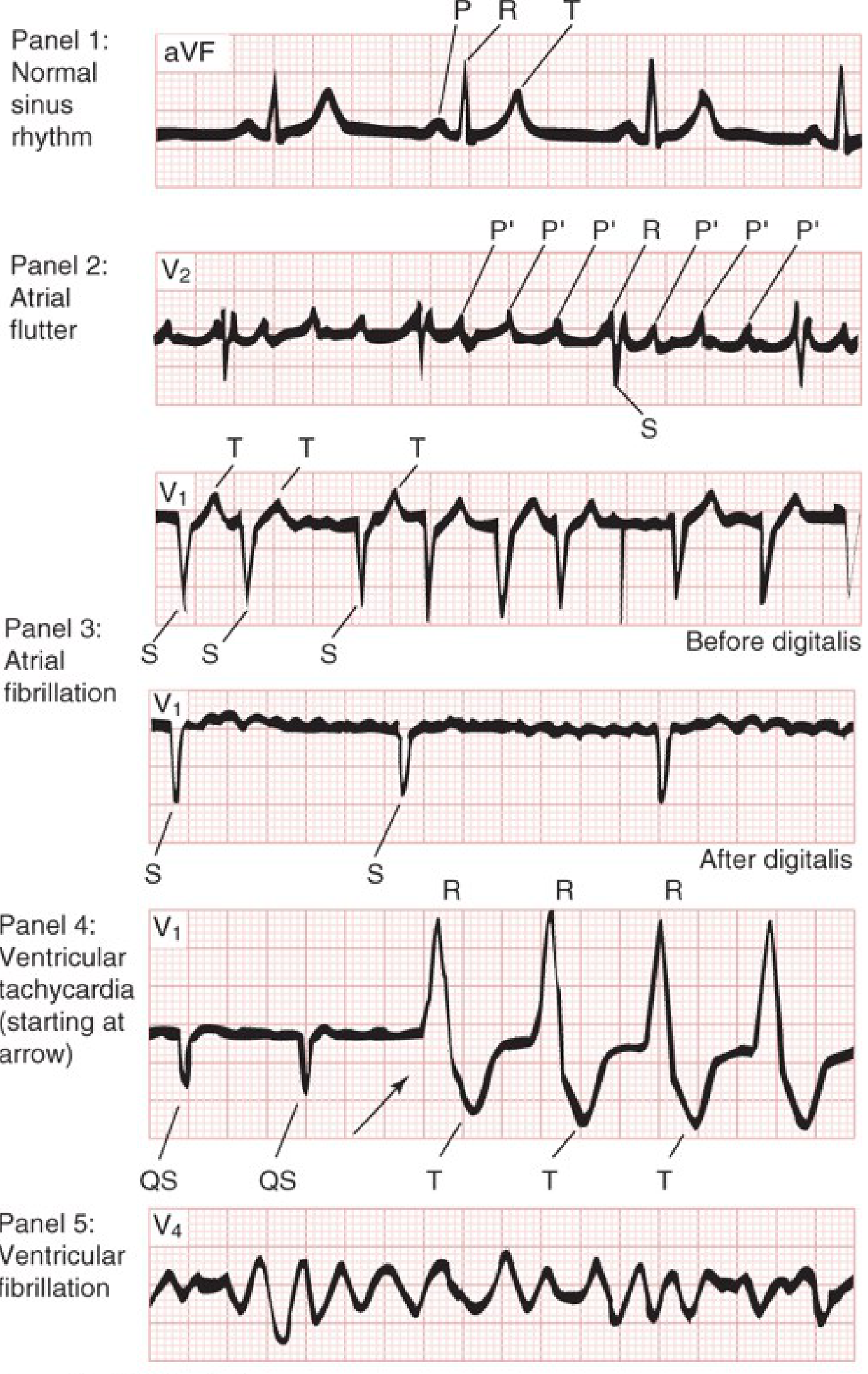
5. NORMAL SINUS RHYTHM (NSR) — Criteria
- P wave present before every QRS
- P wave upright in lead II, inverted in aVR
- PR interval: 0.12–0.20 sec
- QRS: < 0.12 sec
- Rate: 60–100 bpm
- Regular R-R interval
6. SINUS NODE ARRHYTHMIAS
| Arrhythmia | Rate | ECG Feature | Cause |
|---|---|---|---|
| Sinus Tachycardia | >100 | Normal P + QRS, rate up | Fever, pain, hypovolemia, PE, anxiety |
| Sinus Bradycardia | <60 | Normal P + QRS, rate down | Athletes, hypothyroidism, beta-blockers, increased vagal tone |
| Sinus Arrhythmia | Variable | P-P interval varies with respiration | Normal variant (especially children) |
7. AV BLOCKS — MOST IMPORTANT FOR NORCET
1st Degree AV Block
- PR interval > 0.20 sec (> 5 small boxes)
- Every P is followed by a QRS
- Usually benign
- Causes: digitalis, beta-blockers, inferior MI, increased vagal tone
2nd Degree AV Block — Type I (Wenckebach/Mobitz I)
- Progressive lengthening of PR interval until a QRS is dropped
- Then cycle resets
- Block is usually at the AV node
- Usually benign, seen in inferior MI
- Mnemonic: "Longer, longer, longer, DROP! — then you have a Wenckebach"
2nd Degree AV Block — Type II (Mobitz II)
- Constant PR interval with sudden, unexpected dropped QRS (no warning)
- Block is in His bundle or bundle branches → QRS usually wide
- Can progress to complete heart block
- Associated with anteroseptal MI — dangerous!
- Requires pacemaker
3rd Degree (Complete) AV Block
- Complete dissociation between P waves and QRS complexes
- Atrial rate faster than ventricular rate
- Escape rhythm takes over (ventricular rate 20–40 bpm, wide QRS)
- Medical emergency → Pacemaker required
- Causes: inferior/anterior MI, digitalis toxicity, congenital
| Block | PR Interval | Dropped QRS | Treatment |
|---|---|---|---|
| 1st degree | Long (>0.20s) | None | Observe |
| 2nd degree Mobitz I | Progressively longer | Yes (after longest PR) | Observe/Atropine |
| 2nd degree Mobitz II | Constant | Yes (sudden) | Pacemaker |
| 3rd degree (complete) | N/A — dissociated | All — AV dissociation | Pacemaker emergency |
8. TACHYARRHYTHMIAS
Supraventricular Tachycardias (Narrow QRS unless aberrant conduction)
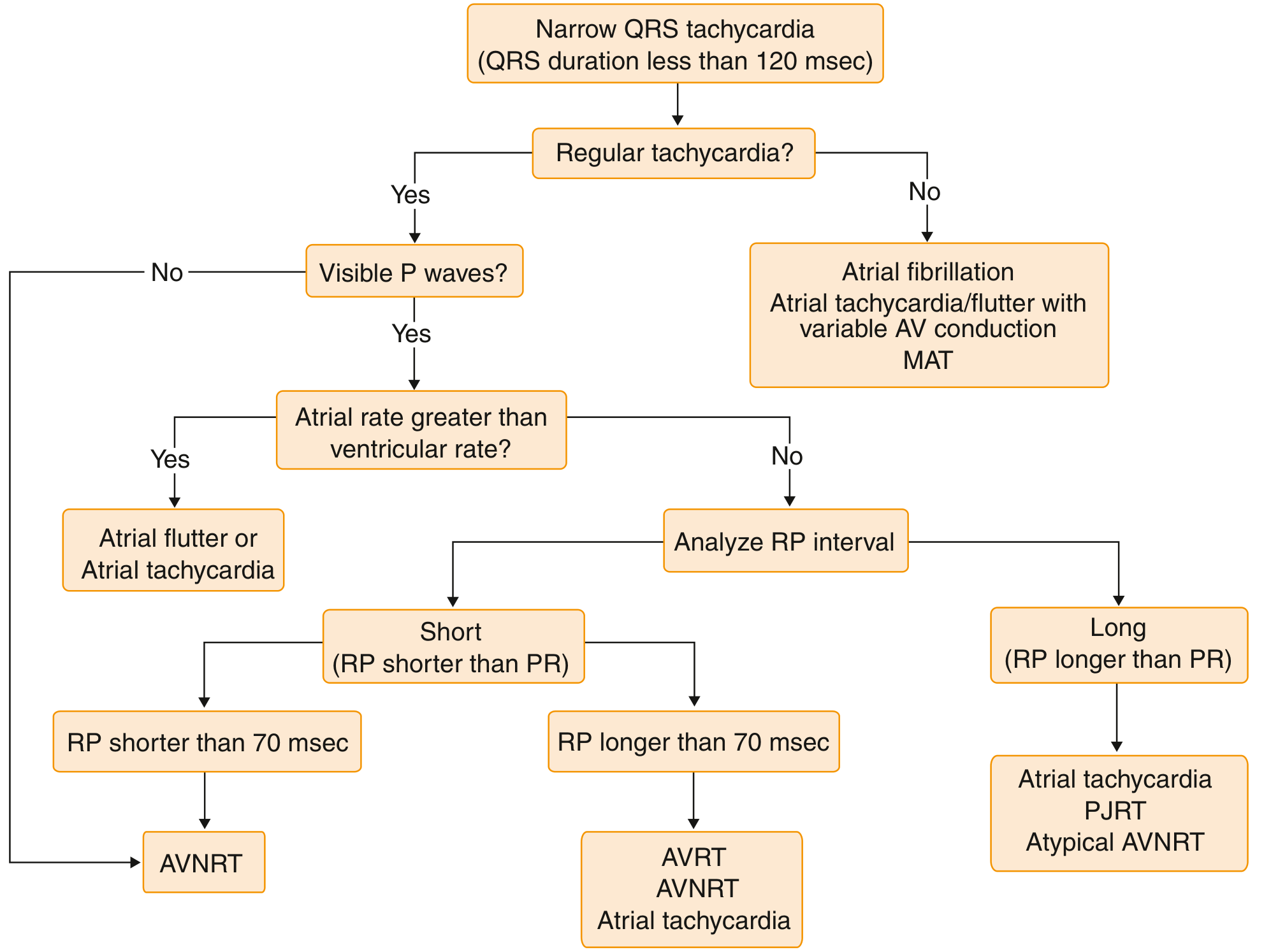
Atrial Fibrillation (AF)
- Absent P waves; irregularly irregular QRS
- Fibrillatory baseline (wavy/chaotic)
- Ventricular rate 100–180 bpm (uncontrolled)
- Risk: stroke (thrombus formation in left atrium)
- Treatment: rate control (beta-blockers, digoxin), rhythm control, anticoagulation
Atrial Flutter
- Sawtooth flutter waves (F waves) at 250–350/min, best seen in II, III, aVF
- Usually 2:1, 3:1 or 4:1 AV conduction (regular ventricular response)
- Ventricular rate ~150 bpm in 2:1 block
- Treatment: cardioversion, rate control, ablation
PSVT / SVT (AV Nodal Re-entry Tachycardia — AVNRT)
- Heart rate 150–250 bpm
- Narrow QRS, P waves hidden in or just after QRS
- Treat: Valsalva maneuver → Adenosine (drug of choice) → Cardioversion if unstable
Junctional Tachycardia
- Origin: AV node / Bundle of His
- P wave absent, inverted, or after QRS
- Rate 60–100 (accelerated junctional) or >100 (junctional tachycardia)
9. VENTRICULAR ARRHYTHMIAS — LIFE-THREATENING
Premature Ventricular Contractions (PVCs)
- Wide, bizarre QRS (>0.12s) without preceding P wave
- Compensatory pause follows
- Isolated PVCs: benign; frequent (>6/min) or multifocal = concerning
Ventricular Tachycardia (VT)
- ≥ 3 consecutive PVCs at rate > 100 bpm
- Wide bizarre QRS complexes; P waves absent or dissociated
- Can be sustained (>30 sec) or non-sustained
- Treatment: Amiodarone (drug of choice); if pulseless → Defibrillation + CPR
Ventricular Fibrillation (VF)
- Chaotic, irregular baseline — no discernible QRS complexes
- No cardiac output = cardiac arrest
- Treatment: Immediate Defibrillation (unsynchronized shock) + CPR
- Drugs: Epinephrine, Amiodarone
Torsades de Pointes
- "Twisting of the points" — polymorphic VT
- QRS complexes twist around baseline
- Caused by prolonged QT interval
- Treat: IV Magnesium Sulfate (drug of choice)
10. BUNDLE BRANCH BLOCKS
Right Bundle Branch Block (RBBB)
- Wide QRS (>0.12 sec)
- rSR' (M-shape or "rabbit ears") in V1
- Wide S wave in leads I, aVL, V5, V6
- Can be normal variant or seen in PE, RVH
Left Bundle Branch Block (LBBB)
- Wide QRS (>0.12 sec)
- Broad, notched R wave (W-shape) in V5, V6
- Deep S or QS in V1
- Nearly always indicates underlying heart disease
- New LBBB in chest pain = treat as STEMI
Mnemonic: WiLLiaM MaRRoW
- WILLIAM = LBBB → W in V1, M in V5/V6
- MARROW = RBBB → M in V1, W in V5/V6

11. MYOCARDIAL INFARCTION ON ECG
Evolutionary ECG Changes in STEMI:
- Hyperacute T waves (tall, peaked) — minutes
- ST elevation (tombstone/coved) — early (minutes to hours)
- Q wave formation (pathologic, >0.04 sec wide, >1/3 QRS height) — hours to days (permanent)
- T wave inversion — hours to days
- ST segment normalizes — days to weeks
Localization of MI by Leads:
| Territory | Culprit Artery | Leads with Changes |
|---|---|---|
| Anterior | LAD | V1–V4 |
| Anteroseptal | LAD (septal branch) | V1–V2 |
| Anterolateral | LAD / LCx | V1–V6, I, aVL |
| Lateral | LCx | I, aVL, V5–V6 |
| Inferior | RCA | II, III, aVF |
| Right ventricular | RCA | V4R (right-sided lead) |
| Posterior | RCA / LCx | Tall R in V1–V2, reciprocal ST depression |
STEMI vs NSTEMI:
| STEMI | NSTEMI | |
|---|---|---|
| ST segment | Elevated | Depressed or flat |
| Q waves | Often develop | Usually absent |
| Troponin | Elevated | Elevated |
| Treatment | Urgent PCI/thrombolysis | Medical management / PCI |
12. ELECTROLYTE CHANGES ON ECG
| Electrolyte | ECG Change | Key Feature |
|---|---|---|
| Hyperkalemia | Peaked (tall) T waves → wide QRS → sine wave → VF | Earliest = tall T waves |
| Hypokalemia | Flat T waves, prominent U waves, ST depression | U wave > T wave = hypokalemia |
| Hypercalcemia | Shortened QT interval | |
| Hypocalcemia | Prolonged QT interval | Risk of TdP |
| Hypermagnesemia | Prolonged PR, wide QRS | |
| Hypomagnesemia | Prolonged QT → TdP |
13. PERICARDITIS ECG FINDINGS
- Diffuse ST elevation in all/most leads (saddle-shaped)
- PR segment depression (very specific for pericarditis)
- No reciprocal changes (differentiates from MI)
- Later: ST returns to normal, T wave inversions
14. WOLFF-PARKINSON-WHITE (WPW) SYNDROME
- Accessory pathway (Bundle of Kent) bypasses AV node
- Short PR interval (<0.12 sec)
- Delta wave (slurred upstroke of QRS)
- Wide QRS
- Prone to PSVT and AF with rapid conduction
- Treat: Procainamide or ablation; avoid AV-nodal blockers (adenosine, digoxin, verapamil)
15. ECG IN PULMONARY EMBOLISM
- Most common finding: Sinus tachycardia
- Classic (but insensitive): S1Q3T3 pattern — prominent S wave in lead I, Q wave and T-wave inversion in lead III
- Right heart strain: right axis deviation, RBBB, T-wave inversions V1–V4
16. SYSTEMATIC APPROACH TO READING ANY ECG (14-Point Checklist)
Per Harrison's Principles of Internal Medicine 22E:
- Standardization (10 mm = 1 mV calibration)
- Rhythm (sinus or not?)
- Heart rate (300 ÷ large boxes)
- PR interval (AV conduction)
- QRS duration (bundle branch block?)
- QT/QTc interval
- Mean QRS electrical axis
- P waves (morphology, axis)
- QRS voltages (LVH/RVH criteria)
- Precordial R-wave progression (V1 → V6)
- Abnormal Q waves (infarction?)
- ST segments (elevation or depression?)
- T waves (inversion, peaked?)
- U waves (prominent = hypokalemia)
17. NORCET EXAM HIGH-YIELD QUICK MNEMONICS
| Mnemonic | Meaning |
|---|---|
| "W-I-L-L-I-A-M, M-A-R-R-O-W" | LBBB = W in V1, M in V6; RBBB = M in V1, W in V6 |
| "Longer, Longer, DROP" | Wenckebach (Mobitz I) |
| "STEMI = elevation, NSTEMI = depression" | MI recognition |
| "Tall Tents = K (Hyperkalemia)" | Tall T waves |
| "U see Uka (U wave) in hypoKalemia" | U wave prominence |
| "Shorten QT → Ca+ up (Hypercalcemia)" | QT shortening |
| "Prolong QT → Ca- down (Hypocalcemia)" | QT prolongation |
| "Torsades → Mg2+" | TdP treatment = Magnesium |
| "Adenosine for SVT" | Drug of choice for SVT |
| "Shock VF first" | Defibrillation for VF/pulseless VT |
18. COMMONLY TESTED NORCET SCENARIO QUICK-ANSWER TABLE
| ECG Finding | Diagnosis |
|---|---|
| Absent P waves + irregularly irregular QRS | Atrial Fibrillation |
| Sawtooth flutter waves ~300/min | Atrial Flutter |
| Short PR + delta wave | WPW Syndrome |
| Progressive PR prolongation → dropped QRS | 2nd Degree AV Block Mobitz I (Wenckebach) |
| Sudden dropped QRS, constant PR, wide QRS | 2nd Degree AV Block Mobitz II |
| P waves and QRS completely dissociated | Complete (3rd Degree) AV Block |
| ST elevation + Q waves | STEMI |
| ST depression + inverted T | NSTEMI / Ischemia |
| Diffuse ST elevation + PR depression | Pericarditis |
| Peaked T, wide QRS, sine wave | Hyperkalemia |
| Prominent U waves | Hypokalemia |
| Prolonged QT, twisting QRS | Torsades de Pointes |
| Chaotic baseline, no QRS | Ventricular Fibrillation |
| Wide QRS ≥3 at >100 bpm | Ventricular Tachycardia |
| rSR' (M-shape) in V1 | RBBB |
| Broad notched R in V5/V6 | LBBB |
| S1Q3T3, sinus tachycardia | Pulmonary Embolism |
This guide covers every major ECG topic tested in the NORCET exam based on Harrison's, Goldman-Cecil, Miller's Anesthesia, and Morgan & Mikhail's Anesthesiology. Study the arrhythmia recognition table and the systematic 14-point approach — they appear most frequently as MCQs. Good luck!
Norcet exam ?
Searching the Web
NORCET exam 2025 2026 complete details syllabus pattern eligibility AIIMS
Searching the Web
NORCET nursing officer recruitment exam latest notification 2025
Reading Web Page
https://www.adda247.com/exams/nursing/aiims-norcet-syllabus/
Here is a complete overview of the NORCET exam:
🏥 NORCET — Complete Guide (2025–2026)
What is NORCET?
NORCET = Nursing Officer Recruitment Common Eligibility Test
- Conducted by AIIMS New Delhi on behalf of multiple AIIMS institutions across India
- Selects candidates for Nursing Officer (Group B) posts
- Held twice a year (approximately)
- Official website: aiimsexams.ac.in
Latest Status: NORCET 10 (2026)
| Update | Details |
|---|---|
| Notification released | 24 February 2026 |
| Total vacancies | 2,551 posts |
| Institutes covered | AIIMS New Delhi, AIIMS institutions pan-India, NITRD, AIIPMR Mumbai, CNCI Kolkata |
| Stage I (Prelims) | 11 April 2026 |
| Stage II (Mains) | 30 April 2026 |
| Mains Result declared | 12 May 2026 ✅ |
| Next step | Seat Allotment / Document Verification |
Eligibility Criteria
Educational Qualification
Option A (B.Sc. Route):
- B.Sc. Nursing / B.Sc. Nursing (Hons.) / Post-Basic B.Sc. Nursing from a recognized institution
- Must be registered as Nurse & Midwife with State/Indian Nursing Council
Option B (GNM Route):
- Diploma in GNM from a recognized institution
- Valid Nurse & Midwife registration
- Minimum 2 years of experience in a hospital with ≥50 beds
Age Limit
- 18 to 30 years (age relaxation for SC/ST/OBC/PwD as per government norms)
Exam Pattern
Stage I — Prelims (Qualifying)
| Feature | Detail |
|---|---|
| Mode | Computer-Based Test (CBT) |
| Questions | 100 MCQs |
| Breakdown | 80 Nursing + 20 GK & Aptitude |
| Duration | 90 minutes |
| Marking | +1 correct / −1/3 wrong |
| Purpose | Qualifying round only (not counted in merit) |
Stage II — Mains (Merit-Based)
| Feature | Detail |
|---|---|
| Mode | Computer-Based Test (CBT) |
| Questions | 160 MCQs (Nursing only) |
| Duration | 180 minutes (3 hours) |
| Marking | +1 correct / −1/3 wrong |
| Purpose | Decides final merit list |
Syllabus
GK & Aptitude (Prelims only — 20 questions)
- Current affairs, Indian Constitution, Healthcare policies
- Number system, Percentage, Ratio & Proportion, Time & Distance, Profit & Loss, Simple/Compound Interest, Permutation & Combination
Nursing Subjects (Main syllabus — Prelims 80 Qs + Mains 160 Qs)
| Subject | Key Topics |
|---|---|
| Anatomy & Physiology | Organ systems, cardiac cycle, nervous system |
| Fundamentals of Nursing | Nursing process, vital signs, wound care, sterile techniques |
| Medical-Surgical Nursing | ECG, cardiac conditions, respiratory, neuro, ortho, renal, oncology |
| Obstetric & Gynecological Nursing | ANC, labor, postnatal care, gynecological disorders |
| Pediatric Nursing | Growth milestones, immunization schedule, neonatal care |
| Community Health Nursing | National Health Programs, epidemiology, PHC |
| Mental Health Nursing | Schizophrenia, mood disorders, defense mechanisms, psychiatric drugs |
| Microbiology | Infection control, sterilization, pathogens |
| Pharmacology | Drug classifications, nursing implications, calculations |
| Nutrition | Therapeutic diets, deficiency diseases |
| Nursing Management | Administration, ethics, legal aspects |
| Biochemistry | Lab values, enzymes, metabolic pathways |
Application Fee
- ₹3,000 (General/OBC)
- Reduced for SC/ST/PwD (check official notification for current rates)
- Payment: Online (Debit/Credit Card, Net Banking)
Salary & Pay Scale
- Pay Level 7 of the 7th Pay Commission Pay Matrix
- Basic Pay: ₹44,900/month
- Gross salary with allowances (HRA, DA): approximately ₹60,000–₹75,000/month depending on posting city
Selection Process
Online Application → Stage I CBT (Prelims) → Qualify →
Stage II CBT (Mains) → Merit List → Document Verification → Appointment
Preparation Tips for NORCET
| Strategy | Detail |
|---|---|
| High-yield topics | ECG, cardiac nursing, IMCI, drug calculations, labor stages |
| Practice MCQs daily | Previous year papers are very representative |
| Negative marking | Attempt only if ≥60–70% confident |
| Stage II is what counts | Focus most energy on mains-level depth |
| National Health Programs | Frequently asked — RNTCP, NPCDCS, NHM, JSSK, etc. |
| Pharmacology | Drug of choice for conditions is a common question type |
Official Resources
- Official website: aiimsexams.ac.in
- Results & notifications: Check the NORCET section under "Recruitment"
NORCET 11 is expected to be notified in mid-to-late 2026. Keep checking the official AIIMS website for new notifications.
Norcet mains
Asking for Preferences
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.