chronic pds and acute pds types
acute peritoneal dialysis and chronic peritoneal dialysis types
Peritoneal Dialysis (PD): Acute vs. Chronic Types
Acute Peritoneal Dialysis
- Hyperkalemia refractory to medical management
- Metabolic acidosis refractory to treatment
- Volume overload refractory to diuretics
- Uremic encephalopathy or pericarditis
- Certain intoxications (methanol, ethylene glycol, salicylates)
- Resource-limited settings where hemodialysis machines are unavailable (e.g., used extensively during COVID-19 pandemic)
- Washington Manual of Medical Therapeutics, p. 503
- Fischer's Mastery of Surgery 8th ed., p. 5783
Chronic Peritoneal Dialysis
Types of Chronic PD
| Type | Full Name | Description |
|---|---|---|
| CAPD | Continuous Ambulatory Peritoneal Dialysis | Manual instillation and drainage of dialysate fluid 3-5 times per day. Fluid is always present in the peritoneal cavity (continuous). No machine needed - patient does exchanges by hand using gravity. |
| APD | Automated Peritoneal Dialysis | Use of a cycler machine to instill and drain fluid. Umbrella term for all machine-based PD. |
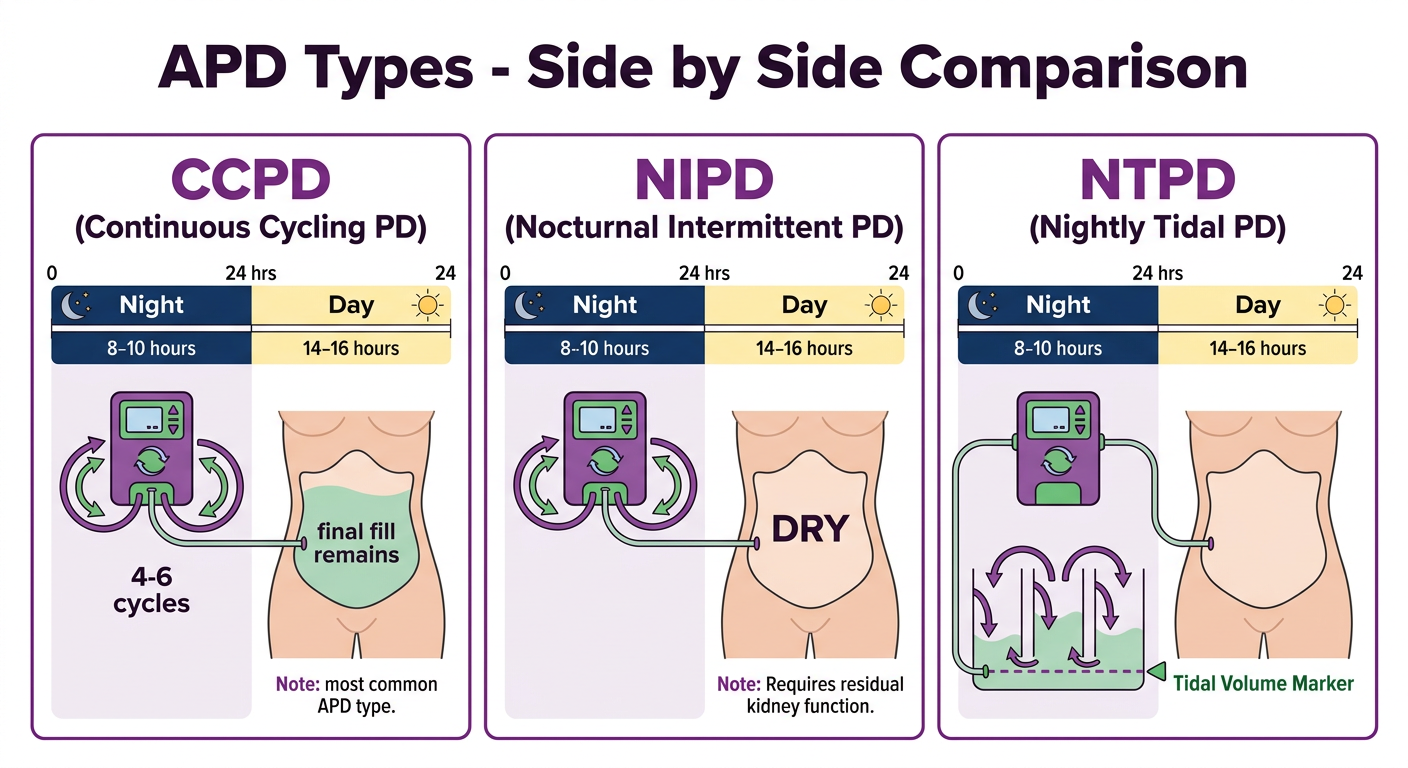
| CCPD | Continuous Cycling Peritoneal Dialysis | APD performed at night (machine runs exchanges while patient sleeps) plus a final "fill" of fluid left in the peritoneal cavity during the day. An extra daytime exchange may also be done. Most widely used APD modality. |
| NIPD | Nocturnal Intermittent Peritoneal Dialysis | APD performed at night only - no fluid fill during the day (abdomen is "dry" during daytime). Appropriate only for patients with significant residual kidney function (RKF). |
| NTPD | Nightly Tidal Peritoneal Dialysis | A cycler-based APD variant where only a portion of the dialysate is drained each cycle, leaving a tidal volume behind to reduce time spent in the drain/fill phase. |
| DAPD | Daytime Ambulatory Peritoneal Dialysis | Manual exchanges performed during the day; patient has a "dry night." Used in selected patients. |
| IPPD | Intermittent Peritoneal Dialysis | Thrice-weekly treatment; less commonly used today. |
- Fischer's Mastery of Surgery 8th ed., Table 209.1
- Brenner & Rector's The Kidney, PD Modalities section
- Smith & Tanagho's General Urology 19th ed., p. 574
Key Distinction: Continuous vs. Intermittent
| Feature | Continuous (CAPD, CCPD) | Intermittent (NIPD, IPPD) |
|---|---|---|
| Dialysate in cavity | 24 hours/day, 7 days/week | Only during treatment period |
| Residual kidney function needed | No (can manage without) | Yes (requires significant RKF) |
| Sodium sieving problem | Less prominent | More prominent (short dwells) |
| Ultrafiltration | More reliable | Risk of reabsorption with long dry period |
Choosing Between CAPD and CCPD
-
Patient preference is the primary driver
-
Peritoneal transport rate matters: slow/low transporters need longer dwells (favors CAPD); fast/high transporters benefit from shorter night dwells (favors CCPD)
-
Prescription variables for any PD type: dwell volume (typically 2-3 L), dwell time, number of exchanges, dextrose concentration (1.5%, 2.5%, or 4.25%)
-
Icodextrin - a glucose polymer - is used for long dwells as it is minimally absorbed and maintains osmotic gradient up to 18 hours
-
Washington Manual of Medical Therapeutics, p. 505
-
Brenner & Rector's The Kidney
diagrams separate with headings
Medical diagram titled "ACUTE Peritoneal Dialysis" showing indications for acute PD: AKI (Acute Kidney Injury), Hyperkalemia refractory to treatment, Metabolic acidosis refractory to treatment, Volume overload refractory to diuretics, Uremic encephalopathy, Uremic pericarditis, Intoxications (methanol, ethylene glycol, salicylates), Resource-limited settings. Below that show the technique: Intermittent Peritoneal Dialysis (IPD) with frequent rapid exchanges over 10-36 hours every few days. Clean medical education style with blue color scheme, white background, clear bold heading.
Medical diagram titled "CHRONIC Peritoneal Dialysis - TYPES OVERVIEW" showing a branching tree structure. Main branch splits into two: MANUAL EXCHANGES and AUTOMATED (Cycler-based). Under MANUAL EXCHANGES: CAPD (Continuous Ambulatory PD) - 3 to 5 manual exchanges per day, fluid always present. Under AUTOMATED: APD (Automated PD) as umbrella term, then branches to CCPD (Continuous Cycling PD) - night cycler plus daytime fill, NIPD (Nocturnal Intermittent PD) - night only, dry during day, NTPD (Nightly Tidal PD) - partial drain each cycle, DAPD (Daytime Ambulatory PD) - day exchanges, dry night. Clean medical education style with green color scheme, white background, clear bold heading.
Medical diagram titled "CAPD - Continuous Ambulatory Peritoneal Dialysis" showing step by step process: Step 1 - Dialysate bag (2-3L) connected to catheter, Step 2 - FILL: fluid instilled into peritoneal cavity by gravity (15-20 min), Step 3 - DWELL: solutes diffuse from blood into dialysate across peritoneal membrane (4-8 hours), Step 4 - DRAIN: spent dialysate drained out by gravity into drain bag (20-30 min), Step 5 - Repeat 3-5 times daily. Show simple human torso outline with peritoneal cavity highlighted. Bottom note: No machine needed, patient performs manually, fluid always present 24/7. Blue and orange color scheme, clean medical education style.
Medical diagram titled "APD Types - Automated Peritoneal Dialysis" showing three side-by-side comparison panels for the three main APD types. Panel 1 - CCPD (Continuous Cycling PD): timeline bar showing Night = cycler runs multiple exchanges, Day = final fill left in abdomen (1 daytime exchange optional). Panel 2 - NIPD (Nocturnal Intermittent PD): timeline bar showing Night = cycler runs exchanges, Day = abdomen DRY (no fluid). Note: requires residual kidney function. Panel 3 - NTPD (Nightly Tidal PD): shows partial drain cycles, tidal volume always retained. Each panel has a simple cycler machine icon. Green and purple color scheme, white background, clean medical education style with bold headings.
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.
diagrams please
Medical education diagram titled "ACUTE Peritoneal Dialysis - Indications and Technique". Top section lists indications in colored boxes: AKI (Acute Kidney Injury), Refractory Hyperkalemia, Refractory Metabolic Acidosis, Refractory Volume Overload, Uremic Encephalopathy, Uremic Pericarditis, Toxic Ingestions (methanol, ethylene glycol, salicylates), Resource-limited settings. Bottom section shows technique: Intermittent Peritoneal Dialysis (IPD) - rapid exchanges over 10 to 36 hours every few days. Blue color scheme, white background, bold heading, clean clinical style.
Medical education diagram titled "CHRONIC Peritoneal Dialysis - Classification Tree". Central box at top: Chronic Peritoneal Dialysis. Two main branches below: Left branch "MANUAL" leading to CAPD box (Continuous Ambulatory PD) with description: 3-5 exchanges per day by hand, fluid always present in abdomen, no machine needed. Right branch "AUTOMATED (APD - Cycler-based)" leading to 3 sub-boxes: CCPD (Continuous Cycling PD) - night cycler plus daytime fill; NIPD (Nocturnal Intermittent PD) - night cycler only, dry abdomen in daytime, needs residual kidney function; NTPD (Nightly Tidal PD) - partial drain each cycle, tidal volume retained. Also add IPPD (Intermittent PD) - thrice weekly, older method. Green and teal color scheme, white background, clear arrows, bold labels.
Medical education diagram titled "CAPD - How It Works (Step by Step)". Show a simple human torso outline with peritoneal cavity in center. Four sequential steps arranged in a cycle with arrows: Step 1 FILL - fresh dialysate bag (2-3L) flows by gravity into peritoneal cavity via catheter (15-20 min). Step 2 DWELL - fluid sits in abdomen, waste solutes diffuse from blood vessels in peritoneal membrane into dialysate down concentration gradient, glucose draws water out osmotically (4-8 hours). Step 3 DRAIN - spent cloudy dialysate drains by gravity into drain bag (20-30 min). Step 4 REPEAT - 3 to 5 times daily. Bottom note: Fluid ALWAYS present in abdomen 24 hours a day 7 days a week. Blue and orange colors, white background, clean arrows showing cycle.
Medical education diagram titled "APD Types - Side by Side Comparison". Three panels side by side, each with a 24-hour timeline bar divided into Night (dark blue, 8-10 hours) and Day (light yellow, 14-16 hours). Panel 1 labeled CCPD (Continuous Cycling PD): Night section shows cycler machine icon with multiple exchange arrows (4-6 cycles), Day section shows abdomen with fluid (final fill remains). Note: most common APD type. Panel 2 labeled NIPD (Nocturnal Intermittent PD): Night section shows cycler machine with exchange arrows, Day section shows empty abdomen labeled DRY. Note: Requires residual kidney function. Panel 3 labeled NTPD (Nightly Tidal PD): Night section shows partial fill-drain cycles with tidal volume marker always retained at bottom. Day section shows empty abdomen. Each panel has a cycler machine icon. Purple and green colors, white background, bold panel headings.
plasmapheresis diagram
Medical education diagram titled "PLASMAPHERESIS (Therapeutic Plasma Exchange)" showing the complete process. Central flow diagram: Patient's blood drawn from vein via access catheter → enters separator machine (centrifuge or membrane filter) → blood separates into two components: PLASMA (top, pale yellow, contains antibodies, immune complexes, toxins, paraproteins) and CELLULAR COMPONENTS (bottom, red, red blood cells, white blood cells, platelets) → Plasma is DISCARDED/REMOVED → Cellular components are recombined with REPLACEMENT FLUID (Fresh Frozen Plasma OR Albumin 5%) → Cleaned blood returned to patient via return line. Below the main diagram, two side boxes: Box 1 "INDICATIONS" listing: Myasthenia Gravis, Guillain-Barre Syndrome, Thrombotic Thrombocytopenic Purpura (TTP), Goodpasture Syndrome, ANCA Vasculitis, Anti-GBM disease, Hyperviscosity Syndrome, Acute liver failure. Box 2 "REPLACEMENT FLUIDS" listing: Fresh Frozen Plasma (FFP) - used in TTP, Albumin 5% - used in most other conditions. Bottom note: Typically 1-1.5 plasma volumes exchanged per session, 3-5 sessions per week. Blue and yellow color scheme, white background, clean arrows showing direction of flow, bold headings, clinical style.
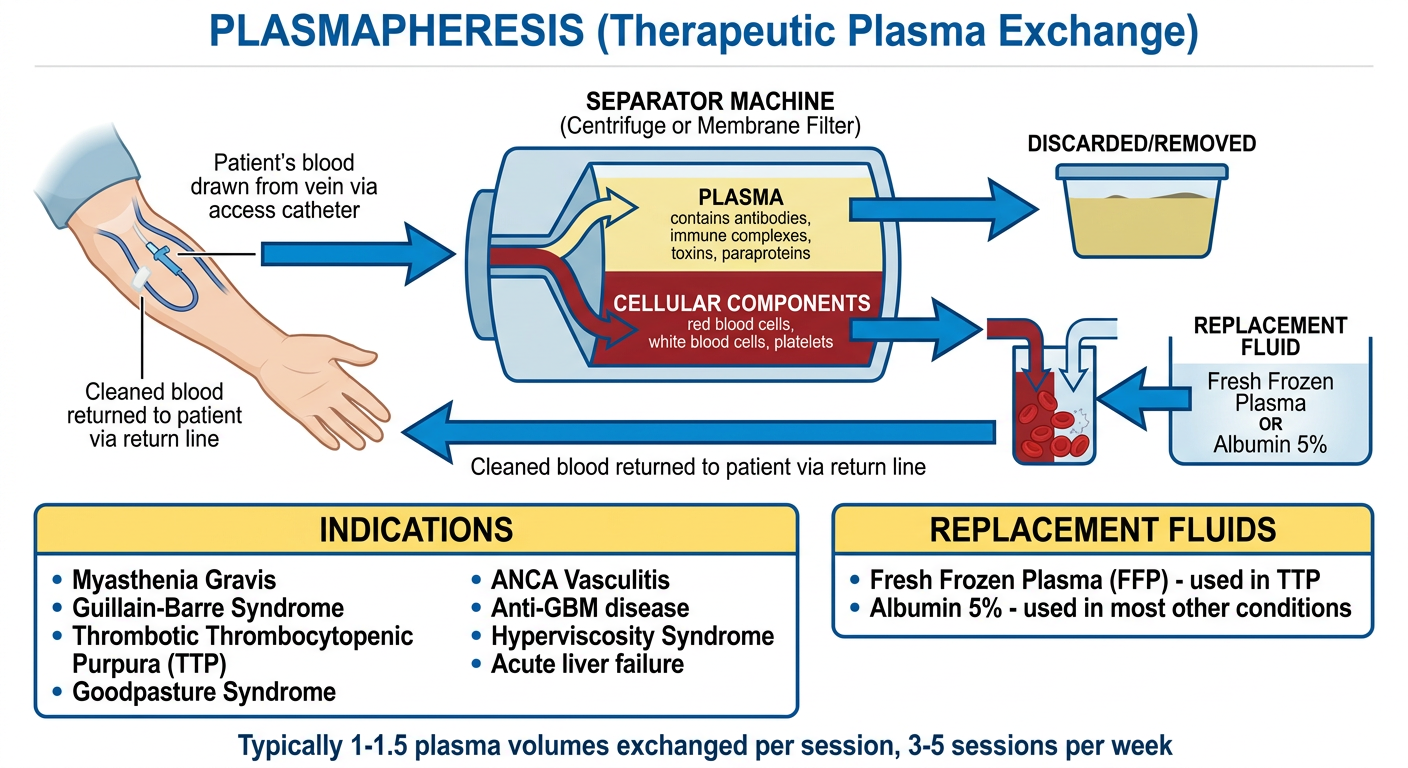
Plasmapheresis (Therapeutic Plasma Exchange) - Key Points
- Centrifugation - spins blood to separate by density
- Membrane filtration - passes blood through a porous filter
| Fluid | Used When |
|---|---|
| Fresh Frozen Plasma (FFP) | TTP (replaces ADAMTS13), coagulopathy |
| Albumin 5% | Most other conditions (cheaper, no infection risk) |
- Thrombotic Thrombocytopenic Purpura (TTP) - first-line treatment
- Guillain-Barre Syndrome
- Myasthenia Gravis (crisis)
- Goodpasture Syndrome / Anti-GBM disease
- ANCA-associated vasculitis
- Hyperviscosity syndrome (myeloma, Waldenstrom's)
- Acute liver failure
plasmapheresis diagram on machine
Detailed medical diagram showing a patient connected to a plasmapheresis machine. On the left side, a patient lying in a hospital bed with two IV lines: one red line (arterial/withdrawal line) coming out of the arm going to the machine, and one blue line (return line) going back into the other arm. In the center, a large plasmapheresis machine with visible components labeled: - Blood pump (peristaltic roller pump) with RPM indicator - Anticoagulant pump (heparin or citrate drip line feeding into the blood line before the separator) - Centrifuge bowl OR membrane plasma filter separator (clearly labeled, showing blood spinning/separating) - Plasma collection bag (pale yellow, labeled "Removed Plasma - contains antibodies, toxins, paraproteins") - Replacement fluid bag hanging on IV pole (labeled "FFP or 5% Albumin") - Air detector and pressure monitors on tubing - Return line mixing replaced fluid with cellular components before going back to patient Color coding: Red tubing = blood going out, Yellow tubing = plasma being removed, Blue tubing = return blood going back. Arrows showing direction of flow throughout. Labels on all components. Title at top: "PLASMAPHERESIS CIRCUIT - Machine Setup". White background, clean technical medical illustration style, realistic machine appearance.
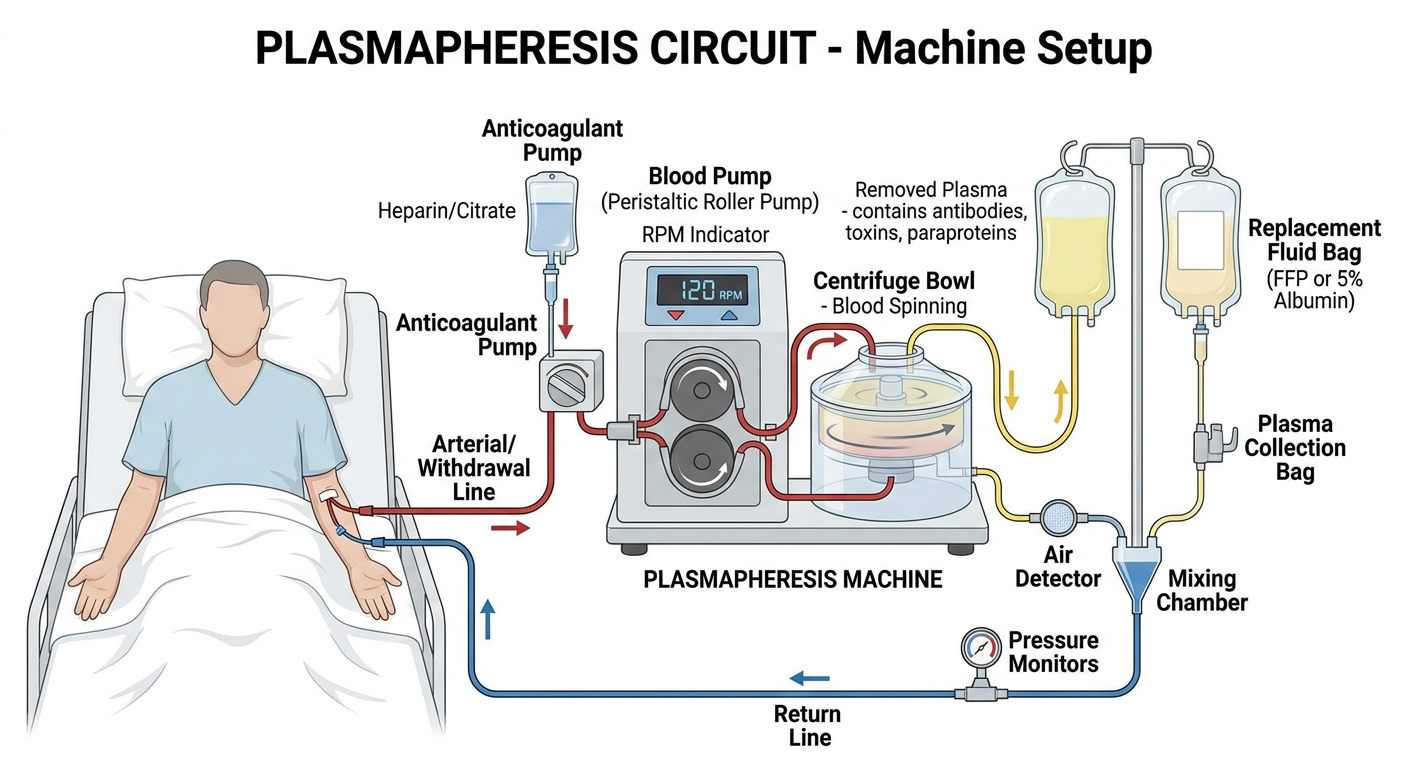
Machine Circuit - Step by Step Flow
- Blood drawn from patient via central venous catheter or large peripheral IV
- Anticoagulant (heparin or citrate) is added to the line immediately to prevent clotting in the circuit
- Peristaltic roller pump drives blood through the circuit at a controlled rate (~50-150 mL/min)
- Centrifuge method - spins blood in a bowl; cells (heavy) settle outward, plasma (light) rises and is skimmed off
- Membrane filter method - blood passes through a porous hollow-fibre membrane; plasma is filtered out, cells cannot pass
- Separated plasma is collected into a waste bag
- This plasma carries the pathological load: autoantibodies, immune complexes, toxins, paraproteins, cryoglobulins
- FFP (for TTP - replaces missing ADAMTS13) or 5% Albumin (for most other indications) is infused into the return line
- Cellular components + replacement fluid are mixed and returned to the patient via the return line
cvvhdf machine ,cvvhd ,cvvh, hd , sled, scuf , crrt ,hemoperfusion ,mars machine diagrams along with patient
Detailed medical diagram titled "CVVH - Continuous Veno-Venous Hemofiltration" showing patient in ICU bed connected to machine. Circuit: Blood withdrawn from double-lumen central venous catheter (jugular or femoral). Red line goes to blood pump (peristaltic roller). Then through a large hemofilter (hollow fiber membrane). No dialysate used. Pre-filter or post-filter replacement fluid bag (labeled "Replacement Fluid - Bicarbonate based") infuses into circuit. Ultrafiltrate (waste fluid, yellow line) drains into collection bag. Cleaned blood (blue line) returns to patient. Labels: Blood pump, Hemofilter, Replacement fluid pump, Ultrafiltrate collection bag, Anticoagulant (heparin/citrate) pump. Mechanism note box: "Convection only - solutes dragged with water through membrane pores (solvent drag)". Flow rate: 25-35 mL/kg/hr. White background, red/blue/yellow color coded tubing, clean ICU style.
Detailed medical diagram titled "CVVHD - Continuous Veno-Venous Hemodialysis" showing patient in ICU bed connected to machine. Circuit: Blood withdrawn from double-lumen central venous catheter. Red line to blood pump then through hemofilter. Dialysate fluid bag (green line) flows counter-current OPPOSITE to blood flow direction through dialysate compartment of filter. Spent dialysate exits into waste bag (green dashed line). NO replacement fluid bag. Blue return line back to patient. Labels: Blood pump, Hemofilter, Dialysate pump IN, Spent dialysate OUT (counter-current arrow emphasized), Anticoagulant pump. Mechanism note box: "Diffusion only - solutes move down concentration gradient from blood into dialysate. Counter-current flow maximizes gradient." White background, red/blue/green color coded tubing, clean clinical diagram style.
Detailed medical diagram titled "CVVHDF - Continuous Veno-Venous Hemodiafiltration" showing patient in ICU bed connected to machine. Circuit: Blood withdrawn from double-lumen central venous catheter. Red line to blood pump then through large hemofilter. TWO inputs to filter: 1) Dialysate bag (green line) flowing counter-current through dialysate side, 2) Replacement fluid bag (orange line) infusing pre or post filter into blood circuit. Ultrafiltrate/spent dialysate exits into waste bag. Blue return line to patient. Labels: Blood pump, Hemofilter, Dialysate pump, Replacement fluid pump, Waste/ultrafiltrate bag, Anticoagulant pump. Mechanism note box: "BOTH Diffusion AND Convection - combines CVVHD plus CVVH. Best clearance of small AND middle molecules." White background, color-coded tubing, arrows showing direction of flow throughout, clean ICU diagram.
Detailed medical diagram titled "Intermittent Hemodialysis (IHD)" showing patient sitting in dialysis chair connected to hemodialysis machine. Circuit: Blood from arteriovenous fistula in forearm (or central catheter) via two needles (arterial and venous). Red arterial line to blood pump on machine. Blood flows through dialyzer (parallel plate or hollow fiber). Dialysate (bicarbonate based) flows COUNTER-CURRENT from dialysate preparation system through dialyzer. Spent dialysate drains to drain. Cleaned blood returns via blue venous line to patient's fistula. Machine components labeled: Blood pump, Dialyzer, Dialysate proportioning system, Air trap/bubble detector, Pressure monitors, Heparin pump, Temperature monitor, Conductivity monitor. Note box: "3-4 hours per session, 3x per week. Intermittent. High efficiency." White background, clean clinical diagram, red/blue color coded lines.
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.
cvvhdf ,cvvhd ,cvvh, hd , sled, scuf , crrt machine diagrams along with patient
Detailed medical diagram titled "CVVH - Continuous Veno-Venous Hemofiltration" showing ICU patient in bed connected to CRRT machine. Blood withdrawal from double-lumen central venous catheter in neck. RED line (blood out) goes through peristaltic blood pump, then through hollow fiber hemofilter. POST-filter replacement fluid bag (labeled Bicarbonate Replacement Fluid) infuses into circuit via replacement pump. YELLOW ultrafiltrate waste line drains from filter into waste bag. BLUE line (clean blood) returns to patient catheter. Anticoagulant (heparin or citrate) syringe pump on access line. All components labeled with arrows showing flow direction. Mechanism box: CONVECTION ONLY - solvent drag pulls solutes through membrane pores. Clearance: 25-35 mL/kg/hr. No dialysate used. White background, color coded tubing, clean clinical style.
Detailed medical diagram titled "CVVHD - Continuous Veno-Venous Hemodialysis" showing ICU patient in bed connected to CRRT machine. Blood withdrawal from double-lumen central venous catheter. RED blood line goes through blood pump then into hollow fiber hemofilter (blood side). GREEN dialysate line flows COUNTER-CURRENT (opposite direction to blood) through dialysate side of same filter from dialysate bag. Spent dialysate (green dashed line) exits filter into effluent/waste bag. NO replacement fluid bag present. BLUE clean blood return line back to patient catheter. Anticoagulant pump on access line. All components labeled: Blood pump, Hemofilter, Dialysate pump, Effluent bag, Counter-current arrow emphasized with label. Mechanism box: DIFFUSION ONLY - solutes move down concentration gradient from blood into dialysate across membrane. Best for small molecules urea creatinine. White background, color coded tubing.
kidney diagram