Answer with diagrams and all the necessary details
Asking for Preferences
Describe in detail the MAMMARY GLAND under the following headings: a. Extent b. Relations c. Structure d. Blood Supply e. Lymphatic drainage f. Applied Anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content and diagrams needed. Let me compile the comprehensive answer.
The Mammary Gland - Detailed Description
Sources: Gray's Anatomy for Students (9780323934237), Creasy & Resnik's Maternal-Fetal Medicine (9780323828499), Histology: A Text and Atlas (9781975181512)
a. Extent
The mammary gland is a modified sweat gland situated in the superficial fascia of the pectoral region, anterior to the thoracic wall. It lies between skin and the deep pectoral fascia, from which it is separated by the retromammary space - a layer of loose connective tissue that allows limited mobility.
Vertical extent: Rib II (2nd rib) to Rib VI (6th rib)
Horizontal extent: Lateral border of the sternum to the midaxillary line
Nipple position: At the center of the areola, typically at the level of the 4th intercostal space, just below the midclavicular line
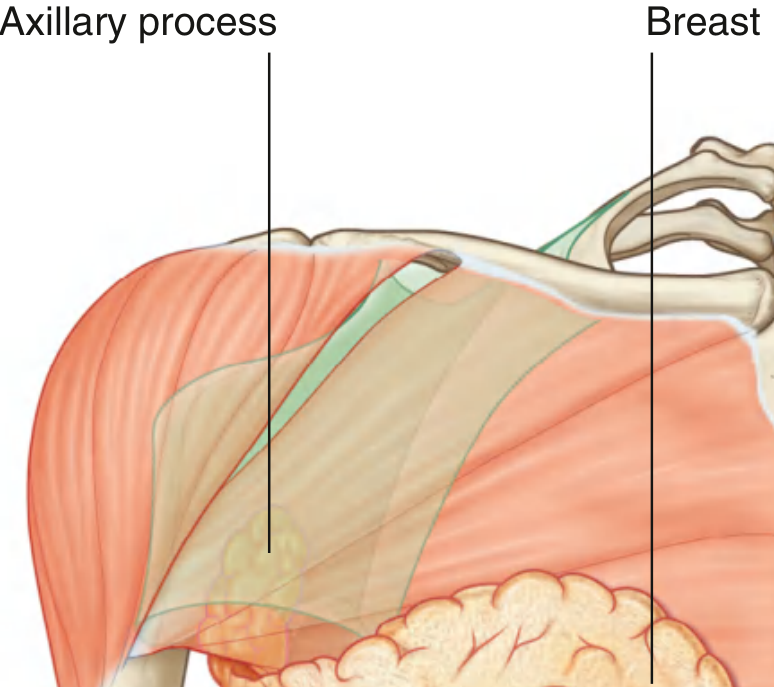
Axillary (Spence's) Tail: The superolateral region of the breast extends along the inferior margin of pectoralis major toward the axilla. In some individuals, it passes around the margin of the muscle, perforates the deep fascia, and enters the axilla - though it rarely reaches the apex of the axilla.
b. Relations
Anterior
- Skin with overlying superficial fascia
- Nipple and areola at the 4th intercostal space level
Posterior (Deep surface)
- Retromammary space (loose connective tissue) - allows the breast to slide on underlying structures
- Deep (pectoral) fascia covering pectoralis major (medially), serratus anterior (laterally), and external oblique/rectus abdominis (inferiorly)
Superior
- Clavicle
- Branches of the supraclavicular nerves
Inferior
- Upper anterior abdominal wall
Medial
- Sternum
Lateral
- Axilla (with the axillary tail projecting into it)
Muscles related to the breast:
| Position | Muscle |
|---|---|
| Central/medial deep | Pectoralis major |
| Lateral deep | Serratus anterior |
| Inferolateral deep | External oblique |
| Inferomedial | Rectus abdominis |
c. Structure
The mammary gland is a compound tubuloalveolar gland derived from modified sweat glands of the ectoderm.
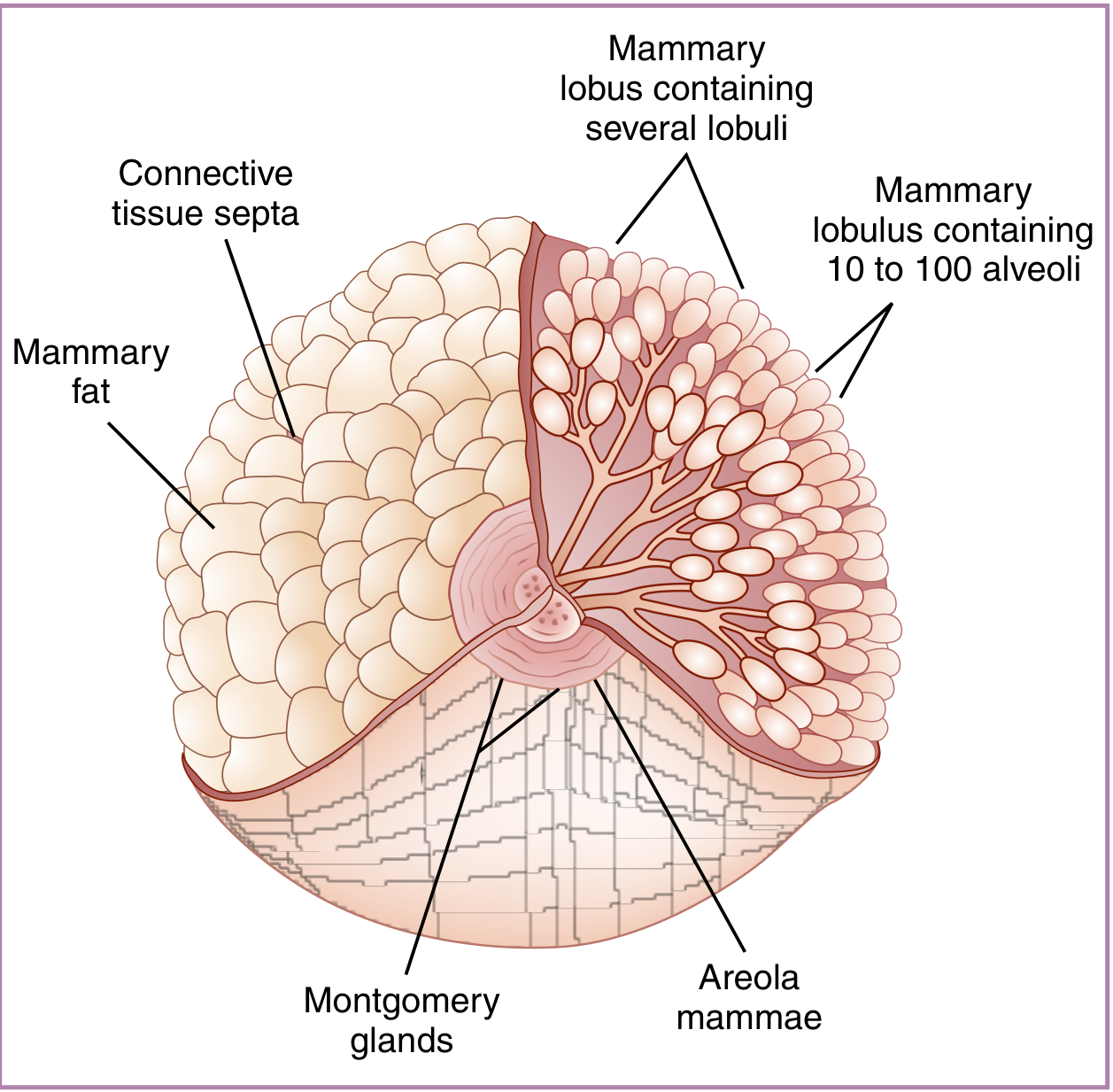
Parenchyma (Glandular tissue)
- 15-20 lobes arranged radially around the nipple, separated by connective tissue septa (Cooper's ligaments)
- Each lobe contains several lobules
- Each lobule contains 10-100 alveoli (secretory units)
- Each lobe drains via a lactiferous duct that opens independently at the nipple tip
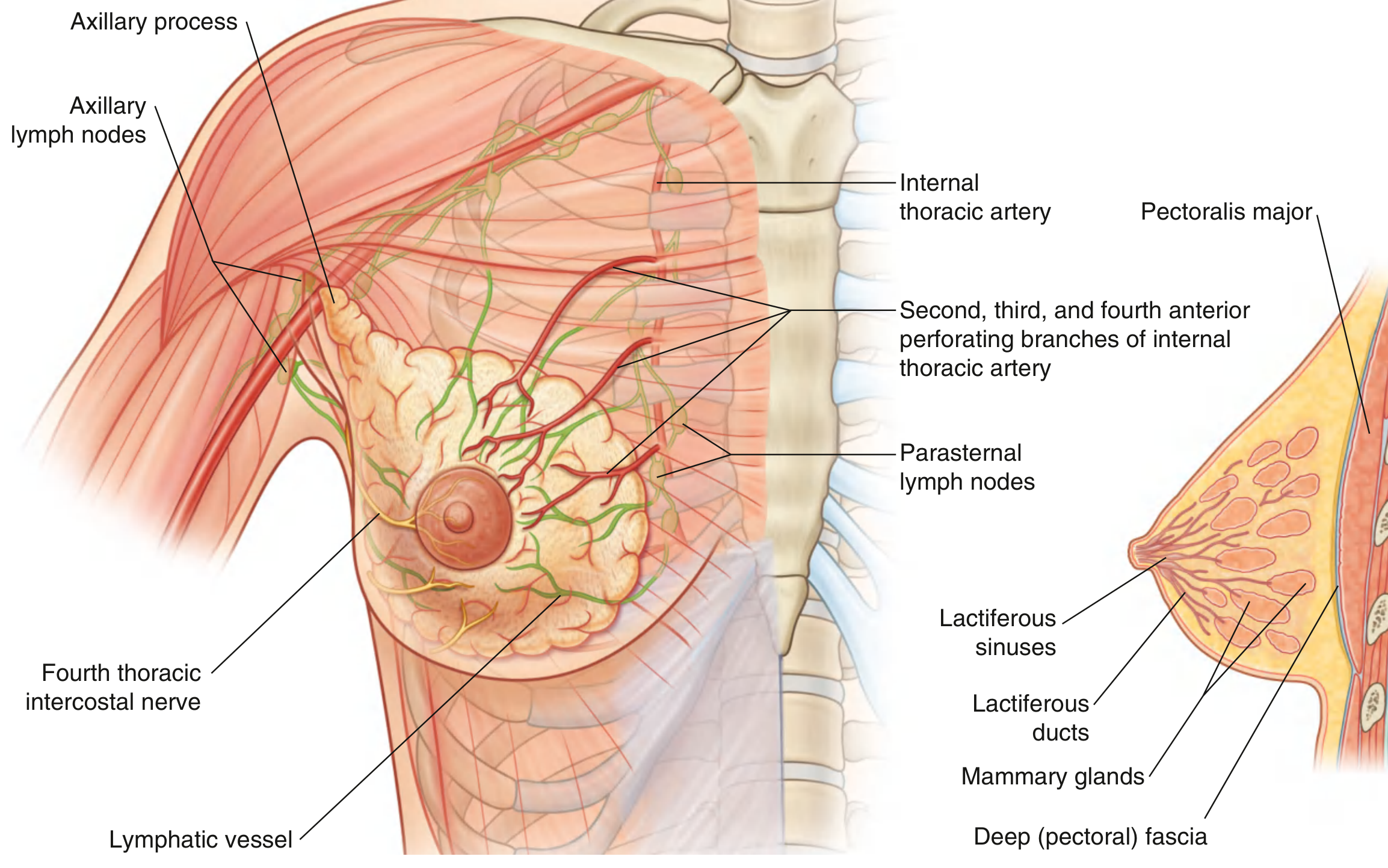
- Just before opening at the nipple, each lactiferous duct dilates into a lactiferous sinus (ampulla), which acts as a temporary reservoir for milk
Stroma
- Dense irregular connective tissue (interlobular) and loose connective tissue (intralobular)
- Cooper's (Suspensory) Ligaments: Fibrous bands that extend from the dermis of the skin to the deep fascia, providing structural support. Distortion or shortening of these by carcinoma produces characteristic skin dimpling
- Adipose tissue: The predominant component in non-lactating women; fat surrounds the glandular elements and gives the breast its smooth, rounded contour
Nipple and Areola
- Nipple: Conical elevation at the center of the areola; contains smooth muscle fibers (erectile), richly innervated with sensory and pain fibers; contains 4-18 lactiferous duct openings (5-8 main ducts)
- Areola: Circular pigmented zone (avg. 15-16 mm diameter, enlarges in pregnancy); contains Montgomery glands (modified sebaceous/sweat glands) that hypertrophy during pregnancy and lactation to lubricate and protect the nipple
- Verrucous surface of nipple; has sebaceous and apocrine sweat glands but no hair
Histological Stages
| Stage | Features |
|---|---|
| Inactive (resting) | Sparse parenchyma; mainly ducts; intralobular loose CT + interlobular dense CT with adipocytes; alveoli absent (represented as cellular thickenings) |
| Pregnant/Lactating | Extensive alveolar proliferation; alveoli lined by cuboidal secretory and myoepithelial cells; lipid droplets in cells; reduced stroma |
| Post-weaning (Involution) | Alveoli regress; gland returns to near-resting state |
In males
- Rudimentary breast consisting of small ducts (often cords of cells) that do not extend beyond the areola
d. Blood Supply
The breast has a rich, multi-source blood supply reflecting its dual anatomical relationship with both the thoracic wall and upper limb.
Arterial Supply
| Source | Contribution |
|---|---|
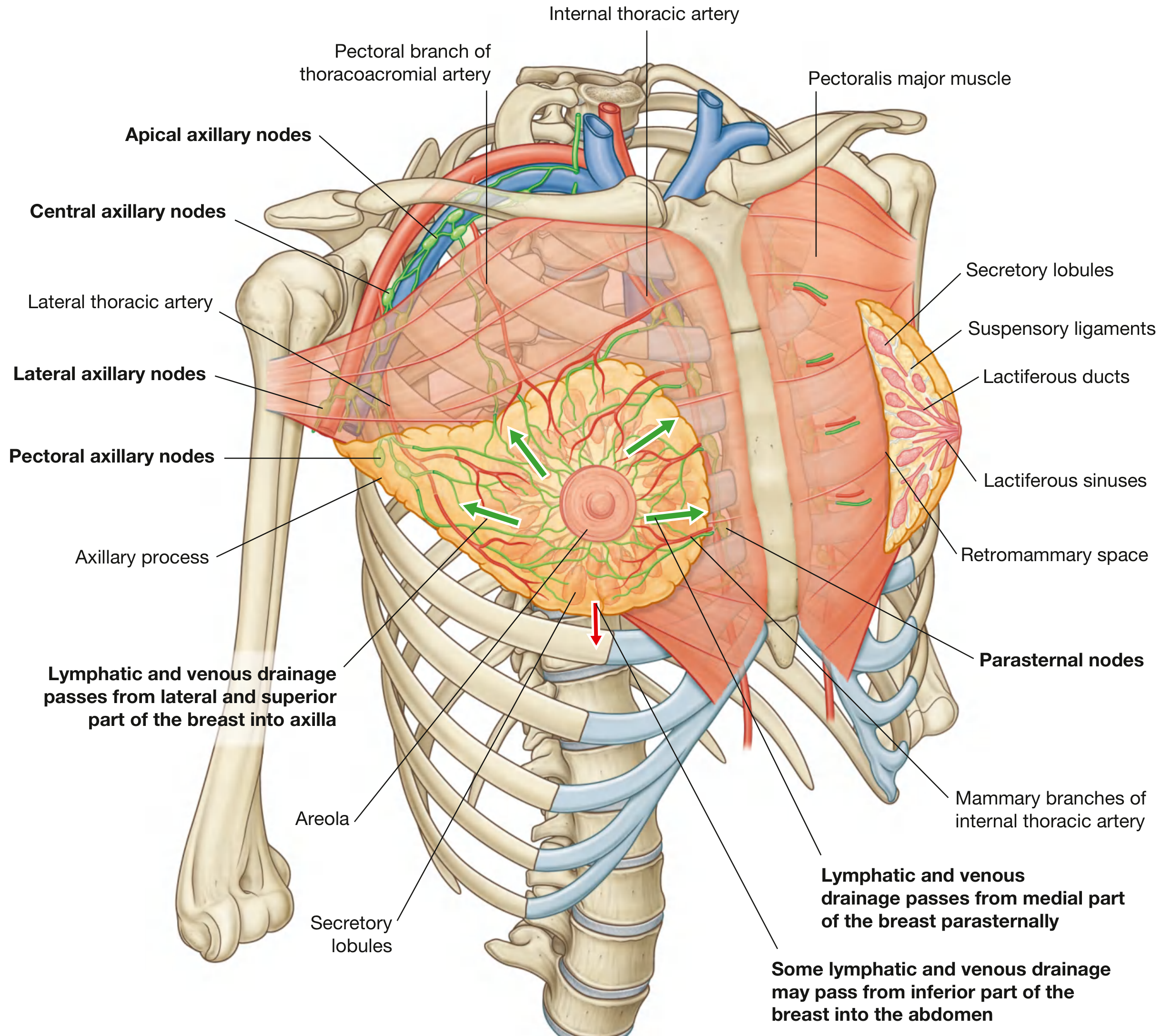
| Internal thoracic artery (internal mammary artery) - perforating branches (2nd-4th spaces) | Anteromedial breast (major supply ~60%) |
| Lateral thoracic artery (branch of axillary artery) | Lateral and superior breast |
| Thoracoacromial artery - pectoral branch | Superior breast |
| Superior thoracic artery (branch of axillary artery) | Superior breast |
| Subscapular artery (branch of axillary artery) | Lateral breast |
| Anterior intercostal arteries (2nd-4th branches) | Lateral perforating branches |
| Posterior intercostal arteries (2nd-5th) | Deep breast tissue |
The internal mammary artery and lateral thoracic artery are the primary sources of blood supply.
Venous Drainage
Veins follow a pattern parallel to the arteries and drain into:
- Internal thoracic (mammary) vein - anteromedially
- Axillary vein - laterally and superiorly
- Intercostal veins - posteriorly and inferiorly
Note: The intercostal veins connect with the vertebral venous plexus (Batson's plexus), providing a route for haematogenous metastasis of breast cancer to the vertebral column, skull, and pelvis - without going through the pulmonary circulation.
Innervation
- Anterior and lateral cutaneous branches of the 2nd-6th intercostal nerves
- Nipple: specifically innervated by the 4th intercostal nerve
- Efferent nerves are sympathetic adrenergic; no parasympathetic or cholinergic supply
- Sensory stimulation of nipple/areola triggers release of prolactin (adenohypophysis) and oxytocin (neurohypophysis)
e. Lymphatic Drainage
Lymphatic drainage is of paramount clinical importance due to its role in the spread of breast carcinoma. The lymphatics of the breast originate in lymph capillaries of the mammary connective tissue.
Primary Drainage Routes
1. Axillary Route (~75% of total drainage)
- Drains the lateral, superior, and central parts of the breast
- Drains into the axillary lymph nodes, which are divided into 5 groups:
| Group | Location | Receives from |
|---|---|---|
| Pectoral (anterior) | Along lateral thoracic vessels | Most of anterior chest wall, most of the breast |
| Subscapular (posterior) | Along subscapular vessels | Posterior thoracic wall, posterior shoulder |
| Humeral (lateral) | Along axillary vein | Upper limb (arm) |
| Central | Embedded in axillary fat | Pectoral, subscapular, humeral groups |
| Apical | Most superior, medial to pectoralis minor | All other axillary groups + superior breast; drains via subclavian trunk |
Efferent pathway: Apical nodes → Subclavian trunk → Joins subclavian vein at junction with internal jugular vein (right side) or joins thoracic duct (left side)
2. Parasternal (Internal Mammary) Route (~20-25%)
- Drains the medial and central parts of the breast
- Lymphatics accompany perforating branches of the internal thoracic artery
- Drain into parasternal (internal mammary) nodes along the internal thoracic vessels on the deep surface of the anterior thoracic wall
- Parasternal nodes drain into the bronchomediastinal trunks
3. Intercostal Route (minor)
- Some drainage from the posterior and inferior breast
- Via lymphatics that follow lateral branches of posterior intercostal arteries
- Drain into intercostal nodes near the heads and necks of ribs
- Intercostal nodes drain into the thoracic duct or bronchomediastinal trunks
4. Inferior (Subdiaphragmatic) Route
- Small amount of drainage from the inferior breast
- May communicate with subdiaphragmatic lymphatics and hepatic lymphatics (via the falciform ligament)
Summary Diagram (Lymphatic Routes)
BREAST LYMPHATIC DRAINAGE
|
┌───────────────┼───────────────┐
▼ ▼ ▼
AXILLARY (~75%) PARASTERNAL INTERCOSTAL
(lateral/sup.) (~20-25%) (minor, post.)
| (medial) |
Pectoral nodes Parasternal Intercostal
→ Subscapular nodes nodes
→ Humeral | |
→ Central Bronchomediastinal Thoracic duct /
→ Apical trunk Bronchomediastinal
| trunk
Subclavian trunk
|
Venous junction
(subclavian + IJ vein)
f. Applied Anatomy
1. Breast Carcinoma
Breast cancer is one of the most common malignancies in women. It arises from:
- Acini (terminal duct lobular units - TDLU) - lobular carcinoma
- Lactiferous ducts - ductal carcinoma (most common)
Spread routes:
- Lymphatic: To axillary nodes (most common), parasternal nodes, supraclavicular nodes, and contralateral breast
- Haematogenous: Via Batson's vertebral venous plexus (through intercostal veins) → vertebral column, skull, pelvis; or via axillary/internal thoracic veins → lungs, liver, bone
- Direct invasion: Into pectoral muscles, chest wall, skin
Staging requires:
- Size of primary tumor
- Exact site
- Number and sites of lymph node spread
- Distant metastasis (lungs, liver, bone - detected by CT, bone scan, PET-CT)
2. Skin Changes in Carcinoma
| Sign | Mechanism |
|---|---|
| Skin dimpling / pitting | Carcinoma invades and shortens Cooper's (suspensory) ligaments |
| Peau d'orange (orange-peel appearance) | Lymphatic obstruction causes skin oedema; hair follicles tethered to skin produce pitting |
| Nipple retraction / inversion | Carcinoma invades and shortens the lactiferous ducts |
| Nipple discharge | Intraductal carcinoma or Paget's disease |
3. Lymphoedema After Mastectomy
- Axillary lymph node clearance (ALND) or radiotherapy to the axilla disrupts lymphatic drainage of the upper limb
- Results in chronic lymphoedema of the arm (brawny, non-pitting oedema)
- Clinicians now favor sentinel lymph node biopsy (SLNB) to reduce this complication
4. Sentinel Lymph Node Biopsy (SLNB)
- The sentinel node is the first lymph node to receive lymphatic drainage from the primary tumor
- Identified by injecting blue dye or radioactive tracer around the tumor
- If sentinel node is clear of metastasis, full axillary clearance is avoided
- Reduces risk of lymphoedema significantly
5. Axillary Tail (Spence's Tail)
- Clinicians must examine the axillary tail when assessing breast lumps; pathology (carcinoma, fibroadenoma) can occur in this extension
- It may be mistaken for an axillary lymph node
6. Mammography
- The primary imaging modality for breast cancer screening
- Uses low-dose X-rays; the breast is compressed between plates
- Can detect microcalcifications (early sign of ductal carcinoma in situ - DCIS) and soft tissue masses
7. Paget's Disease of the Nipple
- Eczema-like change of the nipple/areola due to underlying intraductal carcinoma
- Paget's cells (large clear cells) invade the nipple epidermis
- Associated with subjacent ductal carcinoma in situ (DCIS) or invasive ductal carcinoma
8. Gynaecomastia
- Benign proliferation of male breast glandular tissue
- Can occur physiologically (neonatal, pubertal, elderly) or due to hormone imbalance, drugs (spironolactone, digitalis, cimetidine, exogenous estrogens), liver cirrhosis, or testicular tumors (hCG-secreting)
9. Supernumerary Breasts / Nipples (Polymastia / Polythelia)
- Due to failure of involution of the milk line (mammary ridge - a bilateral ectodermal thickening extending from axilla to groin during fetal development)
- Accessory nipples most commonly appear along the milk line, particularly below and medial to the normal breast
10. Abscess of the Breast
- Most common during lactation (puerperal mastitis)
- Superficial abscess: In the subcutaneous tissue; drains anteriorly
- Deep (retromammary) abscess: In the retromammary space; presents with deep fluctuance; may point inferiorly
Sources: Gray's Anatomy for Students, p. 168-176; Creasy & Resnik's Maternal-Fetal Medicine, p. 242-244; Histology: A Text and Atlas, p. 2361
This is a shared conversation. Sign in to Orris to start your own chat.