Seizure detail and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"seizure" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compose the full response.
Seizures: Detail and Management
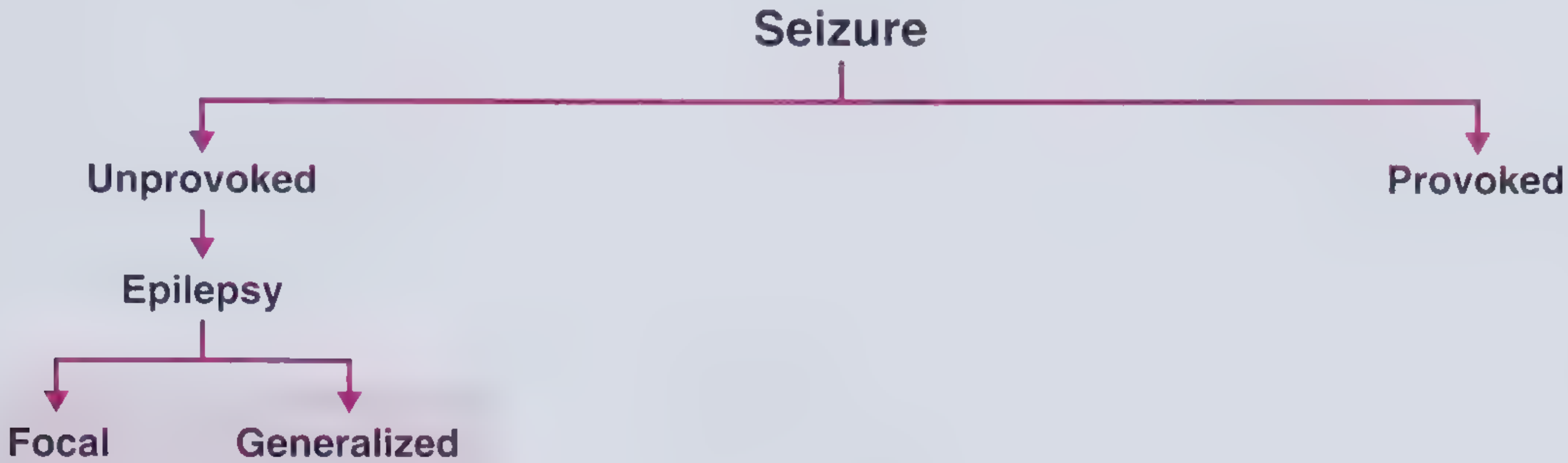
1. Definitions
| Term | Definition |
|---|---|
| Seizure | A transient occurrence of signs/symptoms due to abnormal excessive or synchronous neuronal activity in the brain |
| Provoked (Acute symptomatic) seizure | Occurs in close temporal relationship with an acquired precipitating condition (metabolic, toxic, structural, infectious) |
| Unprovoked seizure | Occurs in the absence of a temporary or reversible precipitant |
| Epilepsy | At least 2 unprovoked seizures >24 hours apart, OR 1 unprovoked seizure with ≥60% risk of recurrence over 10 years |
Recurrence risk:
-
After 1 unprovoked seizure: ~40-50% risk of a second within 2-8 years
-
After 2 unprovoked seizures: ~60-90% risk of a third within 4 years
-
Frameworks for Internal Medicine, p. 559
2. ILAE 2017 Classification of Seizure Types
(Source: Katzung's Basic and Clinical Pharmacology, 16th Edition)
Focal Onset Seizures (formerly Partial)
| Type | Key Feature |
|---|---|
| Focal aware (formerly simple partial) | Consciousness preserved |
| Focal impaired awareness (formerly complex partial) | Consciousness impaired |
| Focal-to-bilateral tonic-clonic (formerly secondarily generalized) | Starts focally, spreads to both hemispheres |
Generalized Onset Seizures
| Type | Notes |
|---|---|
| Tonic-clonic (grand mal) | Most dramatic; tonic phase (10-20s) then clonic phase; postictal confusion |
| Absence (petit mal) | 10-15s stare, abrupt onset/offset, no postictal state; age 5-15y |
| Myoclonic | Brief jerks; e.g., juvenile myoclonic epilepsy |
| Atonic (drop attacks) | Sudden loss of muscle tone; e.g., Lennox-Gastaut |
| Epileptic spasms | e.g., West syndrome (infantile spasms) |
3. Seizure Types in Detail
Absence Seizures
- Onset age 5-15 years; family history in 20-40% of patients
- Abrupt behavioral arrest, no warning, no postictal phase, usually 10-15 seconds (up to 40s)
- Simple absence: altered consciousness only
- Complex absence: altered consciousness + eyelid flutter, minor automatisms, autonomic changes (pallor, tachycardia, urinary incontinence)
- Office diagnosis: hyperventilate for 3-4 minutes often induces an episode
- Bradley and Daroff's Neurology, p. 38
Tonic-Clonic Seizures
- No warning/aura in primary generalized form
- Tonic phase (10-20 s): sustained muscle contraction; apnea, cyanosis, hypertension, incontinence possible
- Clonic phase: rhythmic synchronous muscle jerking
- Postictal: prolonged lethargy, confusion, somnolence, may have pathologically brisk reflexes
- Injury from falls, shoulder dislocation, tongue biting
- Bradley and Daroff's Neurology, p. 38
Focal Seizures
- Manifestations depend on the brain region involved:
- Frontal lobe: tonic posturing, complex motor automatisms
- Temporal lobe: lip smacking, oral/alimentary automatisms, fear, deja vu
- Parietal lobe: contralateral paresthesia
- Occipital lobe: visual symptoms (flashes, scotoma)
- Jacksonian march: motor spread along contiguous motor cortex
- Todd's paralysis: transient postictal weakness in the region affected by a focal motor seizure
- Frameworks for Internal Medicine, p. 561
Provoked Seizure Causes (mnemonic: VITAMINS)
- Vascular: stroke, hypertensive encephalopathy, PRES, cerebral venous thrombosis
- Infectious: meningitis, encephalitis, brain abscess
- Toxic/drug-related: alcohol withdrawal, cocaine, bupropion, isoniazid, theophylline
- Autoimmune/Inflammatory: anti-NMDA receptor encephalitis, lupus cerebritis
- Metabolic: hypo/hypernatremia, hypoglycemia, hypocalcemia, hypomagnesemia, hepatic/uremic encephalopathy
- Idiopathic/Structural: tumors, head trauma, AVM
- Neoplastic
4. Workup
| Investigation | Purpose |
|---|---|
| Blood glucose (bedside) | Exclude hypoglycemia immediately |
| Electrolytes (Na, Ca, Mg), BUN, creatinine | Metabolic causes |
| CBC, LFTs | Infection, hepatic failure |
| Toxicology screen (urine/blood) | Toxic precipitant |
| AED drug levels | Subtherapeutic in known epileptics |
| Prolactin (drawn 10-20 min post-seizure) | May help distinguish true GTC from pseudoseizure (not always reliable) |
| EEG | Confirms epileptiform activity; identifies seizure type/focus |
| MRI brain (preferred over CT) | Structural lesion, cortical dysplasia, mesial temporal sclerosis |
| LP | If CNS infection suspected |
5. Chronic Pharmacologic Management (Anti-Seizure Medications)
First-Line Agents by Seizure Type
| Seizure Type | First-Line Drug(s) |
|---|---|
| Focal (partial) | Carbamazepine, lamotrigine, levetiracetam, oxcarbazepine |
| Generalized tonic-clonic | Valproate, lamotrigine, levetiracetam |
| Absence | Ethosuximide, valproate |
| Myoclonic | Valproate, levetiracetam, clonazepam |
| Atonic | Valproate, lamotrigine, clonazepam |
Common Agent Summary
| Drug | Starting Dose | Key Adverse Effects |
|---|---|---|
| Carbamazepine | 200 mg BID, increase 200 mg/day weekly (max 1000 mg/day) | Drowsiness, diplopia, benign leukopenia, rare aplastic anemia, SIADH |
| Valproate (divalproex) | 10-15 mg/kg/day | Weight gain, alopecia, tremor, hepatotoxicity, teratogen (neural tube defects) - AVOID in pregnancy |
| Lamotrigine | Titrate slowly (risk of Stevens-Johnson) | Rash (including SJS if titrated too fast), dizziness |
| Levetiracetam | 500 mg BID | Behavioral changes (irritability, depression), otherwise well tolerated |
| Phenytoin | 300-400 mg/day | Nystagmus, ataxia, gum hyperplasia, hirsutism, zero-order kinetics - narrow therapeutic index |
| Phenobarbital | Oldest agent | Sedation, cognitive impairment, hyperactivity in children |
| Ethosuximide | Absence only | GI upset, headache |
Key prescribing principles:
-
Try monotherapy first; combine only after multiple monotherapy failures
-
Seizure control + side effects matter more than drug levels alone
-
Levetiracetam and lamotrigine are safest in pregnancy (valproate is contraindicated)
-
Textbook of Family Medicine, 9e, p. 1229-1230; Katzung's Basic and Clinical Pharmacology, 16th Edition
6. Non-Pharmacologic Treatment
-
Lifestyle: avoid sleep deprivation, limit alcohol, identify/avoid triggers (flashing lights, hyperventilation, stress, fever, certain drugs)
-
Epilepsy surgery: temporal lobe resection is the most common (for mesial temporal lobe epilepsy); cortical resection for lesion-associated focal epilepsy
-
Vagus nerve stimulator (VNS): for drug-refractory focal seizures; continuous open-loop stimulation
-
Responsive neurostimulator (RNS): closed-loop device; detects abnormal EEG pattern and delivers stimulation
-
Deep brain stimulation (DBS): bilateral anterior nuclei of thalamus; adjunctive for focal seizures
-
Ketogenic diet: high-fat, low-carbohydrate; effective especially in pediatric refractory epilepsy
-
Katzung's Basic and Clinical Pharmacology, 16th Edition
7. Status Epilepticus (SE)
Definition: >30 minutes of continuous or recurrent seizure activity without recovery of consciousness (functionally, treat after 5 minutes of active seizure)
Time-sensitive emergency - delays in benzodiazepines >10 minutes increase mortality, duration, and complications.
Step-by-Step Management Protocol
┌────────────────────────────────────────────────────────────┐
│ 0-5 min: STABILIZE │
│ • Airway: position, O2, suction; nasopharyngeal airway │
│ • Monitoring: HR, BP, SpO2, temperature │
│ • IV/IO access; blood glucose (give D50 if hypoglycemic) │
│ • Labs: electrolytes, glucose, Ca, Mg, CBC, LFTs, │
│ tox screen, AED levels │
│ • Correct metabolic abnormalities │
└────────────────────────────────────────────────────────────┘
▼
┌────────────────────────────────────────────────────────────┐
│ 5 min: FIRST-LINE - Benzodiazepines │
│ • Lorazepam IV 0.1 mg/kg (max 4 mg) - PREFERRED │
│ OR Diazepam IV 0.15-0.2 mg/kg │
│ • If no IV: intranasal/buccal/IM midazolam │
│ (IM midazolam 10 mg for adults ≥40 kg) │
│ • Terminate seizure in ~70% of cases │
└────────────────────────────────────────────────────────────┘
▼ (if seizure continues at 5 min after 1st BZD)
┌────────────────────────────────────────────────────────────┐
│ Repeat benzodiazepine (second dose) │
└────────────────────────────────────────────────────────────┘
▼ (if seizure continues 5 min after 2nd BZD)
┌────────────────────────────────────────────────────────────┐
│ SECOND-LINE (equal efficacy): │
│ • Levetiracetam IV 60 mg/kg (max 4500 mg) │
│ • Fosphenytoin IV 20 mg PE/kg (max 1500 mg PE) │
│ - Water-soluble, IM-compatible, less cardiotoxic │
│ than phenytoin │
│ • Valproic acid IV 40 mg/kg (max 3000 mg) │
│ - Avoid in liver disease, thrombocytopenia, │
│ suspected metabolic disease │
└────────────────────────────────────────────────────────────┘
▼ (if refractory)
┌────────────────────────────────────────────────────────────┐
│ REFRACTORY SE - Intubation + ICU │
│ • Propofol, midazolam, or pentobarbital infusion │
│ • Consider ketamine (case report evidence) │
│ • Continuous EEG monitoring essential │
└────────────────────────────────────────────────────────────┘
Fosphenytoin vs Phenytoin: Fosphenytoin is 3x faster to administer, IM-compatible, less sclerosing, and substantially less cardiotoxic - prefer over phenytoin when available.
- Rosen's Emergency Medicine, p. 169
8. Special Situations
| Scenario | Key Point |
|---|---|
| First unprovoked seizure | AED not mandatory; weigh recurrence risk vs. side effects; restrict driving |
| Alcohol withdrawal seizures | Benzodiazepines (treat the withdrawal); phenytoin NOT effective for this cause |
| Febrile seizures in children | Usually self-limited; <15 min simple febrile seizure has excellent prognosis |
| Pregnancy | Levetiracetam + lamotrigine safest; valproate contraindicated; monitor drug levels closely (volume of distribution increases) |
| Post-cardiac arrest | No prophylactic AEDs; treat seizures/SE aggressively; continuous EEG for NCSE |
| TBI | 7 days of levetiracetam 500 mg BID for early seizure prophylaxis only; no long-term benefit shown |
| ICH | Prophylactic AEDs associated with worse outcomes; do NOT routinely recommend |
9. When to Refer to Neurology
- Any first unprovoked seizure (for EEG/MRI workup)
- Seizures not controlled after 2 monotherapy trials
- Consideration of epilepsy surgery
- Pregnancy in a known epileptic
- Suspected epilepsy syndrome (e.g., juvenile myoclonic epilepsy, Lennox-Gastaut)
Sources:
- Frameworks for Internal Medicine, pp. 558-562
- Bradley and Daroff's Neurology in Clinical Practice, pp. 38, 510-512
- Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 637-649
- Rosen's Emergency Medicine, pp. 1985-1992, 169
- Textbook of Family Medicine, 9e, pp. 1228-1232
- Adams and Victor's Principles of Neurology, 12th Edition, p. 333
This is a shared conversation. Sign in to Orris to start your own chat.