I need answers for... What are the causes of acute, subacute, and chronic fevers? What are the examples for continuous, remittent, intermittent, and relapsing type of fevers? In India, if you suspect... if there is fever, you have to suspect what and all diseases which are more common? If a patient presents with fever with ar- arthralgia, what are the differential diagnosis? If they're present with fever with rash, then what and all are the diagnosis? What is Jenvey's lesion? Fever with hepatosplenomegaly seen in which and all conditions? Uh, then I want about life cycle of malaria, abdominal TB. Where in all do we see fever with altered sensorium? What is leukoencephalopathy?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is your comprehensive clinical reference covering all the topics you asked about:
Fever - Complete Clinical Overview
1. Causes of Acute, Subacute, and Chronic Fever
Acute Fever (< 2 weeks)
- Infections: Most bacterial infections (pneumonia, UTI, cellulitis, meningitis), viral illnesses (influenza, dengue, COVID-19), malaria, typhoid (early phase), leptospirosis
- Non-infectious: Drug fever, transfusion reactions, pulmonary embolism, deep vein thrombosis, acute myocardial infarction, hematoma, post-operative fever
Subacute Fever (2-6 weeks)
- Infections: Infective endocarditis, brucellosis, tuberculosis (early), typhoid (prolonged), enteric fever, fungal infections, viral hepatitis
- Non-infectious: Malignancy (lymphoma), connective tissue diseases (SLE, vasculitis), drug fever
- Common in ICU: ~80% of febrile episodes are infectious - pneumonia, catheter-related infections
Chronic Fever (> 6 weeks / Fever of Unknown Origin)
- Infections: Tuberculosis, brucellosis, deep-seated abscesses, infective endocarditis, HIV, fungal infections (histoplasmosis - classified by duration into acute/subacute/chronic)
- Non-infectious: Malignancies (lymphoma, renal cell carcinoma, hepatocellular carcinoma), connective tissue diseases (SLE, Adult Still disease, vasculitis), granulomatous diseases (sarcoidosis, Crohn's)
- Drug fever can occur at any duration
Sources: Goldman-Cecil Medicine; Histoplasmosis chapter, Red Book 2021
2. Types of Fever - Patterns with Examples
| Type | Definition | Classic Examples |
|---|---|---|
| Continuous | Temperature stays elevated throughout 24 hours, does not touch normal; variation < 1°C | Typhoid fever (Salmonella typhi), lobar pneumonia, urinary tract infection |
| Remittent | Temperature remains elevated but touches near-normal values; variation > 1°C but does NOT reach normal | Infective endocarditis, many viral infections, brucellosis |
| Intermittent | Temperature spikes to fever then returns to NORMAL (afebrile) during the same day | Malaria (tertian = P. vivax/ovale every 48h; quartan = P. malariae every 72h), pyogenic abscess, septicemia, kala-azar (double daily spike = Pel-Ebstein not applicable here) |
| Relapsing / Periodic | Days of fever alternating with days of completely normal temperature | Borrelia relapsing fever, malaria (relapses from P. vivax/ovale hypnozoites), Pel-Ebstein fever in Hodgkin's lymphoma, brucellosis (undulant fever) |
3. Fevers Common in India - What to Suspect
In the Indian subcontinent, the following should be strongly suspected in a febrile patient:
Infectious (most common):
- Malaria (P. vivax most common; P. falciparum - severe/cerebral)
- Typhoid / Enteric fever (Salmonella typhi/paratyphi)
- Dengue fever (Aedes mosquito-borne)
- Chikungunya (fever + severe arthralgia)
- Leptospirosis (post-flood, occupational exposure)
- Scrub typhus (Orientia tsutsugamushi; eschar is pathognomonic)
- Rickettsial fever (spotted fevers, tick-borne)
- Tuberculosis (pulmonary and extrapulmonary; chronic low-grade fever)
- Kala-azar / Visceral leishmaniasis (Bihar, Jharkhand, Bengal, Assam endemic belt)
- Brucellosis (cattle farming areas, dairy workers)
- Viral hepatitis A/E (hepatitis with fever in endemic areas)
- Japanese encephalitis (Culex mosquito; Bihar, UP, Assam)
- Melioidosis (Northeast India, coastal areas)
- Enteric fever-related complications
Non-infectious to consider:
- Connective tissue diseases (SLE, adult Still's disease)
- Lymphomas
- Drug fever
4. Fever with Arthralgia - Differential Diagnosis
| Diagnosis | Key Features |
|---|---|
| Chikungunya | Bilateral symmetrical, very severe joint pain (incapacitating); maculopapular rash; Aedes aegypti |
| Dengue | Bone-crushing myalgia + arthralgia; retro-orbital pain; thrombocytopenia |
| Acute Rheumatic Fever | Migratory polyarthritis; Jones criteria (major: carditis, chorea, erythema marginatum, subcutaneous nodules, arthritis) |
| Rheumatoid Arthritis (reactive/early) | Symmetrical small joint involvement; morning stiffness |
| Serum sickness / Drug reaction | Fever + arthralgia + rash + urticaria |
| Infective Endocarditis | Fever + arthralgia + cardiac murmur |
| Primary HIV seroconversion (ARS) | Fever, pharyngitis, lymphadenopathy, rash, arthralgia; resembles glandular fever |
| Viral hepatitis (HBV) | Serum sickness-like prodrome: fever + arthralgia + rash before jaundice |
| SLE | Non-erosive arthralgia, malar rash, multi-system involvement |
| Adult Still's disease | Daily spiking fever, evanescent salmon-colored rash, arthralgia |
| Lyme disease | Tick exposure; erythema migrans rash; migratory arthralgia, carditis, neuroborreliosis |
| Brucellosis | Undulant fever; occupational/dietary exposure; sacroiliitis |
Sources: Fuster & Hurst's The Heart; Fitzpatrick's Dermatology; Goldman-Cecil Medicine
5. Fever with Rash - Differential Diagnosis
By Rash Type:
Maculopapular rash + fever:
- Measles (cephalocaudal spread, Koplik spots)
- Rubella (milder, lymphadenopathy)
- Dengue
- Chikungunya
- Infectious mononucleosis (EBV)
- Roseola infantum (HHV-6; rash appears as fever breaks)
- Primary HIV (ARS)
- West Nile virus
- Zika virus
- Parvovirus B19 (slapped cheek + lacy reticular rash)
- Scarlet fever (sandpaper rash, strawberry tongue, desquamation of palms/soles)
- Rocky Mountain spotted fever (centripetal spread, palms/soles involvement)
- Ehrlichiosis
- Drug reactions (exanthematous)
- Kawasaki disease
Petechiae/Purpura + fever (EMERGENCIES):
- Meningococcemia (Neisseria meningitidis) - non-blanching purpura, rapidly progressive; EMERGENCY
- Rocky Mountain spotted fever (may progress to purpura)
- Disseminated gonococcal infection
- Infective endocarditis (petechiae + Osler nodes + Janeway lesions)
- Dengue hemorrhagic fever
- Thrombotic thrombocytopenic purpura (TTP)
- Vasculitis (HSP/IgA vasculopathy)
Vesicular/Pustular rash + fever:
- Varicella (chickenpox)
- Herpes zoster (dermatomal)
- Smallpox (all lesions in same stage - historical)
- Herpes simplex
- Enteroviral hand-foot-mouth disease
Other specific rashes:
- Erythema migrans - Lyme disease
- Erythema marginatum - Acute rheumatic fever
- Butterfly (malar) rash - SLE
- Erythema nodosum - TB, sarcoidosis, streptococcal infection, Crohn's
- Eschar - Scrub typhus, rickettsial infections
- Rose spots - Typhoid fever (abdomen/chest; faint salmon-colored)
Source: Goldman-Cecil Medicine, Textbook of Family Medicine, Harrison's Principles of Internal Medicine 22E
6. Janeway Lesions
Definition: Janeway lesions are non-tender, erythematous or hemorrhagic macular/papular lesions on the palms and soles, caused by septic emboli in infective endocarditis.
Key features:
- Location: palms and soles (plantar aspect, thenar/hypothenar eminence)
- Non-tender (unlike Osler nodes which are PAINFUL)
- Caused by infected microemboli with microabscess formation
- Associated with acute infective endocarditis (especially Staphylococcus aureus)
Comparison with Osler Nodes:
| Feature | Janeway Lesions | Osler Nodes |
|---|---|---|
| Tenderness | Non-tender | Painful/tender |
| Location | Palms, soles | Fingertips, pulp of digits |
| Mechanism | Septic emboli (microabscesses) | Immune complex deposition |
| Association | Acute IE (Staph aureus) | Subacute IE (Strep viridans) |
Other signs of infective endocarditis: Fever (80-90%), heart murmur (75-85%), splinter hemorrhages (subungual), Roth spots (retinal), conjunctival hemorrhages, petechiae.
Sources: Textbook of Family Medicine; Dermatology 2-Volume Set 5e; Braunwald's Heart Disease
7. Fever with Hepatosplenomegaly - Conditions
Infectious:
- Malaria (P. vivax/falciparum - massive splenomegaly in chronic/hyperreactive malaria)
- Kala-azar / Visceral Leishmaniasis (massive progressive splenomegaly; the largest spleens seen in clinical practice)
- Typhoid fever (Salmonella; splenomegaly in 2nd-3rd week)
- Infectious mononucleosis (EBV; teenager with sore throat + lymphadenopathy + hepatosplenomegaly)
- Viral hepatitis (A, B, E)
- Infective endocarditis (bacterial emboli)
- Brucellosis
- Leptospirosis (Weil's disease)
- Schistosomiasis (portal hypertension, massive splenomegaly)
- Miliary tuberculosis
- Typhus/rickettsial disease
- Cytomegalovirus (CMV)
- HIV/AIDS
Non-infectious:
- Lymphomas (Hodgkin's and Non-Hodgkin's)
- Leukemias (CML - massive splenomegaly)
- Hemolytic anemias (thalassemia, sickle cell)
- Storage diseases (Gaucher's, Niemann-Pick)
- Autoimmune diseases (SLE, Still's disease)
- Sarcoidosis
- Portal hypertension (cirrhosis - enlargement of both; liver may actually shrink in cirrhosis)
8. Life Cycle of Malaria
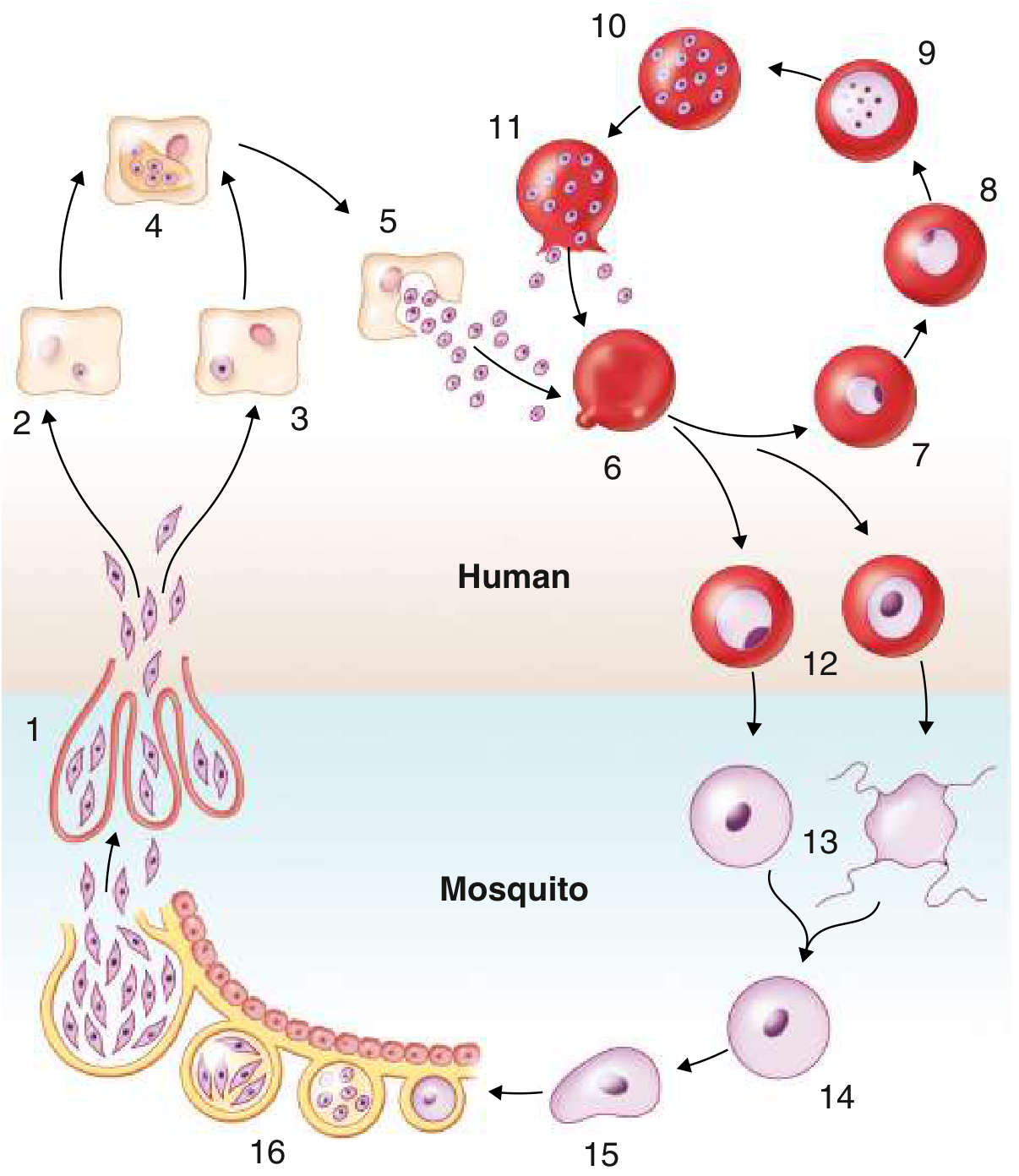
IN THE HUMAN HOST:
1. Exoerythrocytic (Liver) Phase:
- Female Anopheles mosquito bites → injects sporozoites into bloodstream (Step 1)
- Sporozoites travel to liver within 1 hour → enter hepatocytes
- Develop into tissue schizonts (Step 4) → each releases up to 30,000 merozoites (Step 5)
- Hypnozoites (Step 3): In P. vivax and P. ovale only - some sporozoites remain dormant in liver → can reactivate months/years later causing relapse
2. Erythrocytic Phase (symptomatic):
- Merozoites invade RBCs (Step 6) → ring form → trophozoite (Step 9) → schizont (Step 10) → rupture releases new merozoites (Step 11)
- Cycle duration: 48 hrs (P. falciparum, P. vivax, P. ovale) → tertian fever; 72 hrs (P. malariae) → quartan fever
- Schizont rupture causes fever spikes (pyrogens released)
3. Gametocyte Phase:
- Some merozoites develop into male and female gametocytes (Step 12) - taken up by mosquito
IN THE MOSQUITO HOST:
- Gametocytes → gametes → fertilization → zygote (Step 14) → ookinete (Step 15) → oocyst on gut wall (Step 16) → rupture → sporozoites migrate to salivary gland (Step 1) → ready to infect next human
Clinically important species differences:
| Feature | P. vivax | P. falciparum | P. malariae | P. ovale |
|---|---|---|---|---|
| Fever cycle | 48h (tertian) | 48h (malignant tertian) | 72h (quartan) | 48h |
| Hypnozoites (relapse) | YES | No | No | YES |
| Severe disease | Less common | Most dangerous | Rare | Rare |
| RBC preference | Reticulocytes | All RBCs | Old RBCs | Reticulocytes |
Source: Goldman-Cecil Medicine 22E; Medical Microbiology 9e
9. Abdominal Tuberculosis
Definition: TB involving any abdominal organ, accounting for ~15% of extrapulmonary TB cases.
Forms:
- Tuberculous lymphadenopathy - MOST COMMON form; mesenteric lymph nodes most frequently involved; can develop central caseation and calcification
- Peritoneal TB - Three subtypes:
- Wet ascitic type (most common): large free or loculated ascites; exudative; high SAAG
- Fixed fibrotic type: omental/mesenteric involvement, matted bowel loops on imaging
- Dry plastic type: fibrous peritoneal reaction, nodules, adhesions
- GI TB - Most commonly involves the ileocecal region (MC site), followed by the jejunum
- Morphological types: ulcerative, hypertrophic, stricturing
- Difficult to distinguish from Crohn's disease
- Visceral TB - Solid organs; genitourinary most frequent
Clinical Features:
- Abdominal pain (most common), fever, weight loss (present for months)
- Right lower quadrant mass in ~25%
- Ascites on cross-sectional imaging strongly suggests abdominal TB over Crohn's
Key distinguishing features from Crohn's:
- TB: transverse ulcers, patulous ileocecal valve, ascites, granulomas with caseation (>400 µm, large giant cells)
- Crohn's: left colonic involvement, longitudinal ulcers, cobblestoning, skip lesions, rectal involvement
Histology: Caseating granulomas (coalescent, >400 µm, large giant cells); AFB staining, PCR, or culture confirms
Diagnosis: High suspicion in risk groups (immigrants from endemic areas, HIV, malnourished). Anti-TNF therapy for Crohn's can worsen unrecognized TB - must rule out TB before starting biologics.
Source: Yamada's Textbook of Gastroenterology 7e; Grainger & Allison's Diagnostic Radiology
10. Fever with Altered Sensorium - Where We See It
This is a serious clinical presentation. Key conditions:
Infections of CNS:
- Bacterial meningitis (N. meningitidis, S. pneumoniae, L. monocytogenes) - fever + neck stiffness + altered sensorium (triad)
- Viral encephalitis (Herpes simplex - most common treatable cause; Japanese encephalitis in India; West Nile)
- Cerebral malaria (P. falciparum - parasitized RBCs occlude cerebral vessels; severe manifestation)
- Tubercular meningitis (subacute onset, cranial nerve palsies)
- Bacterial brain abscess (focal signs + fever)
- Cerebral toxoplasmosis (HIV patients)
- Rickettsial encephalitis (Scrub typhus with meningoencephalitis)
Systemic infections with CNS involvement:
- Leptospirosis (Weil's disease) - encephalitis, altered sensorium, psychosis, seizures, hemiplegia - quoted directly from Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Typhoid encephalopathy ("muttering delirium" - 2nd-3rd week)
- Septic encephalopathy (any severe sepsis - multiorgan dysfunction)
- Dengue encephalitis (rare manifestation of dengue)
- Rabies (hydrophobia, aerophobia, agitation)
- Neuro-syphilis (chronic, VDRL positive)
- Plasmodium falciparum - cerebral malaria (specific to P. falciparum)
- Polyarteritis Nodosa (PAN) - catastrophic intracranial hemorrhage with altered sensorium has been described (especially pediatric PAN)
Non-infectious:
- Liver failure (hepatic encephalopathy - asterixis, elevated ammonia)
- Uremic encephalopathy
- Anti-NMDA receptor encephalitis (autoimmune; fever + psychiatric + movement disorder)
- Heat stroke (exertional or classic)
- Drug/toxin ingestion
- Metabolic derangements (hyponatremia, hypoglycemia, DKA)
Sources: Bradley and Daroff's Neurology; Kaplan & Sadock's Comprehensive Textbook; Goldman-Cecil Medicine
11. Leukoencephalopathy
Progressive Multifocal Leukoencephalopathy (PML)
Definition: PML is a demyelinating brain disease caused by lytic replication of JC polyomavirus in oligodendrocytes (the cells that produce myelin) in subcortical white matter and, rarely, gray matter neurons.
Pathogen: JC polyomavirus (human polyomavirus 2)
Pathobiology:
- JC virus replicates in oligodendrocytes → cell lysis → loss of myelin sheaths
- Affected oligodendrocytes: enlarged nuclei with eosinophilic intranuclear inclusions
- Lesions start in subcortical white matter, less commonly cerebellum or basal ganglia
- As demyelination expands: lesions range from <1 mm to several cm; multiple zones coalesce
Epidemiology:
- General population: ~0.3 per 100,000 person-years (North America/Europe)
- HIV/AIDS (pre-ART era): ~2.4 per 1,000 patient-years; prevalence 1-7%
- Natalizumab (for MS): ~2.13 per 1,000 patient-years; rises to 11.1 per 1,000 in JC-seropositive patients treated >24 months
- Also seen with: lymphoproliferative malignancies, other immunosuppressive biologics, idiopathic CD4 lymphocytopenia
Predisposing conditions (any state of impaired T- and B-cell immunity):
- HIV/AIDS (most common historically)
- Hematologic malignancies (lymphoma, CLL, multiple myeloma)
- Organ transplant recipients (on immunosuppressants)
- Natalizumab therapy (multiple sclerosis)
- Other monoclonal antibodies (rituximab, efalizumab)
- Sarcoidosis
Clinical Manifestations:
- Progressive motor weakness (most common)
- Speech abnormalities, cognitive deficits
- Headache, ataxia, aphasia, cranial nerve deficits
- Visual disturbances (optic agnosia, cortical blindness, oculomotor abnormalities)
- Seizures (more common with gadolinium-enhancing cortical lesions)
- Sensory deficits of hands (parietal involvement)
Diagnosis: MRI (T2/FLAIR hyperintense non-enhancing white matter lesions), JC virus PCR in CSF
Treatment:
- No specific anti-JC viral therapy proven effective
- For HIV patients: start/optimize antiretroviral therapy → immune reconstitution
- Withdraw offending immunosuppressive agent (e.g., stop natalizumab, plasmapheresis to accelerate removal)
- Risk of IRIS (immune reconstitution inflammatory syndrome) when immunity is restored
Prevention: In HIV/AIDS, ART reducing HIV to undetectable levels has dramatically reduced PML incidence.
Source: Goldman-Cecil Medicine International Edition; Firestein & Kelley's Textbook of Rheumatology; Bradley and Daroff's Neurology in Clinical Practice
Quick Summary Mnemonics
Fever patterns - "CRIR":
- Continuous = Typhoid, lobar pneumonia
- Remittent = Infective endocarditis, viral fevers
- Intermittent = Malaria, pyogenic abscess
- Relapsing = Borrelia, Hodgkin's (Pel-Ebstein), brucellosis
Fever + Rash EMERGENCIES to rule out first:
- Meningococcemia (non-blanching petechiae/purpura → septic shock)
- Rocky Mountain Spotted Fever (petechiae on palms/soles spreading centrally)
- Toxic Shock Syndrome (Staph/Strep)
- Staphylococcal Scalded Skin Syndrome
Janeway vs Osler:
- Janeway = No pain, on palms/soles = Acute IE (Staph aureus)
- Osler = Ouchy/painful, on digits = Subacute IE (Strep viridans)
This is a shared conversation. Sign in to Orris to start your own chat.