
20260516_224421.jpg
Kya problem hai isme btao
Reading File
Is ECG ko main carefully dekh chuka hoon. ECG report mein machine ke conclusions bhi likhe hain. Seedha analysis karta hoon:
🫀 ECG Analysis — Kya Problem Hai?
Machine ke Conclusions (ECG ke neeche likha hua):
ECG machine ne khud ye findings report ki hain:
- Severity: Left Axis Deviation — Dil ki electrical axis left side shift ho gayi hai
- 1° AV Block — SA node se AV node tak signal thoda slow ja raha hai (PR interval badha hua)
- ST Depression — Heart ke muscles ko poora oxygen nahi mil raha (ischemia ka sign)
- Possible Anterolateral Myocardial Ischemia — Dil ke aage aur side wale hisse mein blood supply kam ho sakti hai
- High Lateral ST Depression — aVL aur high lateral leads mein ST neecha gira hua
- I, aVL, V6 — Abnormal T Wave — In leads mein T wave ulti ya flat hai
Kya Matlab Hai Saral Bhasha Mein?
| Finding | Matlab |
|---|---|
| ST Depression | Dil ko uss waqt ya pehle se blood kam mil raha tha |
| Anterolateral Ischemia | Dil ke aage wale hisse ki nali (LAD artery) mein block ya tangi ho sakti hai |
| Abnormal T waves | Dil ke cells stress mein hain |
| Left Axis Deviation | Dil ki wiring mein koi badlaav — kabhi kabhi akela bhi milta hai |
| 1° AV Block | Signal thoda slow hai, abhi critical nahi |
⚠️ Ye ECG Serious Hai!
ST depression + anterolateral ischemia — ye NSTEMI (Non-ST Elevation Myocardial Infarction) ya Unstable Angina ka sign ho sakta hai.
Machine ne khud likha hai: "Report need physician confirm"
✅ Turant Kya Karna Chahiye:
- Abhi doctor/cardiologist ko dikhao — ye ECG urgent attention maangta hai
- Troponin blood test karwao — confirm karta hai dil ka damage hua hai ya nahi
- Echocardiogram bhi recommend kiya ja sakta hai
- Agar seene mein dard, saans phoolna, paseena, ghabhrahat ho — emergency hospital jao
⚕️ Disclaimer: Ye AI analysis hai. Ye ECG ki machine interpretation + mere observations pe based hai. Kisi qualified cardiologist se zaroor milwao — final diagnosis wahi karenge.
Find latest guidelines on NSTEMI diagnosis and management
Reading File
Searching PubMed
"NSTEMI" AND "guidelines" AND "management"
Searching the Web
NSTEMI ACS guidelines 2024 2025 ESC ACC AHA diagnosis management
Finding Sources
Reading Web Page
https://www.hendrickhealth.org/documents/content/2025-ACS-Gu…
Reading Article
PMID: 41749019
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive, guideline-based summary of NSTEMI diagnosis and management — drawn from Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine, Rosen's Emergency Medicine, and the landmark 2025 ACC/AHA/ACEP/NAEMSP/SCAI ACS Guideline (the most current US guideline, replacing all prior ACS guidelines).
NSTEMI: Latest Guidelines (2025)
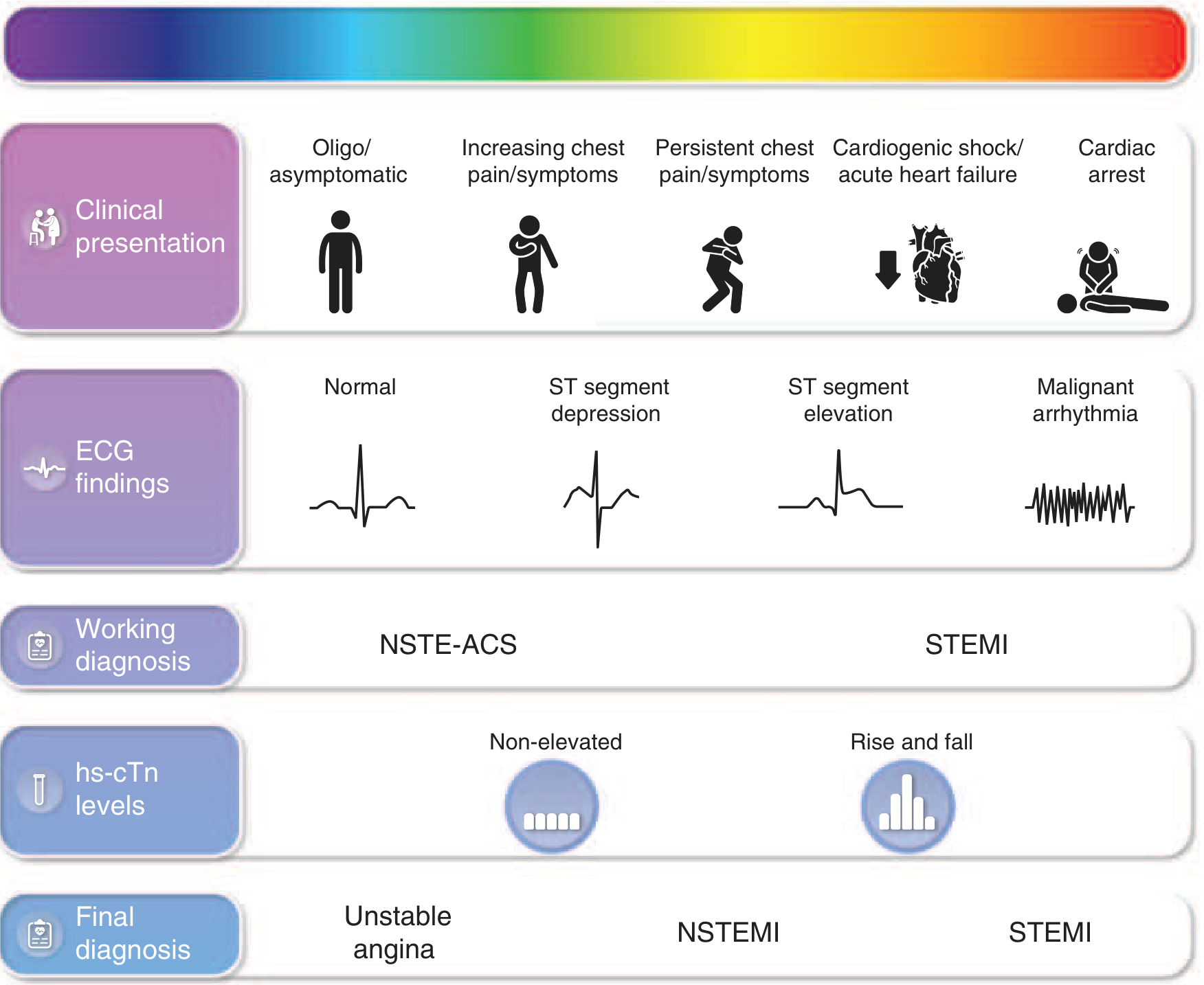
ACS Spectrum — Where NSTEMI Fits
1. DIAGNOSIS
Clinical Presentation
Chest discomfort at rest or minimal exertion, lasting >10 min, with at least one of:
- New onset within prior 2 weeks
- Crescendo pattern (more severe/frequent than before)
- Occurring at rest
Anginal equivalents (more common in women, elderly, diabetics): dyspnea, nausea, epigastric pain, diaphoresis, weakness.
ECG Findings
- ST depression ≥0.5 mm in ≥2 contiguous leads → most specific for NSTEMI ischemia (seen in ~1/3 of patients)
- New T-wave inversions ≥0.3 mV → significant
- No ST elevation required — ECG changes are NOT required to confirm NSTE-ACS diagnosis
- Serial ECGs are mandatory when initial ECG is nondiagnostic
Biomarkers (Cornerstone of Diagnosis)
- High-sensitivity cardiac Troponin (hs-cTn) is the recommended biomarker (Class I)
- NSTEMI = troponin rise/fall above 99th percentile + ischemic symptoms/ECG changes
- 0/1h or 0/2h rapid rule-out/rule-in pathways using hs-cTn are now standard (2025 ESC/ACC)
- CK-MB is no longer recommended for initial diagnosis
Risk Stratification (Mandatory)
Use validated scores to guide timing of invasive strategy:
| Score | Components |
|---|---|
| TIMI score | Age ≥65, ≥3 CAD risk factors, known CAD, ST deviation >0.5mm, ≥2 angina episodes in 24h, elevated troponin, aspirin use |
| GRACE score (preferred) | Age, HR, BP, creatinine, Killip class, arrest at admission, ST deviation, troponin — GRACE 3.0 (2025) has improved calibration across sexes/age groups |
| HEART score | History, ECG, Age, Risk factors, Troponin |
2. MANAGEMENT
A. Anti-Ischemic Therapy (Immediate)
| Drug | Details |
|---|---|
| Nitrates | IV/sublingual; for symptom relief, BP control |
| Beta-blockers | Oral, target HR 50–60 bpm (avoid if hypotension, AV block, bronchospasm) |
| Calcium channel blockers | Verapamil/diltiazem if nitrates + beta-blockers fail or contraindicated |
| Oxygen | Only if SpO₂ <90%; routine O₂ in normoxic patients not recommended (2025 ACC/AHA Class III: Harm) |
| Morphine | Only for refractory severe pain (caution — may mask symptoms) |
B. Antithrombotic Therapy (Two Pillars)
Antiplatelet:
- Aspirin 150–325 mg loading → 75–100 mg/day maintenance (Class I)
- DAPT (Dual Antiplatelet Therapy): Add P2Y₁₂ inhibitor (Class I)
- Ticagrelor 180 mg load → 90 mg BD (preferred; superior to clopidogrel — reduces CV death + MI)
- Prasugrel 60 mg load → 10 mg/day (only post-angiography when PCI planned; avoid if prior stroke/TIA)
- Clopidogrel 300–600 mg load → 75 mg/day (acceptable alternative, less potent)
- DAPT duration: Default 12 months post-ACS (Class I); if high bleeding risk → Ticagrelor monotherapy after 1 month post-PCI (Class I) — NEW 2025 recommendation
Anticoagulation (during hospitalization):
- UFH (unfractionated heparin) or Enoxaparin (LMWH) — Class I
- Fondaparinux — preferred in conservative strategy (lower bleeding)
- Bivalirudin — option during PCI
C. Statins (Early and Intensive)
- High-intensity statin: Atorvastatin 80 mg/day or Rosuvastatin 40 mg/day — initiated immediately (in-hospital)
- Target LDL-C: <55 mg/dL (1.4 mmol/L) with ≥50% reduction from baseline
- If target not achieved: add Ezetimibe 10 mg/day
- If still not at target: add PCSK9 inhibitor (Alirocumab/Evolocumab) — 2025 ESC/EAS update: combination therapy immediately at hospitalization, not stepwise after discharge
D. Invasive Strategy — When and How Soon?
| Category | Timing |
|---|---|
| Very high risk (refractory ischemia, hemodynamic instability, life-threatening arrhythmia, cardiogenic shock) | Immediate angiography (<2h) |
| High risk (dynamic ST/T changes, GRACE score >140, elevated troponin, TIMI ≥3) | Early invasive (<24h) |
| Intermediate risk | Invasive within 72h |
| Low risk (TIMI 0–1, normal ECG, normal troponin) | Conservative/non-invasive evaluation |
PCI Approach (2025 update):
- In NSTE-ACS with multivessel disease (MVD): PCI of non-culprit lesions (at index or staged) is now Class I recommendation to reduce MACE — upgraded from 2b in prior guidelines
- Elderly patients (≥80 years): Early invasive approach superior to conservative in stable octogenarians (SENIOR-NSTEMI data)
E. Secondary Prevention (Post-Discharge)
| Drug | Target |
|---|---|
| Aspirin | Indefinite |
| P2Y₁₂ inhibitor | 12 months (shorter if high bleeding risk) |
| High-intensity statin + Ezetimibe | LDL <55 mg/dL |
| PCSK9 inhibitor | If LDL not at target |
| ACE inhibitor / ARB | Especially if EF <40%, HTN, diabetes |
| Beta-blocker | Especially if EF <40% |
| SGLT2 inhibitor | If HFrEF or diabetes (emerging role, 2025) |
| Colchicine | Anti-inflammatory benefit in selected patients |
3. Key 2025 Updates vs Prior Guidelines
| Change | Old | 2025 ACC/AHA |
|---|---|---|
| Routine O₂ in normoxic patients | Sometimes given | Class III: Harm |
| Non-culprit PCI in NSTE-ACS MVD | Class 2b (maybe reasonable) | Class I (recommended) |
| DAPT → monotherapy after 1 month PCI | Not standard | Class I (Ticagrelor monotherapy) |
| LDL management | Stepwise escalation | Immediate combination therapy at hospitalization |
| Risk scoring | GRACE 2.0 | GRACE 3.0 (better calibration) |
Sources
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 285
- Goldman-Cecil Medicine, Chapter 57 — NSTE-ACS
- Rosen's Emergency Medicine — ACS section
- 2025 ACC/AHA/ACEP/NAEMSP/SCAI ACS Guideline — replaces all prior US ACS guidelines
- 2025 ESC/EAS Focused Lipid Update — aggressive in-hospital LDL lowering
- CVIT 2026 PCI Consensus [PMID: 41749019]
⚕️ These guidelines are for clinical professionals. Individual patient management should be tailored by a treating cardiologist based on full clinical assessment.
This is a shared conversation. Sign in to Orris to start your own chat.