Mechanism of ovulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
ovulation mechanism LH surge follicle rupture
Loading Image
Loading Image
Reading File
Here is a comprehensive account of the mechanism of ovulation, synthesized from Guyton & Hall Physiology and Boron & Boulpaep Medical Physiology.
Mechanism of Ovulation
1. Overview
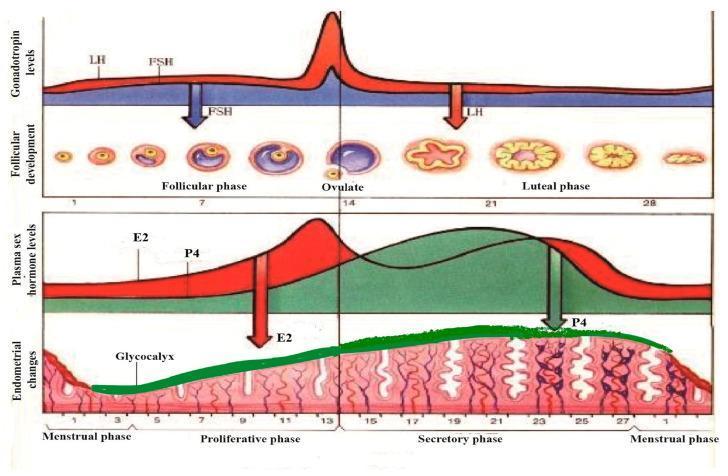
Ovulation occurs on day 14 of a 28-day cycle — the release of a mature secondary oocyte from the dominant Graafian follicle, triggered by a preovulatory LH surge.
2. Prerequisites: Follicular Maturation (Follicular Phase, Days 1–13)
- Rising FSH at the start of the cycle recruits a cohort of primordial follicles into development.
- One follicle becomes dominant due to a higher number of FSH receptors and greater aromatase activity (converting androstenedione → estradiol).
- Less dominant follicles undergo atresia due to a relatively high androgen/estrogen ratio in their local environment.
- The dominant follicle progressively secretes increasing amounts of estradiol (E2).
3. The LH Surge — The Trigger
The dominant follicle's rising estradiol initially exerts negative feedback on the hypothalamus and anterior pituitary, suppressing LH and FSH. However, when estradiol rises sharply and is sustained above a threshold (~200 pg/mL for ≥50 hours), the feedback switches from negative to positive:
- Estradiol sensitizes the anterior pituitary to GnRH
- The hypothalamus increases GnRH pulse frequency
- Result: a massive LH surge (~6–10 fold increase), peaking ~16 hours before ovulation, along with a smaller 2–3 fold FSH rise
Ovulation follows ~36 hours after surge onset, or ~12 hours after the LH peak.
The LH surge terminates partly due to rising progesterone (negative feedback) and partly from depletion of pituitary gonadotropin stores.
4. LH-Induced Events at the Follicle
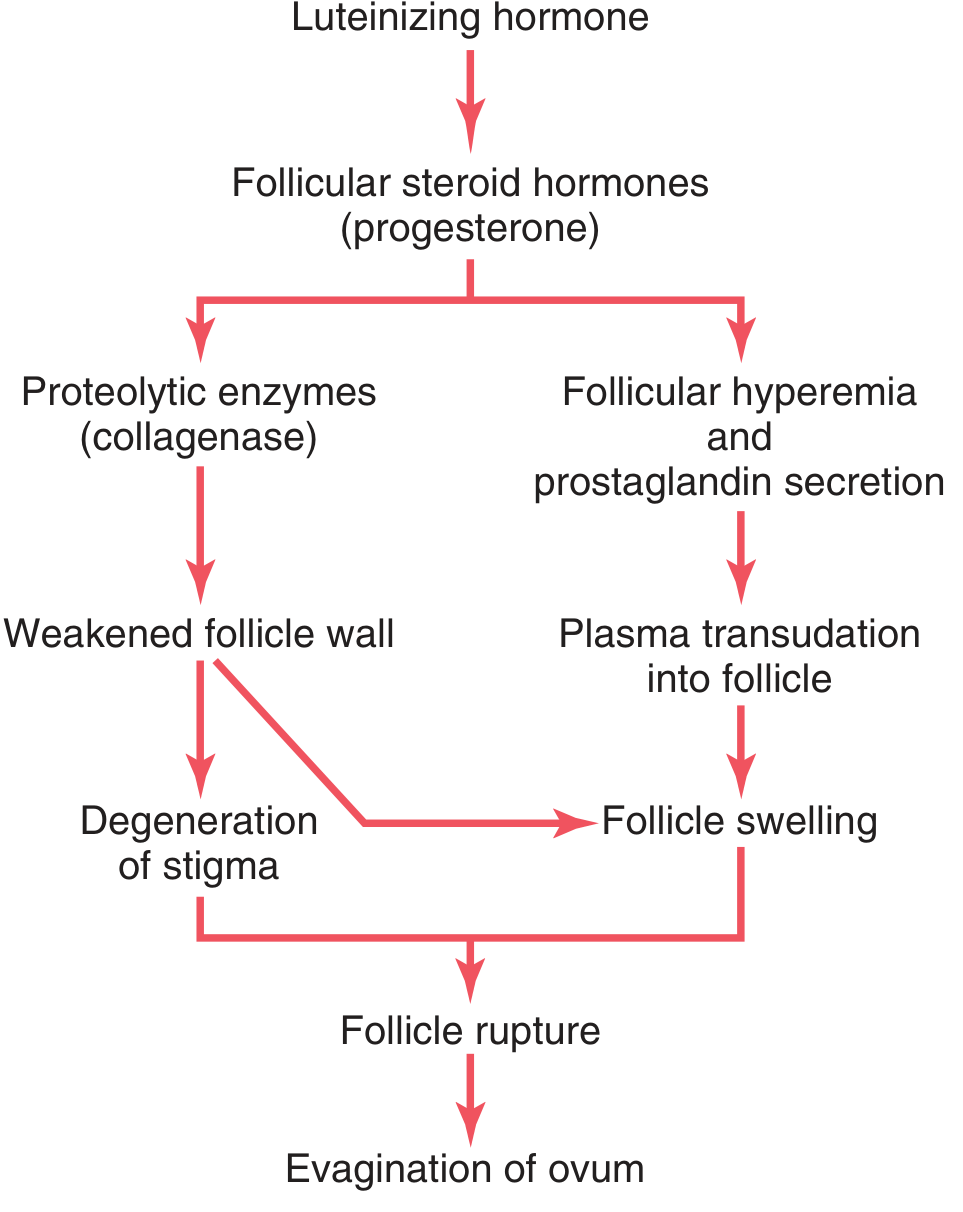
The LH surge triggers the granulosa and theca cells to secrete follicular steroid hormones (principally progesterone), which then set off two parallel mechanisms:
Pathway A — Proteolytic Wall Degradation
- LH → progesterone → release of proteolytic enzymes (collagenase) from lysosomes in the theca externa
- Enzymes dissolve the follicular capsule wall → weakening of the wall → degeneration of the stigma (a small nipple-like protrusion at the follicle apex)
Pathway B — Hyperemia and Pressure Buildup
- LH → progesterone → neovascularization of the follicle wall + secretion of prostaglandins (vasodilators) into follicular tissue
- → plasma transudation into the follicle → follicle swelling
Both pathways converge:
Follicle swelling + stigma degeneration → follicle rupture → evagination of the ovum
5. Oocyte Maturation
At the time of the LH surge, the primary oocyte (which had been arrested in prophase I of meiosis since fetal life) resumes meiosis:
- Completes meiosis I → produces a secondary oocyte (haploid, 2N DNA) + first polar body
- Secondary oocyte arrests in metaphase II until fertilization
- The oocyte is surrounded by the zona pellucida and corona radiata (granulosa cells)
The cumulus oophorus expands under LH influence, facilitated by FSH-stimulated hyaluronidase synthesis — the oocyte-cumulus complex floats free within the antrum before expulsion.
6. The Act of Ovulation
- The stigma protrudes from the surface of the ovary
- Fluid begins to ooze through the stigma, then the stigma ruptures widely
- Viscous follicular fluid carrying the oocyte surrounded by the corona radiata is expelled
- The fimbriae of the fallopian tube sweep the oocyte into the tube
7. Post-Ovulatory: Corpus Luteum Formation
Immediately after ovulation, residual granulosa and theca interna cells undergo luteinization:
- Cells enlarge, fill with lipid inclusions (yellowish appearance)
- Form the corpus luteum, which secretes progesterone + estrogen + inhibin
- These exert negative feedback on the pituitary → suppress FSH/LH
- If no fertilization: corpus luteum regresses (~day 24–26), hormone levels fall → menstruation begins and the cycle restarts
Summary Table
| Step | Event | Key Mediator |
|---|---|---|
| 1 | Follicular recruitment & dominance | FSH, estradiol |
| 2 | Positive feedback switch | High sustained E2 |
| 3 | LH surge | GnRH → LH (6–10×) |
| 4 | Proteolytic wall dissolution | Progesterone → collagenase |
| 5 | Follicle hyperemia & swelling | Prostaglandins, neovascularization |
| 6 | Stigma rupture, oocyte expulsion | Combined wall weakening + pressure |
| 7 | Oocyte completes meiosis I → arrests in metaphase II | LH |
| 8 | Corpus luteum formation | LH (luteinization) |
Without the preovulatory LH surge, ovulation cannot occur. Anovulatory cycles (seen at puberty and perimenopause) result from an insufficient LH surge.
Sources: Guyton and Hall Textbook of Medical Physiology; Boron & Boulpaep Medical Physiology
I need an easier explanation of the given flowchart
Here's a simple, plain-English walkthrough of the flowchart:
The Flowchart, Step by Step
Luteinizing Hormone (LH)
↓
Follicular steroid hormones (progesterone)
↙ ↘
Proteolytic Follicular hyperemia
enzymes + prostaglandin secretion
(collagenase) ↓
↓ Plasma transudation
Weakened into follicle
follicle wall ↓
↓ ————————→ Follicle swelling
Degeneration ↓
of stigma ————→ Follicle swelling
↘ ↙
Follicle rupture
↓
Evagination of ovum
Step 1 — LH arrives
LH (Luteinizing Hormone) is released in a big surge from the pituitary gland. Think of it as the "go signal" for ovulation.
Step 2 — LH tells the follicle to make progesterone
LH stimulates the follicle (the fluid-filled sac holding the egg) to produce progesterone and other steroid hormones. These hormones then kick off two separate processes simultaneously.
Left branch — Breaking down the wall
Step 3L: Progesterone triggers the release of proteolytic enzymes (specifically collagenase — a protein-digesting enzyme).
Step 4L: These enzymes literally digest and weaken the follicle wall, like acid dissolving a bag.
Step 5L: The weakest point of the wall — a small spot called the stigma (like a blister on top of the follicle) — starts to break down and degenerate.
Right branch — Filling the follicle with fluid
Step 3R: Progesterone also causes hyperemia (increased blood flow to the follicle) and the release of prostaglandins (local chemicals that dilate blood vessels).
Step 4R: Because of the extra blood flow and vasodilation, fluid from blood plasma leaks into the follicle — this is called plasma transudation.
Step 5R: The extra fluid causes the follicle to swell up, like a balloon being inflated.
Step 6 — Everything converges: Rupture
Now both branches come together:
- The wall is weakened (left branch)
- The follicle is swollen with pressure (right branch)
The combination of a weakened wall + high internal pressure causes the follicle to rupture — it bursts open.
Step 7 — The egg is released
The egg (ovum), surrounded by a cloud of cells (corona radiata), is pushed out (evaginated) through the rupture site and swept into the fallopian tube.
One-Line Summary
LH → progesterone → (1) enzymes dissolve the wall + (2) fluid inflates the follicle → follicle bursts → egg is released.
This is a shared conversation. Sign in to Orris to start your own chat.