Explain me ANATOMY OF AXILLA in a story and give me notes of axillary after story
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have everything I need. Now let me write the full story + structured notes.
🏠 The Story of the Axilla: "The Gateway Palace"
A story to remember the anatomy of the axilla - based on Gray's Anatomy for Students
Imagine the human body as a great kingdom. The neck is the royal capital, and the upper limb is a distant province that needs supplies, roads, and messengers. Between them lies a remarkable palace-shaped space - the AXILLA - the Gateway Palace through which everything must pass.
Chapter 1: The Palace is Built (Shape and Location)
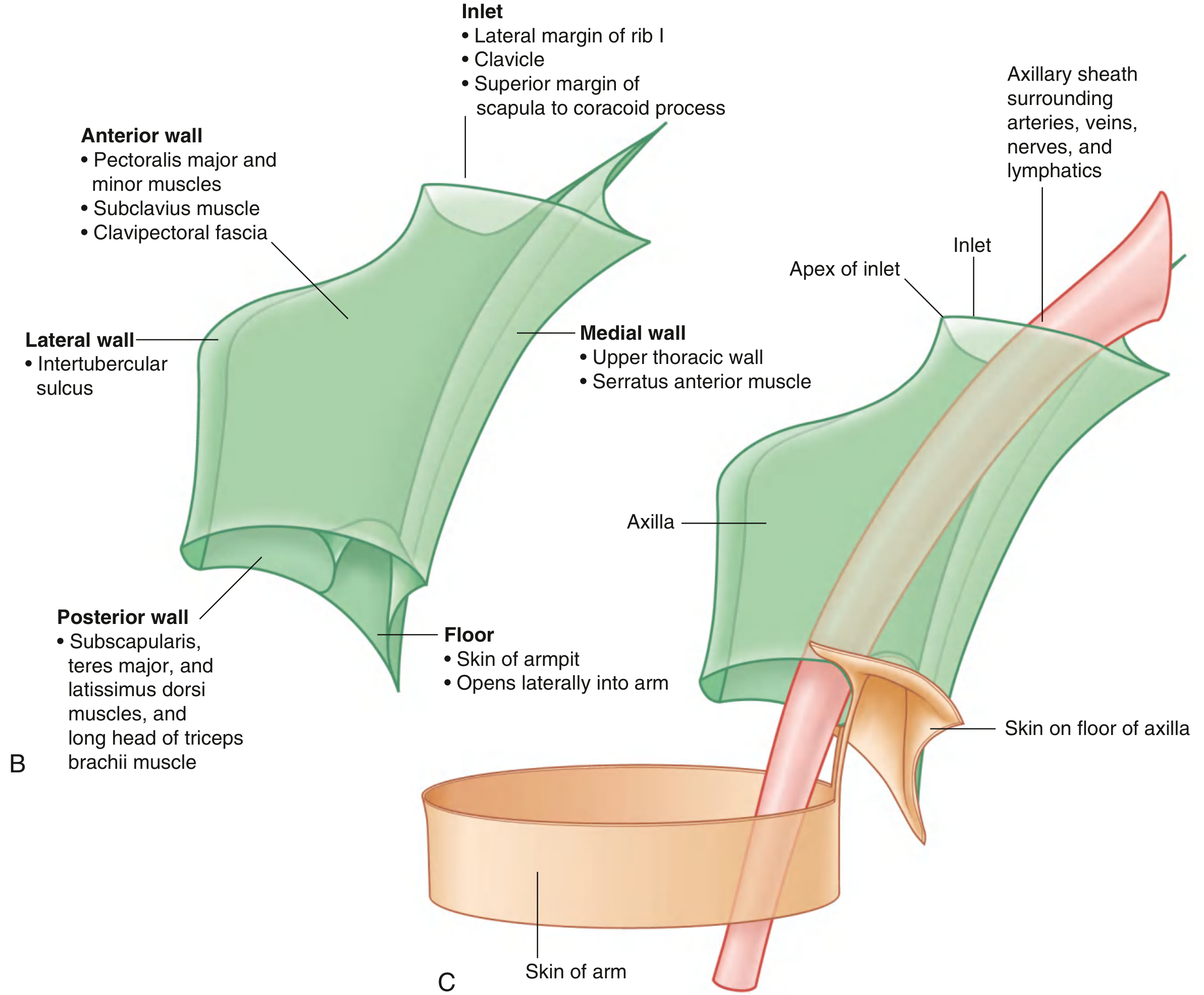
Once upon a time, the architect of the body decided to build a passage between the neck and the arm. The palace he designed was pyramidal - shaped like an upside-down pyramid with four walls, a grand doorway at the top (the inlet), and an open courtyard at the bottom (the floor).
The palace was made from the best materials:
- The clavicle formed the northern bridge
- The scapula formed the eastern wall frame
- The upper thoracic wall (ribs 1-4) formed the inner wall
- The humerus formed the outer pillar
And so the Axillary Palace was born.
Chapter 2: The Grand Entrance (The Axillary Inlet / Apex)
Every palace has a grand entrance. The Axillary Palace's gateway - the inlet (apex) - opens superiorly toward the neck, shaped like a triangle pointing sideways.
Its three borders are:
- Medial - the lateral border of Rib I (the gatepost)
- Anterior - the posterior surface of the clavicle (the front gate)
- Posterior - the superior border of the scapula up to the coracoid process (the back gate)
Through this triangular doorway, the subclavian artery enters and is immediately renamed the axillary artery as it crosses Rib I - like a diplomat receiving new credentials upon entering a new territory. The subclavian vein does the same in reverse when leaving. The brachial plexus trunks march in behind them. At the inlet, the vein is most anterior, the artery is in the middle, and the nerves are most posterior.
Chapter 3: The Four Palace Walls
🧱 The Front Wall (Anterior Wall) - The Chest Guards
The front wall of the palace is guarded by three loyal chest muscles standing in layers:
-
Pectoralis major - the chief guard, largest and most superficial. Its lower edge forms the anterior axillary fold (the front door curtain you can feel in your armpit). It flexes, adducts, and medially rotates the arm. Innervated by the lateral and medial pectoral nerves.
-
Pectoralis minor - the hidden lieutenant, deep to the major. It originates from ribs III-V and inserts on the coracoid process - pulling the tip of the shoulder down and protracting the scapula. This muscle is so important that the axillary artery is divided into three parts based on its position relative to it.
-
Subclavius - the small gatekeeper at the top, between the clavicle and rib I. It pulls the clavicle medially to stabilize the sternoclavicular joint.
The whole front wall is wrapped in the clavipectoral fascia - like the palace's front curtain wall.
🧱 The Inner Wall (Medial Wall) - The Ribcage Servants
The medial wall of the palace faces the chest. It is formed by:
- Ribs 1-4 and their intercostal muscles (the stone foundation)
- Serratus anterior muscle - the palace's inner wall servant, originating from the lateral surfaces of the upper 8-9 ribs and inserting on the costal (front) surface of the medial border of the scapula.
Serratus anterior is innervated by the long thoracic nerve (C5, C6, C7), which runs vertically down the medial wall like a power line on the outer surface of the muscle. Damage to this nerve causes the famous "winging of the scapula" - the scapula lifts off the back wall like a loose panel.
🧱 The Back Wall (Posterior Wall) - The Deep Fortress
The back wall is the most complex, with four muscular layers standing like a fortress:
-
Subscapularis - the front layer of the back wall, covering the costal surface of the scapula. A rotator cuff muscle that medially rotates the arm. Innervated by the upper and lower subscapular nerves.
-
Teres major - the lower layer, passing from the inferior angle of the scapula to the medial lip of the intertubercular sulcus. It adducts, medially rotates, and extends the arm. Innervated by the lower subscapular nerve.
-
Latissimus dorsi - swinging in from the back like a grand cape, passing from the thoracolumbar fascia and lower ribs to the floor of the intertubercular sulcus. The great adductor, medial rotator, and extensor. Innervated by the thoracodorsal nerve (C6, C7, C8).
-
Long head of triceps brachii - the vertical sentinel, passing straight down through the posterior wall.
This back wall has three important secret doorways (gateways):
| Gateway | Boundaries (from anterior view) | What passes through |
|---|---|---|
| Quadrangular Space | Subscapularis (sup), teres major (inf), long head triceps (medial), surgical neck humerus (lat) | Axillary nerve + posterior circumflex humeral artery |
| Triangular Space | Subscapularis (sup), teres major (inf), long head triceps (lat) | Circumflex scapular artery |
| Triangular Interval | Teres major (sup), long head triceps (medial), shaft of humerus (lat) | Radial nerve |
🧱 The Outer Wall (Lateral Wall) - The Humeral Pillar
The lateral wall is the narrowest, formed simply by the intertubercular sulcus (bicipital groove) of the humerus - the bony groove through which the tendons of the front wall muscles insert.
🪑 The Floor (Base) - The Courtyard
The floor of the palace is not a rigid floor but a hammock of fascia and skin (the dome of armpit skin) suspended between the inferior edges of the walls. It is supported by the clavipectoral fascia. The floor opens laterally into the arm where the palace is continuous with the anterior compartment of the arm.
Chapter 4: The Residents of the Palace (Contents)
Now the palace is built, but who lives inside it? The axilla contains a remarkable collection of important travelers:
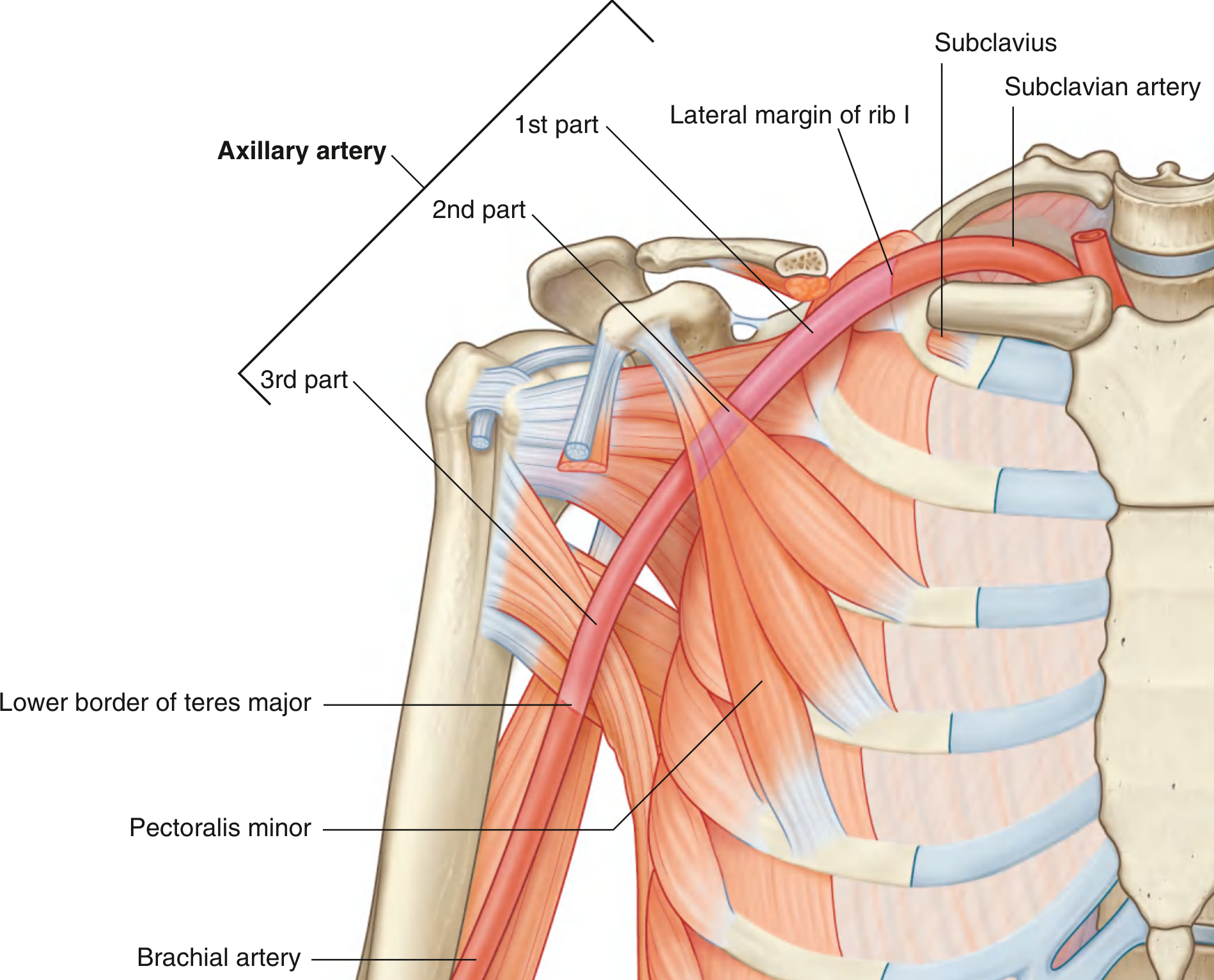
🔴 The Master Road: Axillary Artery
The axillary artery is the main highway through the palace - the subclavian artery renamed at the lateral border of Rib I, becoming the brachial artery at the inferior margin of teres major.
The pectoralis minor muscle divides it into three parts - like three toll zones on a highway:
Part 1 (proximal to pec minor) - 1 branch:
- Superior thoracic artery (supplies upper anterior/medial axillary walls)
Part 2 (behind pec minor) - 2 branches:
- Thoraco-acromial artery (4 branches: pectoral, deltoid, acromial, clavicular)
- Lateral thoracic artery (supplies breast, serratus anterior)
Part 3 (distal to pec minor) - 3 branches:
- Subscapular artery → circumflex scapular + thoracodorsal branches
- Anterior circumflex humeral artery
- Posterior circumflex humeral artery (passes through the quadrangular space)
Memory trick: 1 branch from part 1, 2 from part 2, 3 from part 3. (1-2-3 rule)
🔵 The Return Road: Axillary Vein
The axillary vein lies medial and anterior to the artery. It becomes the subclavian vein when it crosses Rib I heading home to the neck. Clinically important as the "subclavian route" for central venous access actually punctures the first part of the axillary vein.
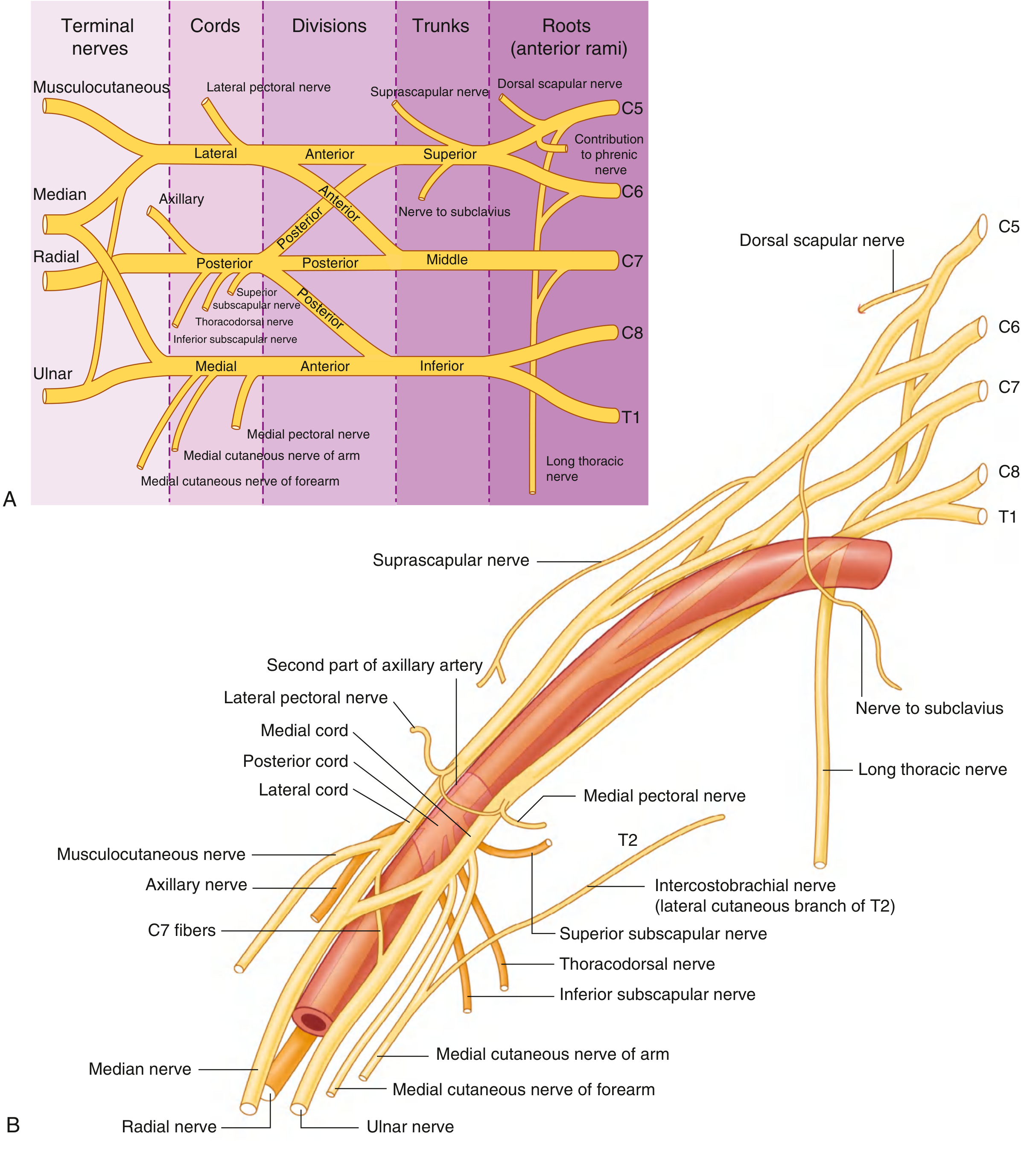
🟡 The Messenger Network: Brachial Plexus
The brachial plexus is the palace's communication system - five nerve roots (C5-T1) entering from the neck and organizing into a sophisticated network:
Route: Roots → Trunks → Divisions → Cords → Terminal Branches
The cords are named by their position relative to the axillary artery's second part:
- Lateral cord (C5, C6, C7)
- Medial cord (C8, T1)
- Posterior cord (C5-T1)
The terminal branches form an "M" shape over the third part of the axillary artery:
- Musculocutaneous (lateral cord)
- Lateral root of median nerve (lateral cord)
- Median nerve (both cords meet)
- Medial root of median nerve (medial cord)
- Ulnar nerve (medial cord)
And from the posterior cord:
- Superior subscapular nerve → subscapularis
- Thoracodorsal nerve → latissimus dorsi
- Inferior subscapular nerve → subscapularis + teres major
- Axillary nerve → through quadrangular space → deltoid + teres minor
- Radial nerve → through triangular interval → posterior arm
🟢 The Lymphatic Guards: Axillary Lymph Nodes
The palace has five groups of guards (lymph node groups) arranged around its walls:
| Group | Location | Drains |
|---|---|---|
| Anterior (pectoral) | Along lateral thoracic vessels, anterior wall | Breast, anterior chest wall |
| Posterior (subscapular) | Along subscapular vessels, posterior wall | Back, posterior shoulder |
| Lateral (humeral) | Along the axillary vein, lateral wall | Upper limb |
| Central | Embedded in axillary fat | Receives from above 3 groups |
| Apical | Near axillary inlet along medial wall | Everything - drains to subclavian trunk |
All ultimately drain to the apical nodes, then into the subclavian lymphatic trunk.
🏋️ The Visiting Muscles
Two muscles pass through the palace on their way to work in the arm:
- Biceps brachii - both heads (long head in the intertubercular sulcus, short head from coracoid process) pass through the axilla before joining in the arm
- Coracobrachialis - passes through, being pierced by the musculocutaneous nerve in the process
Chapter 5: The Palace Wraps Up (The Axillary Sheath)
All the major residents - arteries, veins, and the brachial plexus cords - travel together wrapped in a sleeve of fascia called the axillary sheath. This sheath is a continuation of the prevertebral fascia from the neck. It keeps the important passengers together for their journey, allowing regional anesthesia (the "brachial plexus block") to be administered into the sheath space.
And so the Axillary Palace stands - an architectural wonder connecting the neck to the arm, housing the most important highways, communication cables, and drainage systems of the upper limb. Every surgeon who reaches into it, every physiotherapist who treats it, and every student who studies it is walking through the same gateway built by millions of years of evolution.
📋 STRUCTURED NOTES: ANATOMY OF THE AXILLA
Source: Gray's Anatomy for Students, 4th Ed.
1. DEFINITION & SHAPE
- The axilla is a pyramidal space between the neck and the arm
- Has 4 walls + 1 inlet (apex) + 1 floor (base)
- All major neurovasculature of the upper limb passes through it
2. BOUNDARIES
Inlet (Apex)
- Medial - lateral border of Rib I
- Anterior - posterior surface of clavicle
- Posterior - superior border of scapula to coracoid process
- Apex points laterally toward coracoid process
Anterior Wall
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Pectoralis major | Medial clavicle + sternum + ribs 1-6 | Lateral lip of intertubercular sulcus | Medial + lateral pectoral (C5-T1) | Flexion, adduction, medial rotation |
| Pectoralis minor | Ribs III-V | Coracoid process | Medial + lateral pectoral (C5-T1) | Depresses shoulder, protracts scapula |
| Subclavius | Rib I - costal cartilage junction | Inferior surface of clavicle (middle 1/3) | Nerve to subclavius (C5, C6) | Depresses clavicle, stabilizes SC joint |
- Covered by clavipectoral fascia
- Anterior axillary fold = inferior margin of pectoralis major
Medial Wall
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Serratus anterior | Lateral surfaces of ribs 1-8/9 | Costal surface of medial border of scapula | Long thoracic nerve (C5, C6, C7) | Protracts + rotates scapula upward |
- Ribs 1-4 + intercostals also contribute
- Winging of scapula = long thoracic nerve damage
Posterior Wall
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Subscapularis | Medial 2/3 of subscapular fossa | Lesser tubercle of humerus | Upper + lower subscapular (C5, C6) | Medial rotation (rotator cuff) |
| Teres major | Posterior surface, inferior angle of scapula | Medial lip of intertubercular sulcus | Lower subscapular (C5, C6, C7) | Adduction, medial rotation, extension |
| Latissimus dorsi | Spinous processes T7-L5, iliac crest, lower ribs | Floor of intertubercular sulcus | Thoracodorsal (C6, C7, C8) | Adduction, medial rotation, extension |
| Long head of triceps | Infraglenoid tubercle of scapula | Olecranon (via common tendon) | Radial nerve (C6-C8) | Extension of elbow |
Lateral Wall
- Intertubercular sulcus (bicipital groove) of the humerus
- Narrowest wall
- Insertions of pec major (lateral lip), teres major (medial lip), latissimus dorsi (floor)
Floor (Base)
- Formed by fascia + dome of skin of the armpit
- Supported by clavipectoral fascia
- Opens laterally into the arm
3. POSTERIOR WALL GATEWAYS
| Space | Boundaries | Contents |
|---|---|---|
| Quadrangular space | Subscapularis (sup), teres major (inf), long head triceps (med), surgical neck humerus (lat) | Axillary nerve + posterior circumflex humeral artery/vein |
| Triangular space | Subscapularis (sup), teres major (inf), long head triceps (lat) | Circumflex scapular artery/vein |
| Triangular interval | Teres major (sup), long head triceps (med), humerus (lat) | Radial nerve |
4. AXILLARY ARTERY
Subclavian A → crosses lateral border of Rib I → Axillary A → crosses lower border of teres major → Brachial A
3 parts divided by pectoralis minor:
| Part | Relation to pec minor | Branches (mnemonic: 1-2-3) |
|---|---|---|
| 1st | Proximal to | 1 branch: Superior thoracic A |
| 2nd | Posterior to | 2 branches: Thoraco-acromial A, Lateral thoracic A |
| 3rd | Distal to | 3 branches: Subscapular A, Anterior circumflex humeral A, Posterior circumflex humeral A |
- Thoraco-acromial has 4 branches: pectoral, deltoid, acromial, clavicular
- Subscapular A = largest branch → divides into circumflex scapular + thoracodorsal
5. AXILLARY VEIN
- Lies medial and anterior to the axillary artery
- Becomes subclavian vein at lateral margin of Rib I
- Clinical access point: "subclavian route" actually punctures first part of axillary vein
- Puncture should be at midclavicular line or lateral to it
6. BRACHIAL PLEXUS
Roots → Trunks → Divisions → Cords → Branches
| Root levels | C5, C6, C7, C8, T1 |
|---|
Trunks (in neck):
- Superior trunk (C5, C6) - branches: suprascapular nerve + nerve to subclavius
- Middle trunk (C7)
- Inferior trunk (C8, T1)
Cords (named by position relative to 2nd part axillary artery):
- Lateral cord (C5, C6, C7)
- Medial cord (C8, T1)
- Posterior cord (C5-T1)
Branches of cords:
Lateral cord branches:
- Lateral pectoral nerve → pec major
- Musculocutaneous nerve (C5-C7) → pierces coracobrachialis → all anterior arm muscles
- Lateral root of median nerve
Medial cord branches:
- Medial pectoral nerve → pec major + minor
- Medial cutaneous nerve of arm (C8, T1)
- Medial cutaneous nerve of forearm
- Medial root of median nerve
- Ulnar nerve (C8, T1)
Posterior cord branches (in order):
- Superior subscapular nerve → subscapularis
- Thoracodorsal nerve (C6, C7, C8) → latissimus dorsi
- Inferior subscapular nerve (C5, C6) → subscapularis + teres major
- Axillary nerve (C5, C6) → through quadrangular space → deltoid + teres minor
- Radial nerve (C5-C8, T1) → through triangular interval → posterior arm/forearm
"M" pattern over 3rd part of axillary artery:
Musculocutaneous - Lateral root of median - Median nerve - Medial root of median - Ulnar
7. AXILLARY LYMPH NODES (5 Groups)
| Group | Position | Drains |
|---|---|---|
| Anterior (Pectoral) | Along lateral thoracic vessels | Breast, anterior chest wall |
| Posterior (Subscapular) | Along subscapular vessels | Back, posterior shoulder |
| Lateral (Humeral) | Along axillary vein | Upper limb |
| Central | Central axillary fat | Receives from above 3 groups |
| Apical | Medial wall, axillary inlet | All groups → subclavian lymphatic trunk |
- Clinically significant in breast cancer staging (sentinel lymph node biopsy)
8. MUSCLES PASSING THROUGH AXILLA
| Muscle | Parts in axilla | Nerve | Key clinical note |
|---|---|---|---|
| Biceps brachii | Long head (in intertubercular sulcus) + short head | Musculocutaneous (C5, C6) | Long head prevents superior humeral migration |
| Coracobrachialis | Passes through axilla to mid-humerus | Musculocutaneous (C5, C6, C7) - pierces it | Musculocutaneous nerve can be found by locating this muscle |
9. AXILLARY SHEATH
- Fascial sleeve derived from prevertebral fascia of the neck
- Surrounds axillary artery, vein, and cords of brachial plexus
- Basis for brachial plexus nerve blocks (local anesthetic injected into sheath)
10. CLINICAL PEARLS
| Scenario | Structure at risk | Mechanism |
|---|---|---|
| Anterior shoulder dislocation | Axillary nerve (quadrangular space) | Stretching at surgical neck |
| Anterior dislocation | Axillary artery | Compression by dislocated humeral head |
| Fracture of rib I | Subclavian/1st part axillary artery | Direct trauma |
| Mastectomy/axillary clearance | Thoracodorsal nerve, long thoracic nerve | Surgical dissection |
| Long thoracic nerve injury | Winging of scapula | Serratus anterior paralysis |
| "Crutch palsy" | Radial nerve in axilla | Compression at triangular interval |
| Axillary vein catheterization | Pneumothorax | Needle too medial (enters pleura) |
All content sourced from Gray's Anatomy for Students, 4th Edition - Upper Limb chapter, pp. 841-865
This is a shared conversation. Sign in to Orris to start your own chat.