Diuretics pharmacology in details
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
diuretics mechanism of action nephron site
Reading File
Loading Image
Loading Image
Reading File
Searching Images
carbonic anhydrase inhibitor proximal tubule collecting duct aldosterone diuretic
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Goodman & Gilman's across all diuretic classes. Let me compile the complete, detailed pharmacology answer:
Diuretics: Detailed Pharmacology
Overview
Diuretics increase the rate of urine flow and Na⁺ excretion and are used to adjust the volume or composition of body fluids. The kidney filters ~120 mL of plasma/min (≈180 L/day), reabsorbing >99% of glomerular ultrafiltrate. Diuretics exploit the specific transport proteins distributed along the nephron to selectively inhibit sodium reabsorption at different tubular segments.
Three cardinal principles (Goodman & Gilman's):
- Transport of solute across renal epithelial cells involves highly specialized apical and basolateral membrane proteins.
- Diuretics target and block these transport proteins.
- The site and class of diuretic action are determined by which specific protein is inhibited.
Master Diagram — Sites of Action
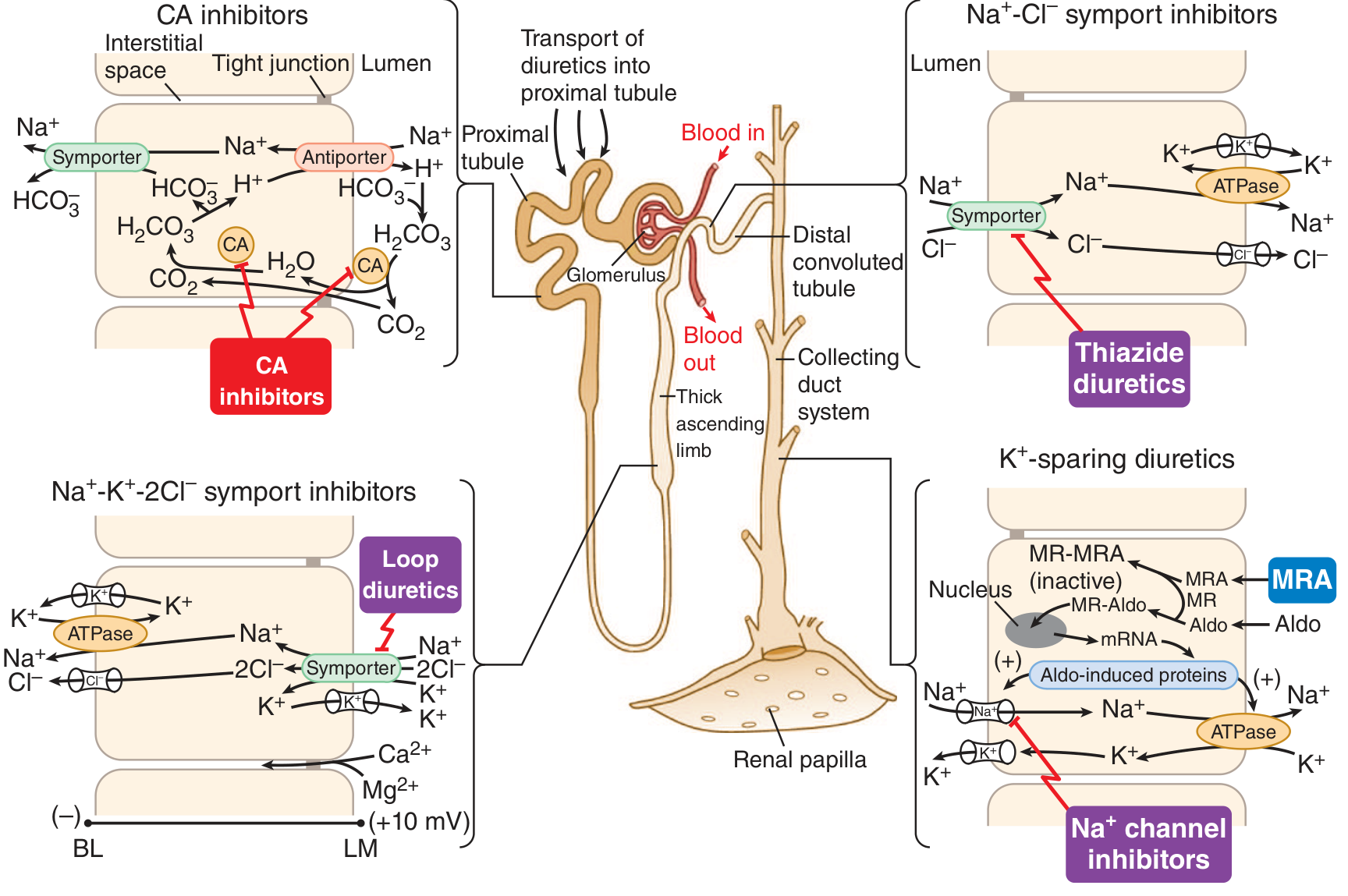
Class 1: Carbonic Anhydrase Inhibitors (CAIs)
Site
Proximal tubule (luminal and cytoplasmic carbonic anhydrase)
Mechanism
In the proximal tubule, CO₂ diffuses into epithelial cells and reacts with water — catalyzed by carbonic anhydrase — to form H₂CO₃, which dissociates into H⁺ and HCO₃⁻. H⁺ is secreted into the lumen via the Na⁺-H⁺ antiporter, allowing NaHCO₃ reabsorption. CAIs block both membrane-bound and cytoplasmic carbonic anhydrase, suppressing H⁺ secretion, thereby inhibiting Na⁺-H⁺ exchange and NaHCO₃ reabsorption.
Drugs & Pharmacokinetics
| Drug | Relative Potency | Oral Bioavailability | t½ (h) | Elimination |
|---|---|---|---|---|
| Acetazolamide | 1 | ~100% | 6–9 | Renal |
| Dichlorphenamide | 30 | ID | ID | ID |
| Methazolamide | >1; <10 | ~100% | ~14 | 25% R, 75% M |
Urinary Effects
- ↑↑ HCO₃⁻ excretion (up to 35% of filtered load)
- ↑ Na⁺, K⁺, H₂PO₄⁻ excretion
- Urine pH rises to ~8 → metabolic acidosis (self-limiting due to decreased filtered HCO₃⁻ load)
- Fractional excretion of Na⁺ up to 5%; K⁺ up to 70%
Extrarenal Actions
- Eye: Inhibit CA in ciliary processes → ↓ aqueous humor formation → ↓ intraocular pressure
- CNS: Anticonvulsant effects (direct CNS action + metabolic acidosis)
- Erythrocytes: ↑ CO₂ in peripheral tissues
- Vasodilation via Ca²⁺-activated K⁺ channels
Clinical Uses
- Open-angle glaucoma (dorzolamide, brinzolamide — topical; acetazolamide — oral)
- Acute-angle closure glaucoma (preoperative IOP reduction)
- Absence seizures (acetazolamide)
- High-altitude sickness (mountain sickness)
- Familial periodic paralysis
- Augmenting loop/thiazide diuretics in severe diuretic resistance
Adverse Effects
- Metabolic acidosis (dose-limiting)
- Hypokalemia, paresthesias, somnolence, renal stones (alkaline urine precipitates calcium phosphate)
- Sulfonamide hypersensitivity reactions
Class 2: Osmotic Diuretics
Site
Proximal tubule and loop of Henle (descending thin limb primarily)
Mechanism
Freely filtered but non-reabsorbable solutes raise luminal osmolality, opposing water reabsorption in the proximal tubule. They also expand extracellular fluid volume, decrease blood viscosity, inhibit renin release, and increase renal medullary blood flow — washing out NaCl and urea from the medullary interstitium (reduces medullary tonicity) → limits passive NaCl reabsorption in the ascending thin limb. Inhibit Mg²⁺ reabsorption in the TAL.
Drugs
- Mannitol (IV only) — most commonly used
- Glycerin, Isosorbide (oral)
- Urea (IV only)
Urinary Effects
Increase excretion of nearly all electrolytes: Na⁺, K⁺, Ca²⁺, Mg²⁺, Cl⁻, HCO₃⁻, phosphate
Clinical Uses
- Dialysis disequilibrium syndrome
- ↓ Intraocular pressure (acute glaucoma, perioperative)
- ↓ Intracranial pressure (traumatic brain injury, cerebral edema)
- Cystic fibrosis (inhaled mannitol — improves mucus clearance)
- Diagnosis of bronchial hyperreactivity
Adverse Effects
- Initial volume expansion (dangerous in heart failure)
- Dehydration and hypernatremia (if water replacement is inadequate)
- Headache, nausea, vomiting
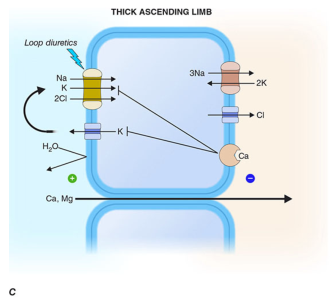
Class 3: Loop Diuretics (High-Ceiling Diuretics)
Site
Thick ascending limb (TAL) of the loop of Henle
Mechanism
Inhibit the Na⁺-K⁺-2Cl⁻ (NKCC2) symporter on the apical membrane of TAL cells — bringing salt transport in this segment to a virtual standstill. The drug attaches to the Cl⁻ binding site in the symporter's transmembrane domain. Blockade of NKCC2:
- Eliminates the lumen-positive transepithelial potential difference normally created by K⁺ recycling back into the lumen
- This positive luminal potential drives passive paracellular reabsorption of Ca²⁺ and Mg²⁺ → both are markedly increased in urine
- Abolishes the medullary concentration gradient → impairs both diluting and concentrating ability
Why loop diuretics are highly efficacious: TAL normally reabsorbs ~25% of filtered Na⁺, and nephron segments distal to the TAL cannot rescue the flood of unabsorbed material, unlike the proximal tubule where the TAL compensates.
Drugs & Pharmacokinetics
| Drug | Relative Potency | Oral Bioavailability | t½ (h) | Elimination |
|---|---|---|---|---|
| Furosemide | 1 | ~60% | ~1.5 | 65% R, 35% M |
| Bumetanide | 40× | ~80% | ~0.8 | 62% R, 38% M |
| Torsemide | 3× | ~80% | ~3.5 | 20% R, 80% M |
| Ethacrynic acid | 0.7× | ~100% | ~1 | 67% R, 33% M |
- Furosemide and bumetanide: sulfonamide moiety
- Ethacrynic acid: phenoxyacetic acid derivative (only non-sulfonamide — use in sulfonamide allergy)
- Torsemide: sulfonylurea — longest half-life, mostly hepatic metabolism (preferred in liver disease)
- All secreted into the proximal tubule via OAT1/OAT3 on basolateral membrane → require tubular secretion to reach their site of action
Urinary Effects
- ↑↑ Na⁺, Cl⁻, K⁺, H⁺, Ca²⁺, Mg²⁺, HCO₃⁻
- Fractional Na⁺ excretion can reach 20–25%
- Produce dilute urine (abolish medullary gradient)
Additional Pharmacological Effects
- Venodilation: Furosemide increases venous capacitance within minutes of IV injection (before significant diuresis) — PGE₂ and NO mediated — beneficial in acute pulmonary edema
- ↑ Renal blood flow acutely (via PGs)
- May activate renin–angiotensin–aldosterone system with prolonged use
Clinical Uses
- Acute pulmonary edema (IV furosemide — immediate venodilation, then diuresis)
- Chronic heart failure — volume overload
- Hypertensive urgency/emergency
- Hypercalcemia (with IV saline infusion)
- Acute kidney injury — (to maintain urine output, though benefit unproven)
- Nephrotic syndrome, cirrhosis (with aldosterone antagonist)
- Forced diuresis for drug overdose
Adverse Effects
- Hypokalemia (most common) → metabolic alkalosis
- Hypomagnesemia
- Hypocalcemia (chronic use)
- Ototoxicity — dose-dependent, reversible (especially with rapid IV infusion or in renal failure; worst with ethacrynic acid — may be irreversible)
- Hyperuricemia (competes with uric acid for tubular secretion; also volume contraction → uric acid reabsorption)
- Hyperglycemia (less than thiazides)
- Hypovolemia, hypotension, pre-renal azotemia
- Sulfonamide allergy cross-reactivity (furosemide, bumetanide)
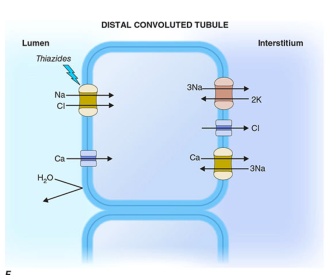
Class 4: Thiazide Diuretics
Site
Distal convoluted tubule (DCT) — cortical diluting segment
Mechanism
Inhibit the Na⁺-Cl⁻ cotransporter (NCC/SLC12A3) on the apical membrane of DCT cells. This reduces Na⁺ and Cl⁻ reabsorption. The lower intracellular Na⁺ concentration enhances the basolateral Na⁺-Ca²⁺ exchanger and increases apical Ca²⁺ channel expression → hypocalciuria (thiazides reduce urinary Ca²⁺). The DCT is not involved in generating the medullary concentration gradient, so thiazides do not impair urine concentration (unlike loop diuretics).
Drugs & Key Pharmacokinetics
- Hydrochlorothiazide (HCTZ): most prescribed (though evidence favors chlorthalidone)
- Chlorthalidone: longer t½ (~40–60 h vs. 6–15 h for HCTZ) → better 24-h BP control
- Indapamide: thiazide-like; also has direct vasodilatory effects
- Metolazone: effective even at GFR <30 mL/min (synergistic with loop diuretics)
- All secreted into the proximal tubule via OAT1/OAT3 and MRP-4
Urinary Effects
- ↑ Na⁺, Cl⁻, K⁺, H⁺, HCO₃⁻
- ↓ Ca²⁺ excretion (unique among diuretics)
- Mild ↑ Mg²⁺ excretion (hypomagnesemia with long-term use)
- Attenuates ability to produce dilute urine; does NOT impair concentrating ability
Clinical Uses
- Hypertension — first-line; additive/synergistic with most antihypertensives. Chlorthalidone preferred over HCTZ for cardiovascular outcomes
- Edema — heart failure, cirrhosis, nephrotic syndrome (less potent than loop diuretics; ineffective if GFR <30 mL/min, except metolazone/indapamide)
- Nephrolithiasis (calcium stones) — ↓ urinary Ca²⁺ excretion
- Osteoporosis — reduction in urinary calcium loss
- Nephrogenic diabetes insipidus — paradoxically ↓ urine volume by ~50% (mild volume depletion → compensatory proximal Na⁺ reabsorption → less water reaches collecting duct)
Adverse Effects
- Hypokalemia → metabolic alkalosis (dose-dependent)
- Hypomagnesemia (especially elderly)
- Hyperuricemia → gout precipitation
- Hyperglycemia (↓ insulin secretion, ↑ insulin resistance) — avoid in diabetes
- Hyperlipidemia (mild — ↑ LDL, ↑ triglycerides; less with indapamide)
- Hypercalcemia (due to ↓ urinary Ca²⁺; may precipitate in hyperparathyroidism)
- Hyponatremia (elderly women at highest risk — thiazide impairs free water excretion)
- Erectile dysfunction
- Sulfonamide allergy cross-reactivity
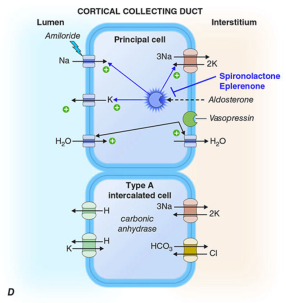
Class 5: Potassium-Sparing Diuretics
5A: ENaC Blockers (Na⁺ Channel Inhibitors)
Site
Late distal tubule and collecting duct (cortical collecting duct)
Mechanism
Amiloride and triamterene directly block the epithelial Na⁺ channel (ENaC) on the apical membrane of principal cells. ENaC blockade:
- Hyperpolarizes the luminal membrane
- Reduces the lumen-negative transepithelial potential
- ↓ K⁺, H⁺, Ca²⁺, Mg²⁺ secretion → these are retained
| Drug | Relative Potency | Oral Bioavailability | t½ (h) | Elimination |
|---|---|---|---|---|
| Amiloride | 1 | 15–25% | ~21 | Renal (intact) |
| Triamterene | 0.1 | ~50% | ~4 | Hepatic (active metabolite → renal) |
Urinary Effects
Mild natriuresis only (~2% of filtered Na⁺); significant K⁺ retention
Clinical Uses
- Combined with thiazide or loop diuretics to prevent hypokalemia
- Liddle syndrome (constitutive ENaC activation → hypertension + hypokalemia)
- Amiloride inhaled — cystic fibrosis (improves mucociliary clearance)
- Amiloride — lithium-induced nephrogenic DI (blocks Li⁺ transport into collecting duct cells)
Adverse Effects
- Hyperkalemia (life-threatening — most important adverse effect)
- Contraindicated: renal failure, concurrent ACEi/ARB/K⁺ supplements, other K⁺-sparing diuretics
- Triamterene: weak folic acid antagonist (megaloblastosis in cirrhotics), renal stones, interstitial nephritis
5B: Mineralocorticoid Receptor Antagonists (Aldosterone Antagonists)
Site
Late distal tubule and collecting duct (cortical collecting duct) — act on cytosolic mineralocorticoid receptor (MR)
Mechanism
Aldosterone binds cytosolic MR → MR-aldosterone complex translocates to nucleus → transcription of aldosterone-induced proteins (AIPs) → upregulation of ENaC, Na⁺/K⁺-ATPase → ↑ Na⁺ reabsorption + ↑ K⁺/H⁺ secretion.
MR antagonists (spironolactone, eplerenone, finerenone) competitively inhibit aldosterone binding → MR-antagonist complex cannot induce AIP synthesis → no ENaC upregulation.
Key distinction: MR antagonists are the only diuretics that do NOT require access to the tubular lumen to induce diuresis — they act on a cytosolic receptor.
| Drug | Oral Bioavailability | t½ (h) | Elimination | Notes |
|---|---|---|---|---|
| Spironolactone | ~65% | ~1.6 (active metabolites: 10–35 h) | Hepatic | Steroidal; anti-androgenic |
| Eplerenone | — | ~5 | Hepatic | Steroidal; selective (fewer sex-hormone effects) |
| Finerenone | — | ~3 | Hepatic | Non-steroidal MR antagonist (FDA approved 2021) |
Clinical Uses
- Primary hyperaldosteronism (Conn's syndrome) — diagnosis and treatment
- Heart failure (HFrEF) — spironolactone/eplerenone reduce mortality (RALES, EMPHASIS-HF trials)
- Cirrhosis with ascites — first-line (with furosemide)
- Resistant hypertension — add-on therapy
- Spironolactone: PCOS, hirsutism, acne (anti-androgenic)
- Finerenone: CKD with type 2 diabetes (reduces CKD progression and cardiovascular events — FIDELIO-DKD, FIGARO-DKD)
Adverse Effects
- Hyperkalemia (most dangerous — monitor K⁺ closely)
- Spironolactone (anti-androgenic/progestogenic): gynecomastia, menstrual irregularities, impotence, decreased libido (less with eplerenone/finerenone)
- Metabolic acidosis (type IV RTA)
- GI upset (spironolactone)
Class 6: SGLT2 Inhibitors (Gliflozins) — Emerging Diuretic Class
Site
Proximal tubule (S1–S2 segment)
Mechanism
Inhibit sodium-glucose cotransporter 2 (SGLT2), which normally reabsorbs ~90% of filtered glucose (linked with Na⁺ reabsorption). This produces glucosuria and osmotic natriuresis. They also cause tubuloglomerular feedback (TGF) restoration — increased NaCl delivery to macula densa reduces hyperfiltration.
Clinical Uses
- Type 2 diabetes (primary indication)
- Heart failure (HFrEF and HFpEF) — reduce CV mortality and HF hospitalization
- CKD — slow progression, reduce end-stage renal disease
- Overcome diuretic resistance (sequential nephron blockade combined with loop diuretics)
Adverse Effects
- Urogenital infections (mycotic, UTIs)
- DKA (rare, including euglycemic DKA)
- Bone fractures, ↓ bone density
- Hyperkalemia, hypovolemia, hypotension
- Contraindicated in severe renal impairment / ESRD
Summary Table: Diuretic Classes at a Glance
| Class | Site | Transporter Blocked | Na⁺ Effect | K⁺ Effect | Ca²⁺ Effect | Key Use | Key Toxicity |
|---|---|---|---|---|---|---|---|
| CA inhibitors | PCT | Carbonic anhydrase | ++ | ↑ loss | NC | Glaucoma, altitude sickness | Metabolic acidosis |
| Osmotic | PCT/LoH | None (osmotic) | ++ | ↑ loss | ↑ loss | ↑ ICP, IOP | Volume overload |
| Loop | TAL | NKCC2 | ++++ | ↑↑ loss | ↑↑ loss | Acute pulm edema, HF, hypercalcemia | Hypokalemia, ototoxicity |
| Thiazide | DCT | NCC | ++ | ↑ loss | ↓ loss | HTN, Ca-stones, nephrogenic DI | Hypokalemia, hyperuricemia, hyperglycemia |
| ENaC blockers | CCD | ENaC | + | ↓ (sparing) | ↓ | K⁺ conservation adjunct | Hyperkalemia |
| MR antagonists | CCD | Mineralocorticoid receptor | + | ↓ (sparing) | — | HF, cirrhosis, Conn's | Hyperkalemia, gynecomastia |
| SGLT2 inhibitors | PCT | SGLT2 | + | ↓ (mild) | — | DM2, HF, CKD | UTI, DKA |
Diuretic Resistance
Occurs when patients fail to respond adequately to diuretic therapy. Key mechanisms include:
- ↓ Oral bioavailability (gut edema in HF impairs furosemide absorption — switch to IV or torsemide/bumetanide)
- Impaired apical drug delivery — albumin binding of furosemide in nephrotic syndrome (→ use bumetanide, which is less protein-bound)
- Braking phenomenon — compensatory upregulation of proximal tubule transporters between doses
- Distal tubular remodeling — chronic loop diuretic use hypertrophies DCT/CCD cells → more NaCl reabsorption distally
Management: IV administration, continuous infusion, sequential nephron blockade (loop + thiazide + SGLT2i), dietary sodium restriction, correct RAAS activation, treat underlying cause.
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed.; Harrison's Principles of Internal Medicine, 21st ed.; Guyton & Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.